4834
Creating Digital Twins of Solid Tumors: Insights from Dynamic Contrast-Enhanced MRI1Department of Human Structure and Repair, Ghent University, Ghent, Belgium, 2IBiTech – BioMMeda, Ghent University, Ghent, Belgium, 3Department of Radiology, Ghent University Hospital, Ghent, Belgium
Synopsis
Keywords: In Silico, Quantitative Imaging, Digital twin
Motivation: Prediction of cancer therapy outcomes is a paramount objective in oncology, closely tied to the integration of novel biomarkers into clinical practice.
Goal(s): The goal of creating digital twins of solid tumors is to equip oncologists with a comprehensive replica of the tumor, allowing them to make well-informed decisions.
Approach: In the development of digital twins for solid tumors, we introduce a multidisciplinary approach that essentially combines quantitative MRI and computational modeling.
Results: The image-based model yields a comprehensive representation of tumor perfusion, providing a map of elevated interstitial fluid pressure, which holds significant potential as a biomarker in oncology.
Impact: Cancer therapy's success is not guaranteed, with potential serious side effects. Our aim is to offer a robust digital tumor replica for evaluating numerous treatment options, identifying the optimal plan while minimizing adverse effects.
Introduction
Drug transport to solid tumors has been shown to be limited [1]. The transport of therapeutic agents to the tumor stroma relies on two mechanisms: convection (dependent on pressure gradients) and diffusion (dependent on concentration gradients) [1, 2]. While convective transport is often hindered by elevated interstitial fluid pressure (IFP) within the tumor, diffusive transport remains the predominant positive transport pathway, but it is both limited and slow, resulting in inadequate drug delivery [2]. The biophysics of drug transport has been extensively reviewed, with the permeability and density of tumor vasculature identified as critical factors controlling IFP [2]. However, patient-specific studies of tumor vasculature properties have been largely lacking due to challenges in addressing both inter- and intra-tumoral heterogeneity. In this context, we utilize dynamic contrast-enhanced MRI (DCE-MRI) as a powerful tool to evaluate tumor vasculature, aiming to construct digital twins of solid tumors.Methods
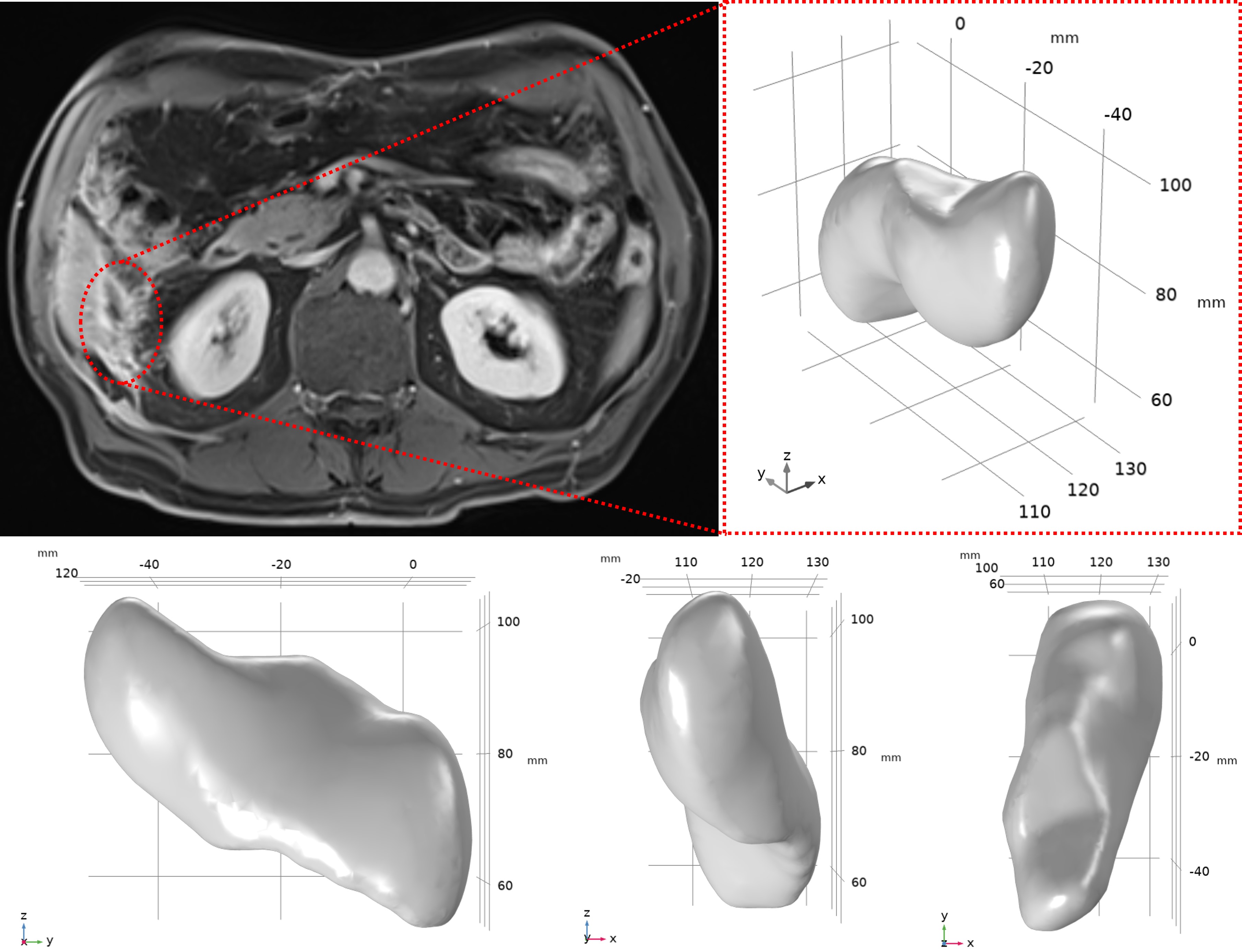
Data acquisitionIn the context of a translational clinical study (EC/2019/1330, approved by the local ethical committee), we conducted imaging on a patient with peritoneal metastasis using a 3T clinical MR system (PrismaFit, Siemens Healthineers, Germany). The MR imaging protocol encompassed various sequences, including coronal respiratory triggering fat-suppressed HASTE T2-weighted imaging, 3D-T2 weighted coronal SPACE imaging with and without fat-suppression, and transversal 3D gradient echo (3D-GRE) volumetric interpolated breath-hold examination (VIBE) T1-weighted imaging. Additionally, axial breath-hold 3D GRE VIBE T1-weighted imaging was performed without the administration of a contrast agent to establish the anatomical location of the tumor. Finally, a transversal free-breathing prototype 3D GRASP-VIBE dynamic contrast-enhanced scan sequence was continuously acquired [3], achieving an offline-reconstructed temporal resolution of 1.4 seconds. This was done after the intravenous administration of 0.1 mmol/kg of Prohance contrast agent, followed by a 20 ml saline flush at a rate of 2.0 ml/s.
Data analysis
We utilized the open-source software, Quantiphyse [4], for image analysis. Groupwise registration was employed for image motion correction and co-registration [5]. Subsequently, the DCE-MRI data was quantified using the extended-Tofts model [6] to generate the volume transfer constant (Ktrans) map. Furthermore, the arterial input function (AIF) was determined from the abdominal aorta, accounting for any bolus arrival delay. The tumor contours were delineated by an experienced radiologist, and based on these contours, the 3D geometry of the tumor was reconstructed.
Computational fluid dynamics (CFD) modeling of IFP
Using the reconstructed 3D geometry, interstitial fluid flow within the tumor was simulated using CFD modeling in COMSOL Multiphysics (Inc., Burlington, USA). The tumor was situated within a normal peripheral region, where the interstitial flow is governed by Darcy’s law (Eq. 1) and the continuity equation. Starling’s law (Eq. 2) is employed to express the interstitial fluid source. Within this framework, the Ktrans map was incorporated to address microvascular permeability (LP) and density (S/V) heterogeneities. It was assumed that no lymphatic vessels were present within the tumor, and the interstitial fluid pressure (IFP) at the boundary of normal tissue, far from the tumor, was set to 0 mmHg (representing normal IFP).
$$u_i=-K\triangledown p_i\hspace{1cm}(Eq.1)\\ \nabla.u_i=L_p\frac{S}{V}(p_v-p_i-\sigma(\pi_v- \pi_i)), L_p=\frac{K^{trans}}{\overline{K^{trans}}}L_{p0}\hspace{1cm}(Eq.2)$$
With pi the IFP, ui the interstitial fluid velocity (IFV), S/V the surface area per unit volume, pv the vascular pressure, σ the osmotic reflection coefficient, πv the vascular osmotic pressure and πi the interstitial osmotic pressure [2]. Lp0 is the baseline value for vascular permeability. To enable the evaluation of image-based data effects, a corresponding basic model was generated using the same geometry, but with a uniform value assigned for LP (i.e. Lp0).
Results
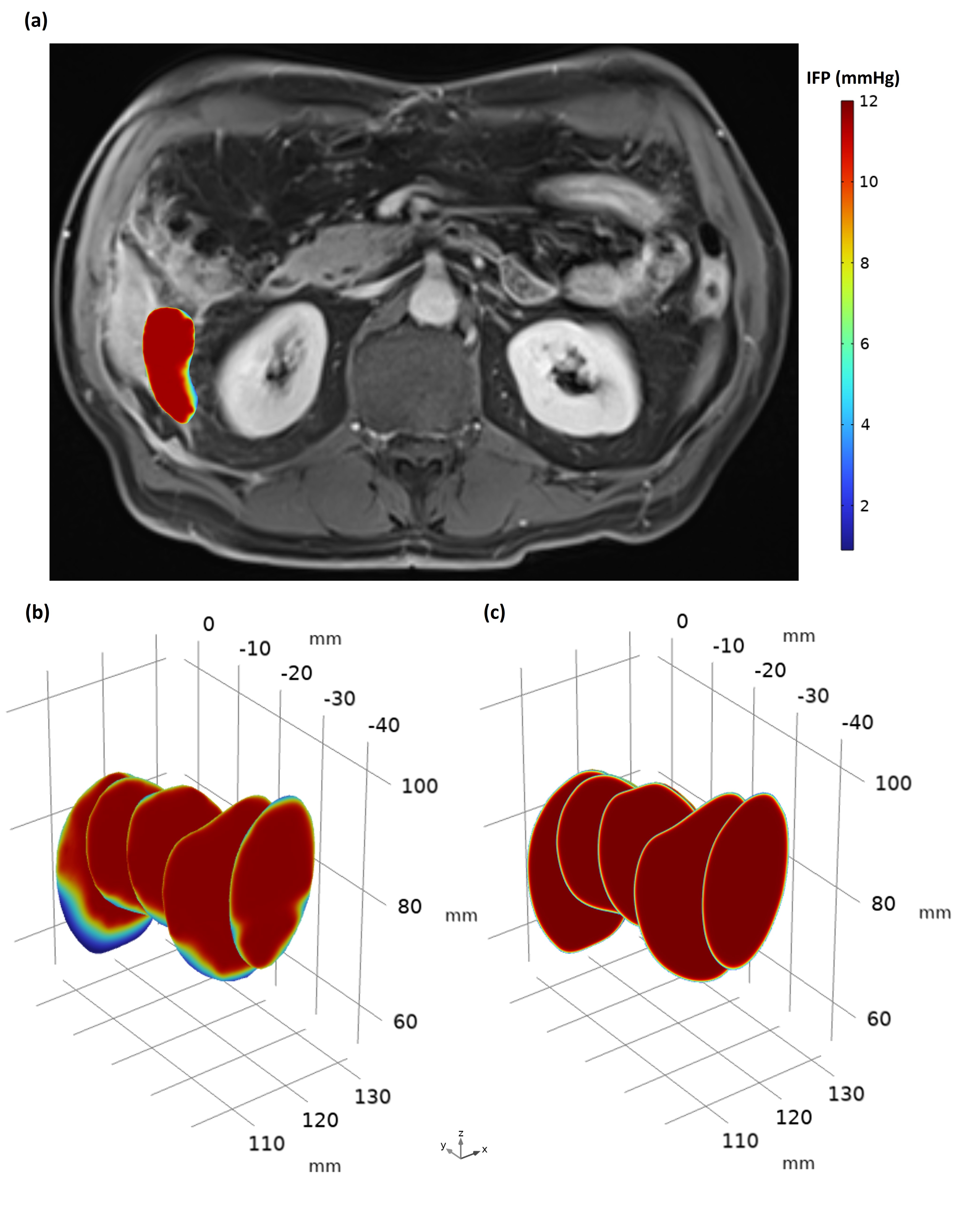
The 3D configuration of the tumor is depicted in Figure 1, with a volume of 27746 mm3. The findings illustrated in Figures 2a and 2b reveal an elevated region of IFP within the tumor. This observation can be correlated with the non-enhancing region depicted in Figure 1. Upon comparing the outcomes of the baseline model (Figure 2c) with the personalized model (Figure 2b), it is apparent that in the basic model, IFP is almost uniformly distributed throughout the tumor, except near the tumor's surface where it rapidly decreases to the normal tissue IFP. In contrast, when incorporating Ktrans data, the IFP exhibits greater heterogeneity, particularly at the outer layers of the tumor (Figure 2b).Discussion and conclusion
An image-based CFD model highlighted the variability in IFP within a solid tumor. The current study, pivotal in creating personalized computational models, gains advantage from enhancements with complex mathematical models and additional patient-specific data. The current study holds the potential to introduce a novel diagnostic tool in clinical oncology.Acknowledgements
No acknowledgement found.References
1. Salavati, H., et al., Interstitial fluid pressure as an emerging biomarker in solid tumors. Biochimica et Biophysica Acta (BBA)-Reviews on Cancer, 2022: p. 188792.
2. Salavati, H., et al., Drug transport modeling in solid tumors: A computational exploration of spatial heterogeneity of biophysical properties. Computers in Biology and Medicine, 2023. 163: p. 107190.
3. Feng, L., et al., Golden‐angle radial sparse parallel MRI: combination of compressed sensing, parallel imaging, and golden‐angle radial sampling for fast and flexible dynamic volumetric MRI. Magnetic resonance in medicine, 2014. 72(3): p. 707-717.
4. Chappell, M.A., et al., Variational Bayesian inference for a nonlinear forward model. IEEE Transactions on Signal Processing, 2008. 57(1): p. 223-236.
5. Huizinga, W., et al., PCA-based groupwise image registration for quantitative MRI. Medical image analysis, 2016. 29: p. 65-78.
6.Tofts, P.S., et al., Estimating kinetic parameters from dynamic contrast‐enhanced T1‐weighted MRI of a diffusable tracer: standardized quantities and symbols. Journal of Magnetic Resonance Imaging: An Official Journal of the International Society for Magnetic Resonance in Medicine, 1999. 10(3): p. 223-232.
Figures