4844
Predictive Value of Biochemical Recurrence in Advanced Prostate Cancer: Development of Deep Learning-based Radiomics Model1Peking University First Hospital, Beijing, China, 2School of Basic Medical Sciences, Capital Medical University, Beijing, China, 3Beijing Smart Tree Medical Technology Co. Ltd, Beijing, China
Synopsis
Keywords: Diagnosis/Prediction, Radiomics
Motivation: Deep learning forpredicting biochemical recurrence (BCR) is feasible but needs further evaluation in advanced prostate cancer (PCa).
Goal(s): We aimed to develop radiomics models with automatic segmentation derived from pretreatment ADC maps that may be predictive of BCR in advanced PCa.
Approach: In this study, PCa areas were segmented on ADC images by using a pre-trained artificial intelligence (AI) model. Three models were constructed to evaluate BCR prediction level.
Results: The deep-radiomics model was superior than the clinical model and the conventional radiomics model in the aspect of prediction accuracy, clinical impact and risk assessment.
Impact: With accurate BCR prediction by deep-radiomics model, more appropriate treatment plans may be formulated and intervention treatment can be carried out as soon as possible, resulting in better prognosis for patients with PCa.
INTRODUCTION
Prostate cancer (PCa) is the second most common cancer in men and a leading cause of cancer-related deaths1. After treatment, some patients might experience biochemical recurrence (BCR)2. BCR serves as a prognostic indicator for the cure of PCa, clinical metastases and ultimately PCa-related death2. Prediction of BCR could help healthcare professionals in treatment planning by identifying patients who may benefit from additional therapies or interventions. Our study aimed to develop radiomics models for predicting the biochemical recurrence (BCR) of advanced prostate cancer (PCa) based on pretreatment apparent diffusion coefficient (ADC) maps.METHODS
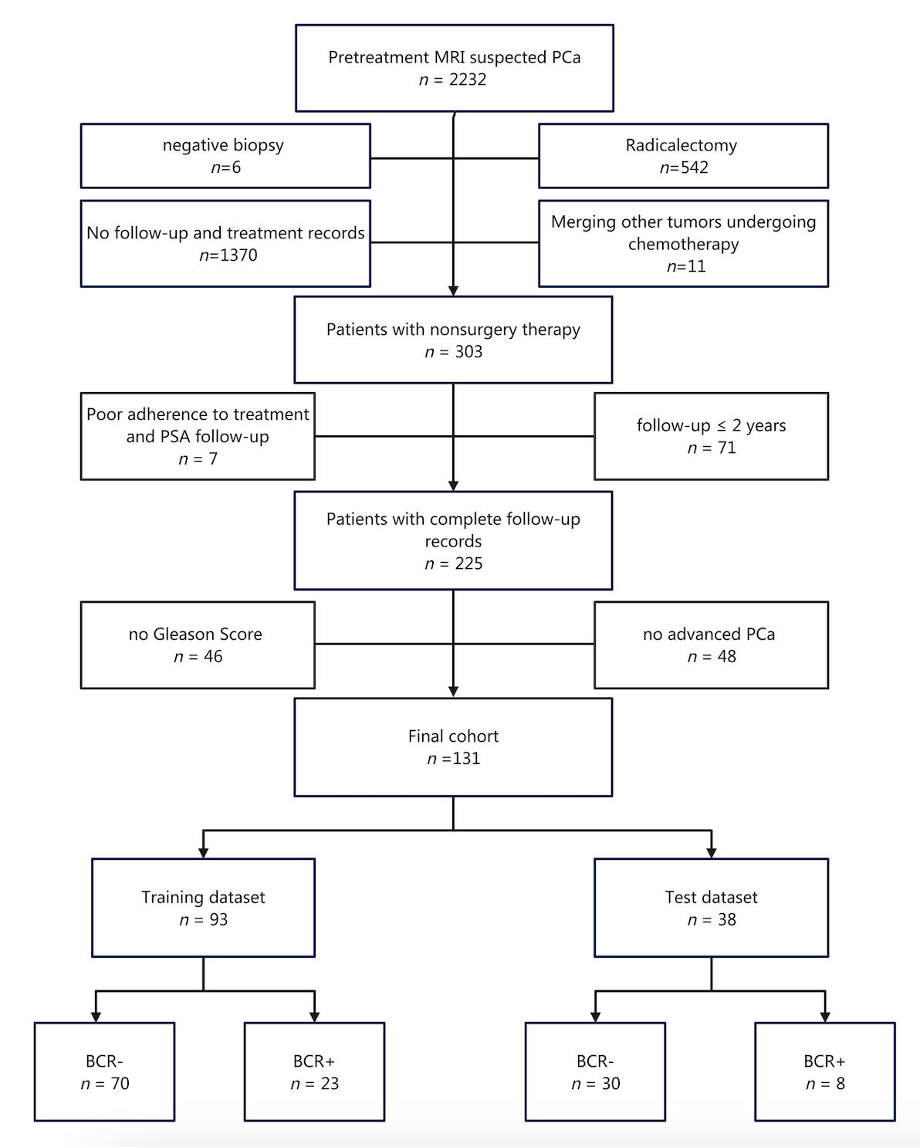
This retrospective study included a total of 131 cases of pathologically confirmed PCa (Figure 1), comprising 100 patients without biochemical recurrence (BCR-) and 31 patients with biochemical recurrence (BCR+). Pre-treatment ADC images were segmented using a pre-trained artificial intelligence (AI) model to identify suspicious PCa areas, which were taken as the regions of interest (ROI) for this study. The 131 cases were randomly divided into training (n = 93) and test (n = 38) datasets. Three predictive models were developed: 1) a clinical model incorporating clinical information, location, volume, and ADC value of the PCa area as the predictor variables, 2) a conventional radiomics model integrating clinical information and radiomics-based PCa image features, and 3) a deep-radiomics model combining clinical information and PCa image features extracted through deep learning neural network algorithms. Performance metrics, such as the area under the receiver operating characteristic (ROC) curve (AUC), precision-recall (PR) curve and decision curve analysis (DCA), were used to assess predictive performance of these models in test dataset. Additionally, the net reclassification index (NRI) and integrated discrimination improvement (IDI) were employed to compare the performance enhancement of the radiomics model and the deep-radiomics model in relation to the clinical model.RESULTS
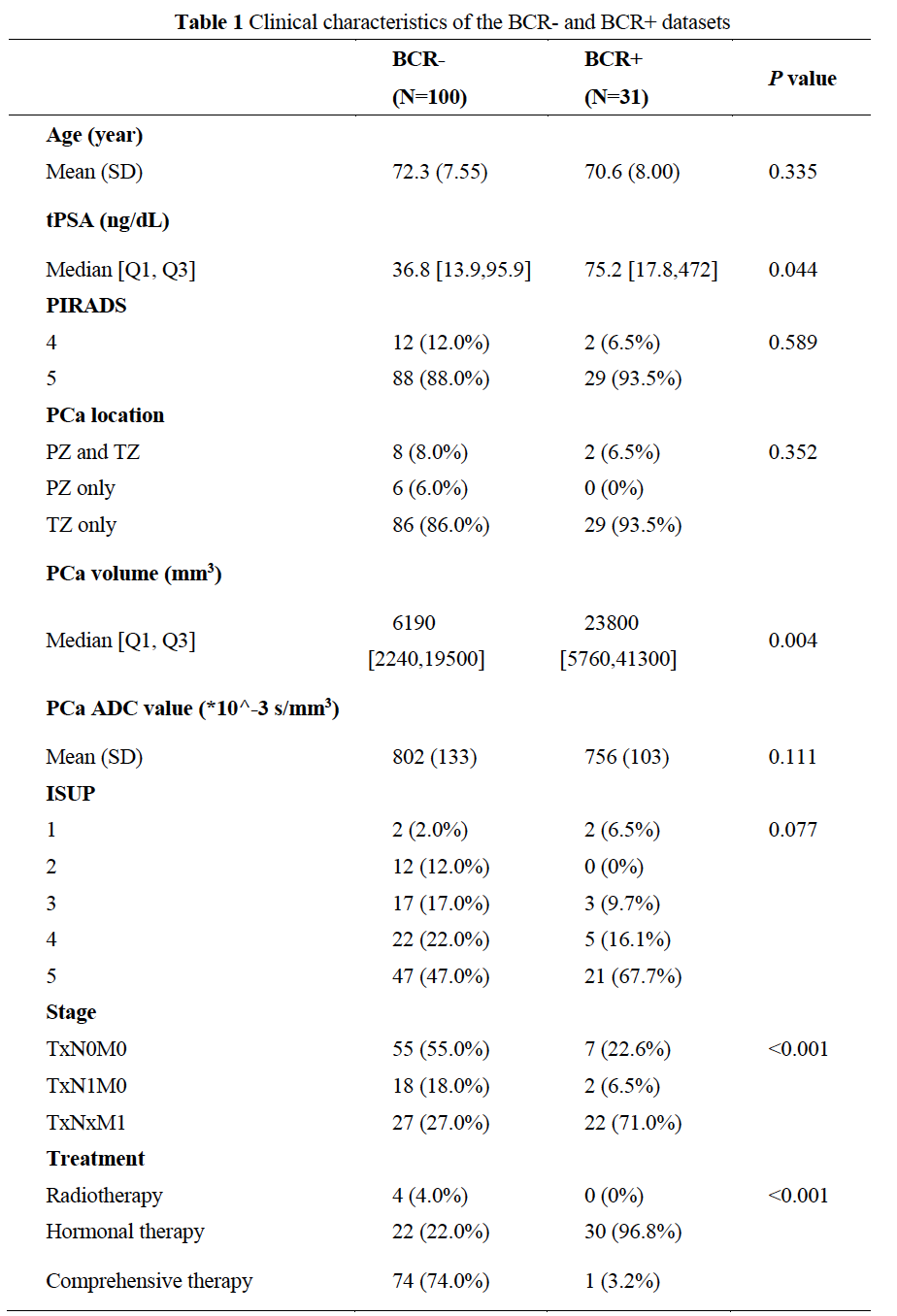
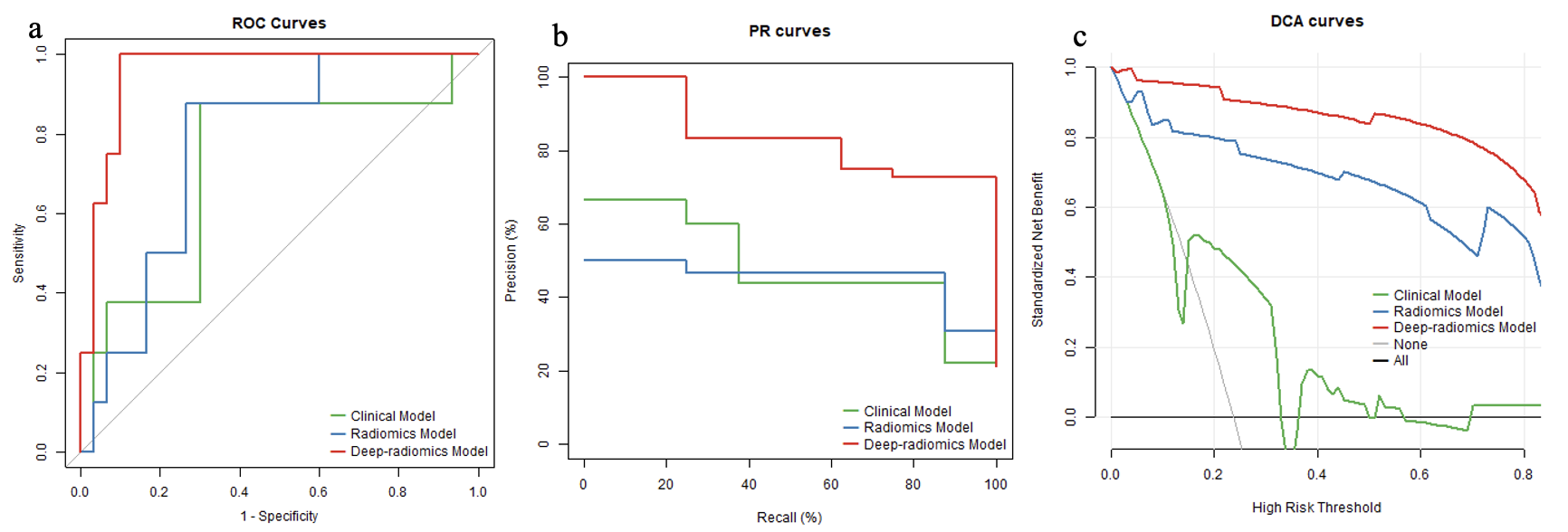
There were no significant differences in age, PI-RADS score, PCa location, PCa ADC value and ISUP group between the BCR- and BCR+ groups (all P > 0.05, Table 1). However, significant differences were observed in PSA level, PCa volume, clinical stage, and treatment method between the BCR- and BCR+ groups (all P < 0.05). The AUC of the ROC curve was 0.717 (95% CI: 0.492, 0.941) for the clinical model, 0.771 (95% CI: 0.607, 0.935) for the radiomics model, and 0.954 (95% CI: 0.892, 1.000) for the deep-radiomics model in the test dataset (Figure 2a). The deep-radiomics model exhibited a significantly higher AUC than the clinical model (P = 0.033) and the radiomics model (P = 0.026). The AUC of the PR curve was 0.385 (95% CI: 0.191, 0.696) for the clinical model, 0.373 (95% CI: 0.209, 0.665) for the radiomics model, and 0.805 (95% CI: 0.451, 0.985) for the deep-radiomics model (Figure 2b). The PR AUC of the deep-radiomics model differed significantly from both the clinical model (0.420, 95% BCa: 0.292-0.651) and the radiomics model (0.432, 95% BCa: 0.327-0.638). The DCA curve demonstrated superior performance for the deep-radiomics model compared to others across all risk thresholds. Additionally, the DCA curve of the radiomics model outperformed the clinical model across all risk thresholds (Figure 2c). Compared to the clinical model, the NRI was 0.359 (95% CI: 0.099, 0.973) for the radiomics model and 0.508 (95% CI: 0.309, 1.175) for the deep-radiomics model. Furthermore, the NRI from the radiomics model to the deep-radiomics model was 0.149 (95% CI: 0.032, 0.300). Taking the clinical model as the reference, the IDI was 0.516 (95% CI: 0.294, 0.666) for the radiomics model and 0.679 (95% CI: 0.431, 0.795) for the deep-radiomics model. The IDI from the radiomics model to the deep-radiomics model was 0.164 (95% CI: -0.045, 0.363).DISCUSSION
Our findings align with previous studies in terms of the predictive efficiency of radiomics models for BCR3-8. However, our study differs from previous research in three main aspects: (1) patients with advanced PCa who received non-surgical treatment as research objective, (2) the utilization of a pre-trained AI model for automatic segmentation of the ROI, and (3) a comparison between conventional radiomics models and deep radiomics models in terms of feature extraction. We employed multiple methods to evaluate the performance of predictive models from different perspectives9.CONCLUSION
The deep-radiomics model exhibits promising potential in predicting BCR in advanced PCa, compared to both the clinical model and the conventional radiomics model.Acknowledgements
This study was funded by National High Level Hospital Clinical Research Funding (Scientific Research Seed Fund of Peking University First Hospital) (2022SF52).References
1. Rawla P. Epidemiology of Prostate Cancer. World J Oncol. 2019;10(2):63-89.
2. Van den Broeck T, van den Bergh RCN, Briers E et al. Biochemical Recurrence in Prostate Cancer: The European Association of Urology Prostate Cancer Guidelines Panel Recommendations. Eur Urol Focus. 2020;6(2):231-234.
3. An P, Lin Y, Hu Y et al. Predicting Model of Biochemical Recurrence of Prostate Carcinoma (PCa-BCR) Using MR Perfusion-Weighted Imaging-Based Radiomics. Technol Cancer Res Treat. 2023; 22:15330338231166766.
4. Bourbonne V, Fournier G, Vallières M et al. External Validation of an MRI-Derived Radiomics Model to Predict Biochemical Recurrence after Surgery for High-Risk Prostate Cancer. Cancers (Basel). 2020;12(4):814.
5. Dinis Fernandes C, Dinh CV, Walraven I et al. Biochemical recurrence prediction after radiotherapy for prostate cancer with T2w magnetic resonance imaging radiomic features. Phys Imaging Radiat Oncol. 2018;7:9-15.
6. Shiradkar R, Ghose S, Jambor I et al. Radiomic features from pretreatment biparametric MRI predict prostate cancer biochemical recurrence: Preliminary findings. J Magn Reson Imaging. 2018;48(6):1626-1636.
7. Shiradkar R, Ghose S, Mahran A et al. Prostate Surface Distension and Tumor Texture Descriptors From Pre-Treatment MRI Are Associated With Biochemical Recurrence Following Radical Prostatectomy: Preliminary Findings. Front Oncol. 2022;12:841801.
8. Zhong QZ, Long LH, Liu A et al. Radiomics of Multiparametric MRI to Predict Biochemical Recurrence of Localized Prostate Cancer After Radiation Therapy. Front Oncol. 2020;10:731.
9. Demircioğlu A. Are deep models in radiomics performing better than generic models? A systematic review. Eur Radiol Exp. 2023;7(1):11.
Figures