4849
Pre-operative prediction of cerebral hemodynamics for cognitive dysfunction in adults with Moyamoya Disease based on 3D-pCASL and radiomics1Department of Medical Imaging Center, Nanfang Hospital, Southern Medical University, Guangzhou, China, 2Philips Healthcare, Guangzhou, China, 3Department of Research & Development, Yizhun Medical AI Co. Ltd, Beijing, China
Synopsis
Keywords: Diagnosis/Prediction, Arterial spin labelling, Moyamoya disease
Motivation: Cognitive function in adult patients with moyamoya disease (MMD) is often impaired because of low cerebral perfusion.
Goal(s): To identify brain regions where low CBF is associated with cognitive dysfunction and assess the predictive performance of radiomics models for cognitive dysfunction in adults MMD.
Approach: 3D-pCASL and logistic regression analysis was employed to quantify CBF and explore independent predictors for preoperative cognitive dysfunction. And five different classifiers were used to establish radiomics models.
Results: Cerebral perfusion in the left LOFL, left IPL, left SMA, and left ACG showed significant associations with cognitive impairment. The final combined model had the best predictive performance.
Impact: Hypoperfusion on 3D-pCASL plays a crucial role in the detection of early cognitive impairment in adults with MMD, and the combined model that combined with CBF and radiomics features of specific brain regions showed better performance in predicting cognitive dysfunction.
Introduction
Moyamoya disease (MMD) is a relatively rare, chronic occlusive cerebrovascular disease with unknown etiology1. With the reduction of cerebral blood flow (CBF), the brain microstructural integrity and cognitive performance are altered in adult MMD2. Approximately 1/3–2/3 of patients may experience varying degrees of cognitive dysfunction, affecting quality of life and emotions3,4. Arterial spin labeling (ASL) is a magnetic resonance perfusion imaging technique that quantifies CBF by using magnetically labeled arterial water as an endogenous tracer. Compared with traditional magnetic resonance technology, ASL has been increasingly applied in various cerebrovascular disease screenings as a non-invasive examination technique without the need for injection of exogenous drugs5-7. The aim of this three-dimensional pseudo-continuous arterial spin labeling (3D-pCASL) based radiomics study was to identify brain regions in which low cerebral blood perfusion is associated with cognitive dysfunction, and to assess the performance of radiomics models in predicting the development of cognitive dysfunction in adult patients with MMD.Methods
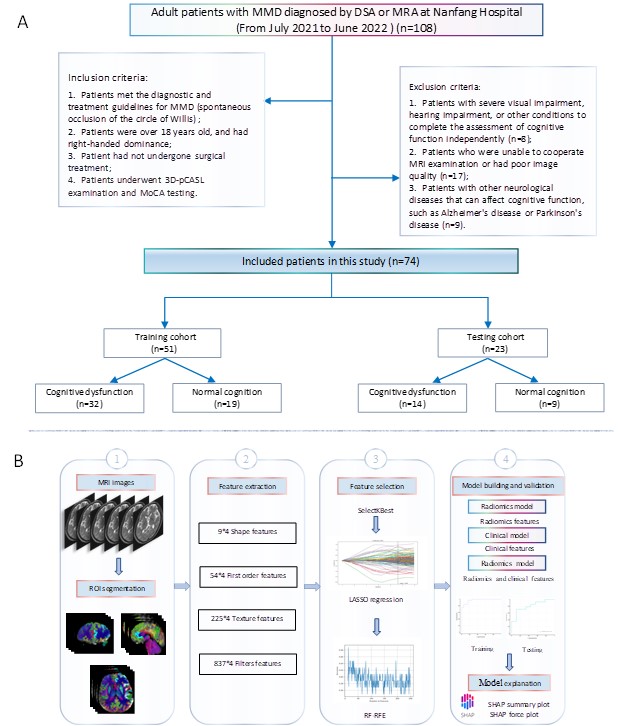
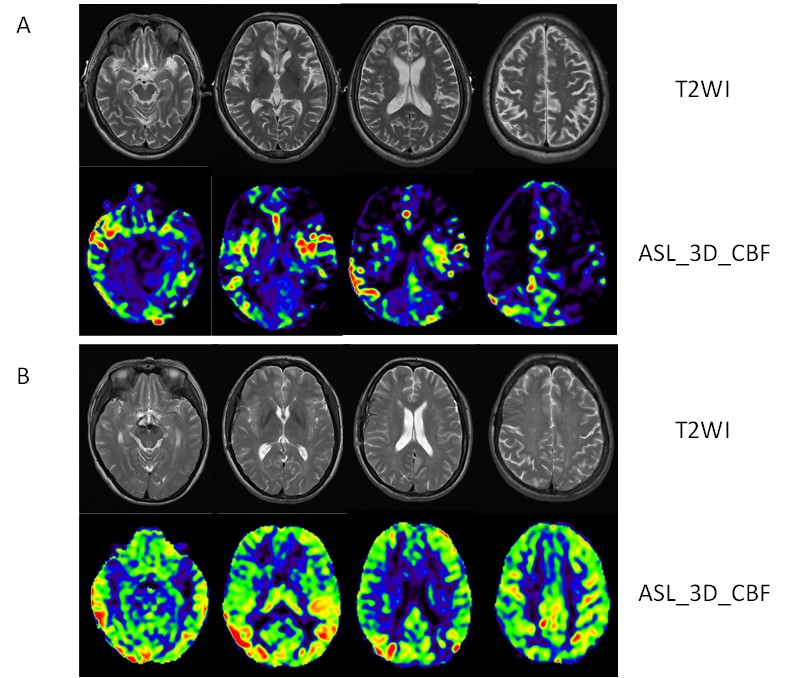
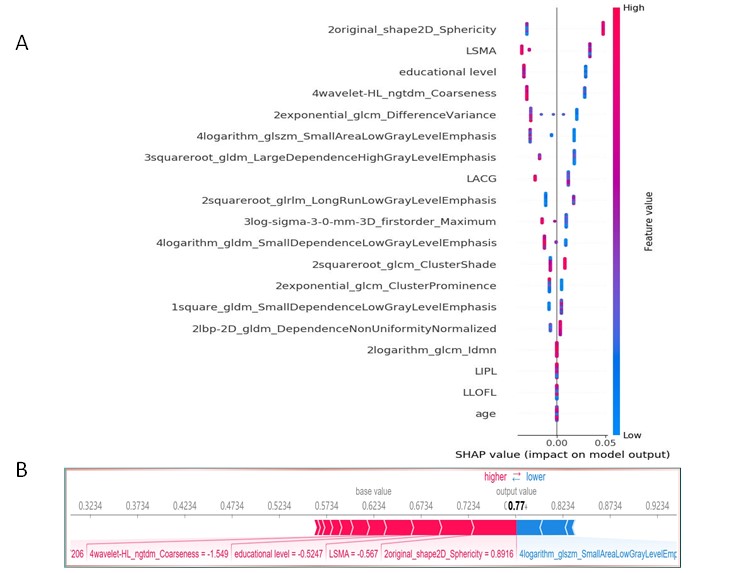
Seventy-four adult patients with MMD diagnosed by DSA or MRA in our hospital were prospectively collected. The Montreal Cognitive Assessment Scale (MoCA) was utilized to assess the cognitive function of the patients and classify them into a normal cognitive function group and a cognitive dysfunction group. All subjects underwent 3D-pCASL examination on a 3.0 T MRI scanner (uMR 780, United Imaging Healthcare, Shanghai, China). The bilateral lateral orbitofrontal lobe (LOFL), anterior cingulate gyrus (ACG), supplementary motor area (SMA), superior temporal gyrus (STG), insula, precuneus (PCu), and inferior parietal lobule (IPL) bilaterally were selected as the regions of interest (ROI), and CBF values were measured in each brain region. Multifactorial logistic regression analysis was employed to identify independent risk factors that affect cognitive function in adult MMD and construct a clinical model. After image resampling and bias correction, radiomics features were extracted from statistically significant brain regions for further analysis. The Intraclass correlation coefficients (ICCs) were used to quantify the reproducibility of the extracted radiomics features. The least absolute shrinkage and selection operator (LASSO) and random forest based recursive feature elimination (RFE-RF) methods were applied for feature selection and dimension reduction. Five different classifiers were used to establish radiomics models, including random forest, support vector machine, logistic regression, XGBoost, and k-nearest neighbor. The diagnostic performance of clinical, radiomics, and combined models that incorporate radiomics and clinical features in predicting cognitive dysfunction in adult MMD patients was assessed using ROC analysis, decision curve analysis (DCA) and calibration curves. The SHapley Additive exPlanations (SHAP) method was utilized to interpret and visualize model results.Results
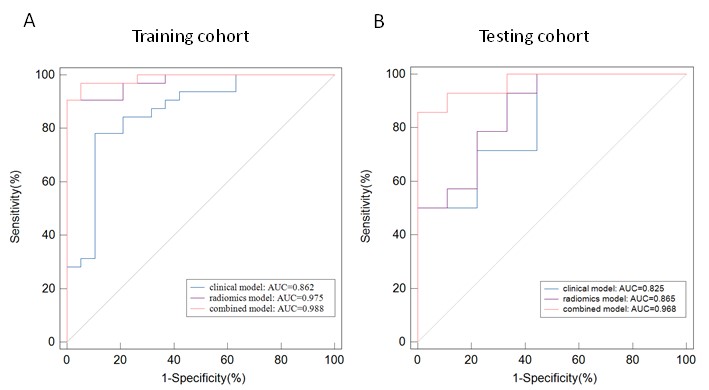
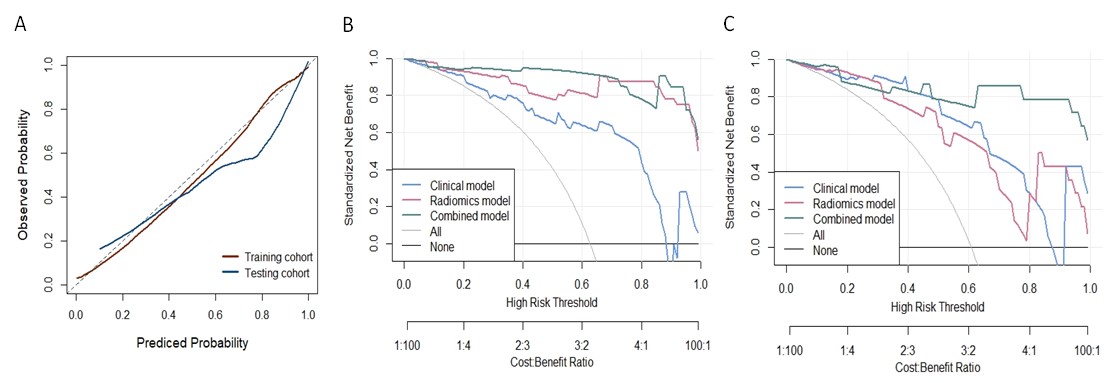
Multifactorial analysis showed that age, educational level, CBF in the left LOFL, left IPL, left SMA, and left ACG had statistical significance (P < 0.05). We conducted logistic regression (LR) with the final clinical features to construct the clinical model. After feature selection, 13 radiomics features from the above four brain regions were considered valuable. In the radiomics model, the LR model showed higher prediction efficiency and robustness, with an AUC of 0.975 in the training cohort and 0.865 in the testing cohort. The diagnostic performance of the combined model was improved in predicting cognitive dysfunction in adult MMD after incorporating the clinical and radiomics features, with an AUC of 0.988 in the training cohort; and 0.968 in the testing cohort. Calibration curve and DCA demonstrated good predictive performance and clinical efficacy of the combined model.Discussion
The cognitive dysfunction in MMD is typically associated with the cerebral regions supplied by the internal carotid and middle cerebral arteries, including the frontal, parietal, and temporal lobes8. Therefore, the bilateral LOFL, ACG, SMA, STG, insula, PCu, and IPL were selected as the ROI for this study. Several studies have shown that cognitive dysfunction in adult MMD patients primarily manifests as executive function deficits, possibly due to decreased perfusion in the frontal lobe 9-11. This study found that MMD patients with cognitive impairment showed significantly decreased perfusion in the left LOFL, left ACG, left SMA, and left IPL compared to patients with normal cognitive function, which is consistent with previous research findings2. Furthermore, our study combined the decreased CBF values with radiomics features in these brain regions, and the final combined model had a good predictive ability for cognitive dysfunction in MMD patients.Conclusion
3D-pCASL can detect areas of decreased CBF in adult MMD patients, with hypoperfusion reflecting cognitive function to some degree. The combined model incorporating CBF and radiomics features of specific brain regions can predict preoperative cognitive dysfunction in adult MMD patients, thus providing a time-saving diagnostic tool to avoid disease progression.Acknowledgements
No acknowledgement found.References
1. Scott RM, Smith ER. Moyamoya disease and moyamoya syndrome. N Engl J Med 2009;360:1226-1237.
2. Kazumata K, Tha KK, Narita H, et al. Chronic ischemia alters brain microstructural integrity and cognitive performance in adult moyamoya disease. Stroke 2015;46:354-360.
3. Karzmark P, Zeifert PD, Tan S, et al. Effect of moyamoya disease on neuropsychological functioning in adults. Neurosurgery 2008;62:1048-1051.
4. Festa JR, Schwarz LR, Pliskin N, et al. Neurocognitive dysfunction in adult moyamoya disease. J Neurol 2010;257:806-815.
5. Haller S, Zaharchuk G, Thomas DL, et al. Arterial Spin Labeling Perfusion of the Brain: Emerging Clinical Applications. Radiology 2016;281:337-356.
6. Won J, Choi DS, Hong SJ, et al. Crossed cerebellar hyperperfusion in patients with seizure-related cerebral cortical lesions: an evaluation with arterial spin labelling perfusion MR imaging. Radiol Med 2018;123:843-850.
7. Lv Y, Wei W, Song Y, et al. Non-invasive evaluation of cerebral perfusion in patients with transient ischemic attack: an fMRI study. J Neurol 2019;266:157-164.
8. Kim JM, Lee SH, Roh JK. Changing ischaemic lesion patterns in adult moyamoya disease. J Neurol Neurosurg Psychiatry 2009;80:36-40.
9. Su SH, Hai J, Zhang L, et al. Assessment of cognitive function in adult patients with hemorrhagic moyamoya disease who received no surgical revascularization. Eur J Neurol 2013;20:1081-1087.
10. Nakamizo A, Kikkawa Y, Hiwatashi A, et al. Executive function and diffusion in frontal white matter of adults with moyamoya disease. J Stroke Cerebrovasc Dis 2014;23:457-461.
11. Fang L, Huang J, Zhang Q, et al. Different aspects of dysexecutive syndrome in patients with moyamoya disease and its clinical subtypes. Journal of Neurosurgery JNS 2016;125:299-307.
Figures