4848
Semi-supervised learning for non-invasive radiopathomic mapping of treatment naïve glioma with multi-parametric MRI1Radiology and Biomedical Imaging, UCSF, San Francisco, CA, United States, 2Center for Intelligent Imaging, UCSF, San Francisco, CA, United States, 3Bioengineering, UCSF/UC Berkeley, San Francisco, CA, United States, 4Neurological Surgery, UCSF, San Francisco, CA, United States, 5Pathology, UCSF, San Francisco, CA, United States
Synopsis
Keywords: Diagnosis/Prediction, Machine Learning/Artificial Intelligence
Motivation: Radiopathomic mapping of glioma could improve standard of care by helping guide surgical resection and subsequent treatment. Most current methods for predicting tumor pathology using MRI neglect intra-tumoral heterogeneity.
Goal(s): We aim to use multi-parametric MRI and deep learning to spatially map pathology for treatment naïve glioma.
Approach: We utilized histopathologically analyzed tissue samples taken during surgical resection with known coordinates on pre-surgical multi-parametric MRI and semi-supervised ensemble networks.
Results: Our model classifies Ki-67 with an AUROC of 0.84 and 0.73 for combined Ki-67 and percent cancerous cells. Including physiologic MRI and pretraining on patches of unknown pathology improved performance.
Impact: We performed radiopathomic mapping in patients with newly-diagnosed glioma using presurgical physiological + anatomical MRI and semi-supervised ensemble networks and achieved AUROCs of 0.84 and 0.73 for Ki-67 and combined Ki-67 and % cancerous cells, respectively.
Introduction
Non-invasive, radiopathomic mapping of glioma in patients with newly-diagnosed glioma can provide critical information for guiding surgical resection and planning subsequent treatment. Although image-guided tissue samples with known spatial coordinates on pre-operative MR imaging and machine learning have been previously utilized to predict tumor pathology1-3, these studies have either used one pathology value to describe the entire lesion2 or analyzed tissue samples for <30 patients3. This study investigates considerations when applying an ensembled deep learning approach for predicting tumor pathology at the location of tissue samples with spatially-mapped coordinates on anatomical and physiological MRI, resulting in higher spatial resolution predictions. The effects of incorporating a self-supervised pretraining strategy using additional unlabeled data from the lesion not involved in the pathology classification task, using overcomplete and traditional CNN architectures, and including physiologic MRI as inputs on performance are evaluated.Methods
Imaging Data: Presurgical multi-parametric MR images (mpMRI) from anatomical, diffusion-weighted, and perfusion-weighted images were obtained from 135 patients with glioma (48% GBM) at the time of diagnosis, and from 105 patients (3 nonunique) at the time of suspected recurrence. These images were acquired with a 3T scanner (GE Healthcare) with 8-channel head coil. Post-contrast 3D T1-weighted, T2 FLAIR, diffusion-weighted (6 or 24 directions, b=1000 or 2000s/mm2, 1.2mm3 isotropic resolution), and Dynamic Susceptibility Contrast perfusion-weighted (DSC;TR/TE/flip-angle=1250-1500/35-54 ms/30°-35°) were obtained. Each imaging modality (T1c, T2-FLAIR, ADC, FA, DSC Peak-height, and %Recovery) were aligned and interpolated to 1mm isotropic resolution then independently standardized to the mode of normal-appearing brain. 10mm volumetric patches surrounding the center of the tissue sample coordinates from each modality were stacked into 4D arrays and used as input to the classification models.Pathology: 284 tissue samples with recorded spatial coordinates on imaging were collected from newly-diagnosed with glioma and evaluated histopathologically for tumor content (tumor score; 1-3) and % MIB-1/Ki-67. A combined invasiveness score was obtained by adding the tumor score to the natural logarithm of the Ki-67. The samples were then labeled as having highly invasive pathology if their combined score was above ln(10)+1.5 (10% is commonly used as a threshold for Ki-672 and 1.5 is the median tumor score separating samples with greater than 10% cancerous cells), resulting in 155/129 high/low invasiveness samples and 109/175 high/low Ki-67 samples.
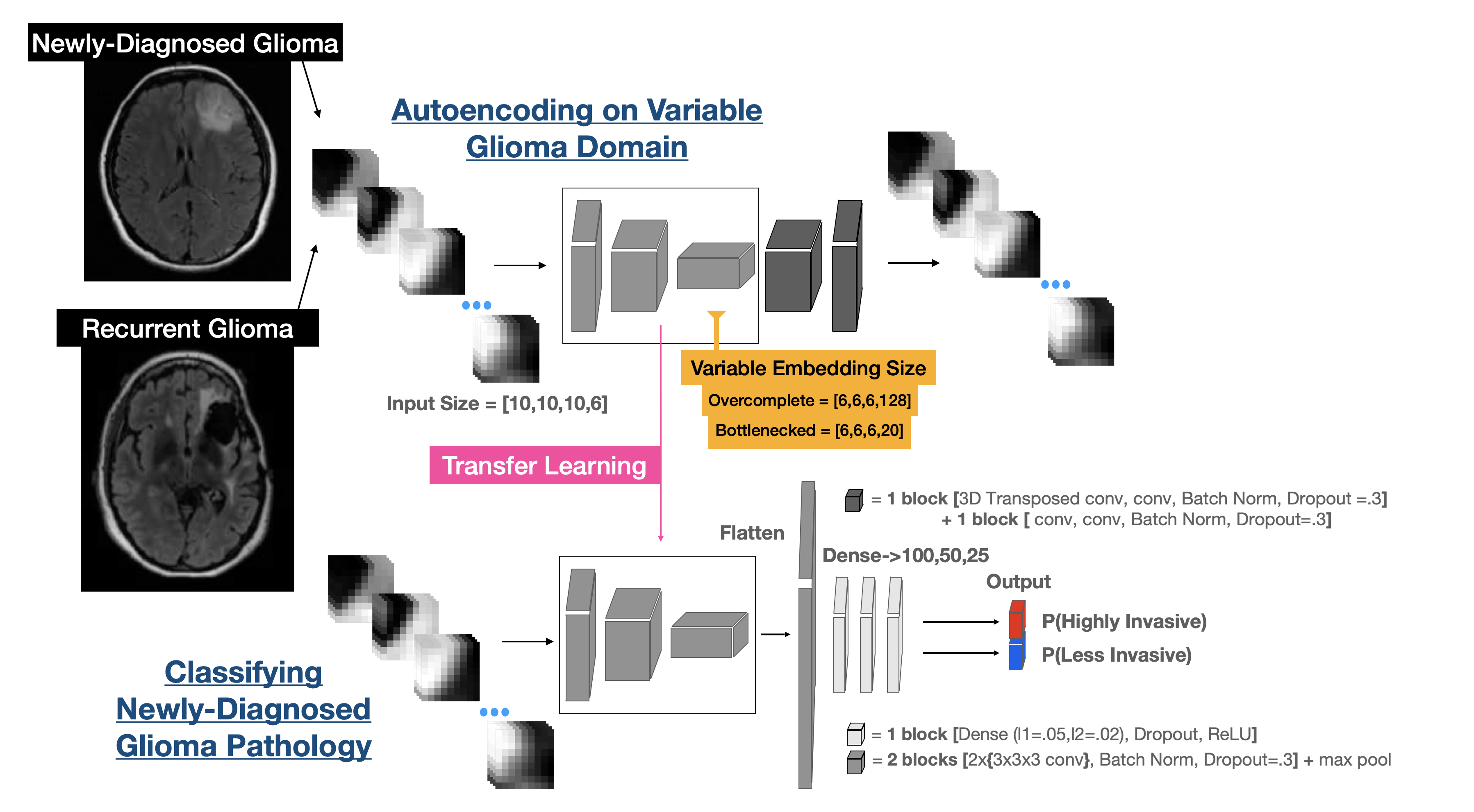
Training: Bottlenecked and overcomplete autoencoders were trained on patches within the T2-lesion without pathology labels to reconstruct multi-parametric stacks of imaging volumes for different glioma datasets. The resulting 16.6k and 27.4k multi-parametric patches from newly-diagnosed and recurrent gliomas, respectively, were used separately and combined in training autoencoders that were used to initialize the encoders of the radiopathomic classification models (Figure 1). A 75/25 initial split was used for both classification tasks. The autoencoders were trained with a further 80/20 split, and the classifiers were trained as an ensemble using 4 repeats of 5-fold cross validation on the original training data with loose constraints on the class stratification but tight constraints on the patient groupings to avoid data leakage4. Smaller class proportions were oversampled via augmentation.
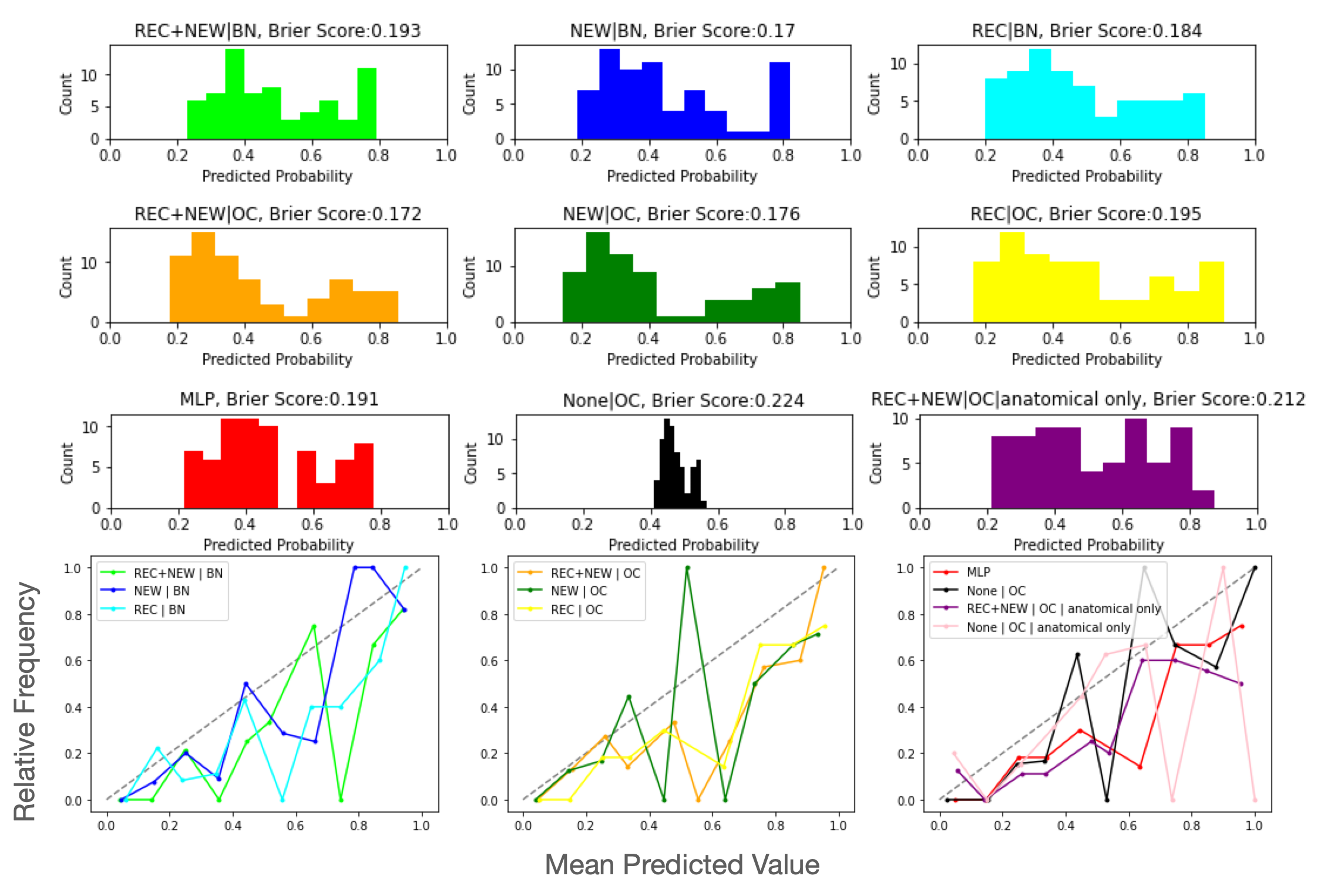
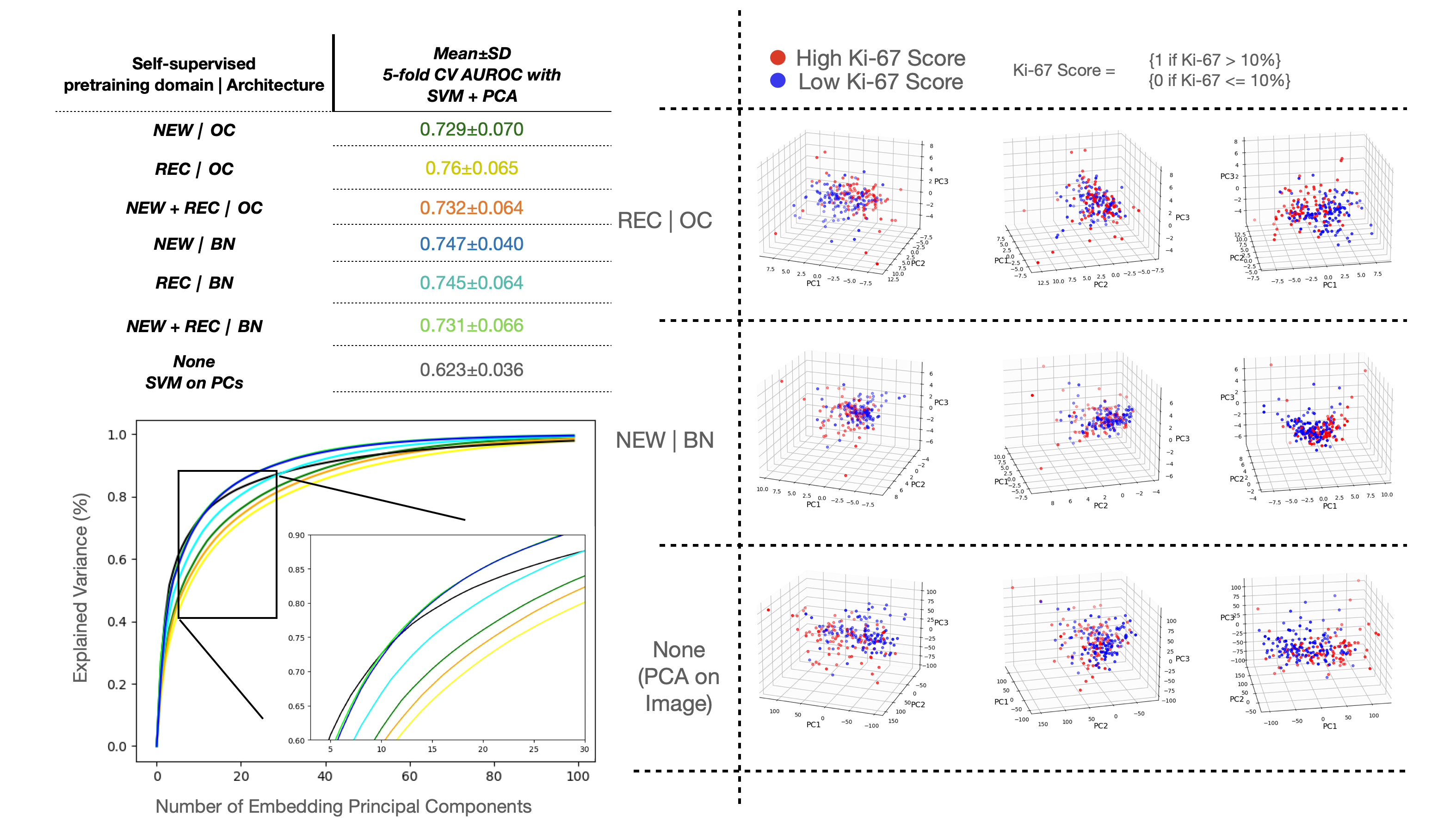
Model Evaluation: Autoencoding strategies were quantitatively compared by downstream classification performance with AUROC. The embeddings of the autoencoders were compared by visualizing class separation after performing PCA and 5-fold CV with an SVM. Classification models were compared using AUROC, Brier scores, histograms of the distribution of the ensemble predictions, and reliability curves.
Results and Discussion
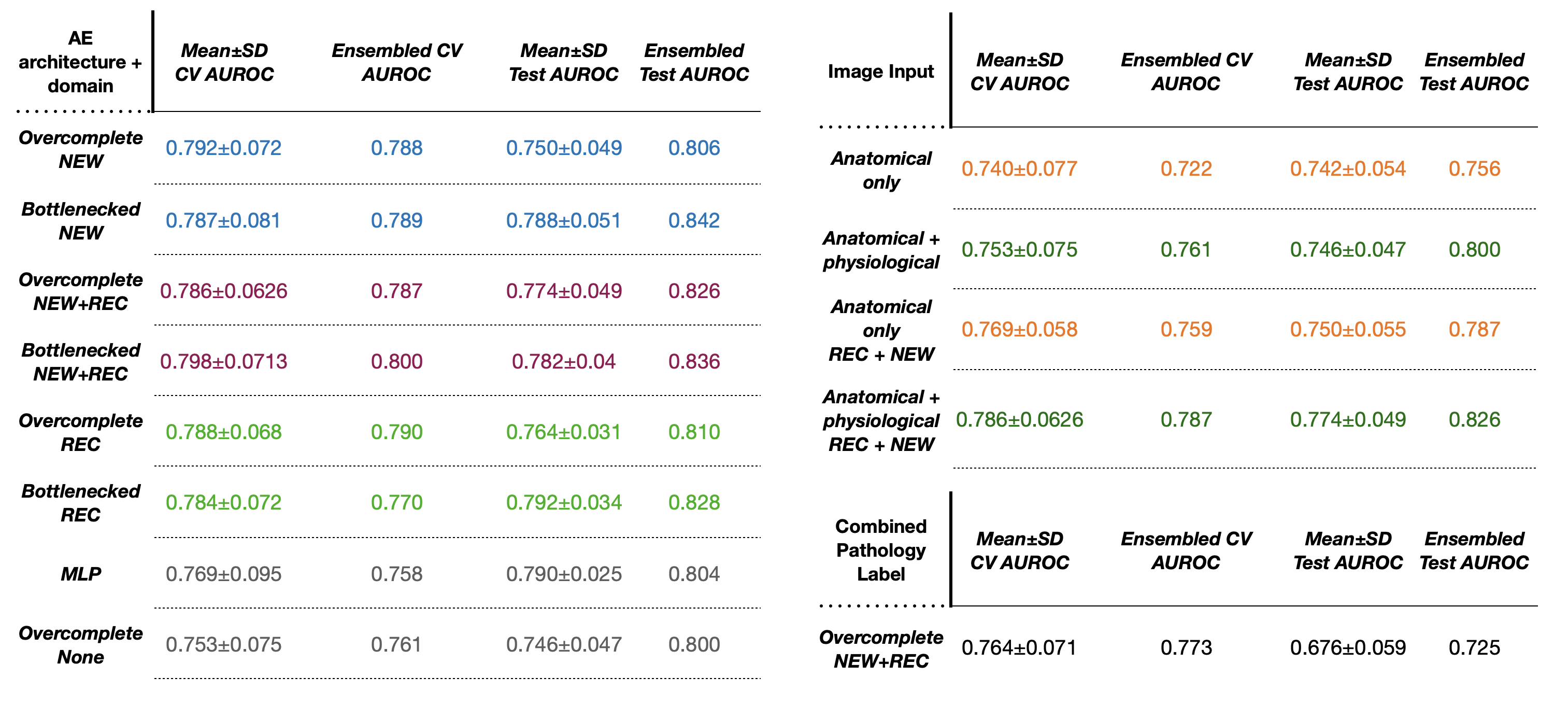
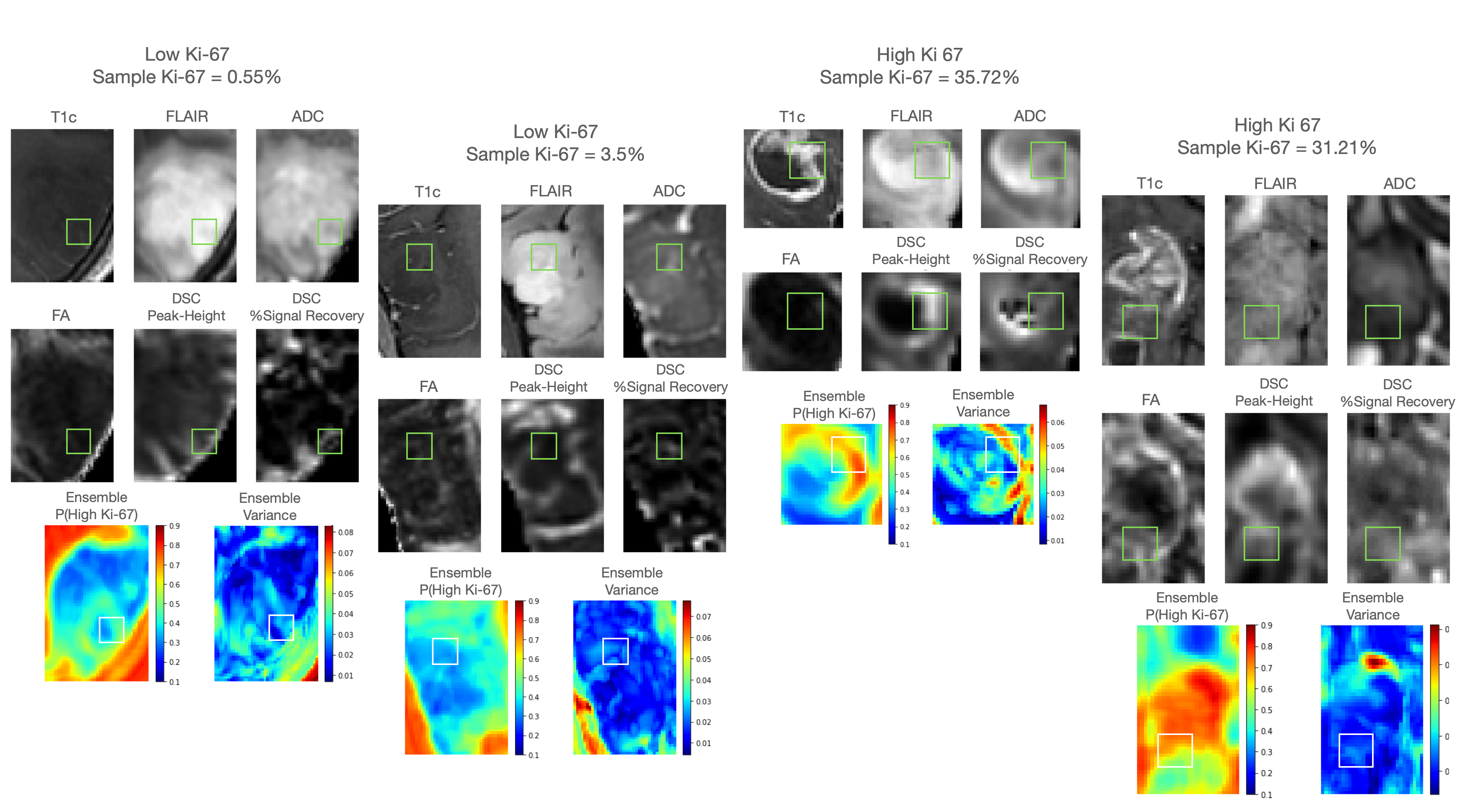
Our best model employed a bottlenecked architecture for pretraining on images from newly-diagnosed gliomas and achieved a test AUROC of 0.84 for classifying Ki-67 (Figure 2). Addition of physiological imaging improved performance across all comparisons. Although bottlenecked models had slightly better performance, the overcomplete models learned nontrivial feature embeddings useful for separation of pathology. The overcomplete model pretrained on a combination of recurrent and newly-diagnosed glioma achieved the highest AUROC of 0.73 for classifying the combined invasiveness score. Self-supervised pretrained models were better calibrated then the fully supervised models as evident by lower Brier scores and higher reliability (Figure 3). Evaluation of the self-supervised autoencoder embeddings showed better SVM performance with PCA in 5-fold CV and showed greater class separability than PCA on the images alone (Figure 4). Spatial maps of the best ensemble demonstrated regions of high/low predicted Ki-67 that corresponded to actual high/low Ki-67 values from tissue samples taken from the same location (Figure 5).Conclusion
Our results support the feasibility of non-invasive radiopathomic mapping of treatment naïve glioma at the time of diagnosis with MRI and deep learning. Semi-supervised models with transfer learning performed better than fully-supervised models and including physiologic imaging contrasts improved performance.Acknowledgements
NIH-NCI: P01CA118816References
[1] van Kempen EJ et. al. “Accuracy of Machine Learning Algorithms for the Classification of Molecular Features of Gliomas: A Systematic Literature Review and Meta-Analysis.” Cancers (Basel); May 2021.
[2] X. Li, Y. Xu, F. Xiang, Q. Liu, W. Huang, and B. Xie, “KINET: A NON-INVASIVE METHOD FOR PREDICTING KI67 INDEX OF GLIOMA,” in Proceedings - International Conference on Image Processing, ICIP, IEEE Computer Society, 2021, pp. 150–154. doi: 10.1109/ICIP42928.2021.9506741.
[3] E. D. H. Gates et al., “Guiding the first biopsy in glioma patients using estimated Ki-67 maps derived from MRI: Conventional versus advanced imaging,” Neuro Oncol, vol. 21, no. 4, pp. 527–536, Mar. 2019, doi: 10.1093/neuonc/noz004.
[4] Ellison J et al. Self-supervised pretraining and network ensembling for spatial mapping of treatment-effect in recurrent GBM with physiologic MRI. International Society for Magnetic Resonance in Medicine; 2023.
Figures