4832
Computational Fluid Dynamics Of Bladder Voiding Using 3D Dynamic MRI1University of Wisconsin-Madison, Madison, WI, United States
Synopsis
Keywords: In Silico, In Silico, MRI-based CFD, Urodynamics
Motivation: Catheter-based urodynamic studies to assess bladder dysfunction are invasive and provide inadequate biomechanical information. MRI-based computational fluid dynamics (CFD) has demonstrated potential to uncover these features not evident from catheterization.
Goal(s): Develop and implement a computational methodology to non-invasively assess urodynamics.
Approach: Acquire 3D dynamic MRI of bladder voiding. Use the images to execute subject-specific CFD simulations of the bladder and urethra. Calculate existing urological nomograms and energy expended to quantify bladder function using the MRI and CFD results.
Results: The healthy subject showed unobstructed bladder outlet and normal contractility. We calculated the energy expended to void bladder for the first time.
Impact: A method using MRI-based computational fluid dynamics was developed to simulate bladder voiding. Results show successful quantification of urine flow dynamics. This method shows potential to overcome limitations of current invasive catheter-based urodynamic studies.
Introduction
Benign prostatic hyperplasia (BPH) and lower urinary tract symptoms (LUTS) are common among aging men1,2. Multichannel urodynamics (UDS) is the most common diagnostic method used to assess BPH/LUTS3,4. UDS require invasive catheterization to assess pressure-flow relations. Moreover, UDS does not provide sufficient information on bladder/urethra biomechanics5,6. MRI provides anatomical features not evident from UDS, but on its own provides no pressure information. The purpose of this study was to develop and implement a non-invasive computational methodology to simulate urinary flow inside bladder and urethra by coupling 3D dynamic MRI and computational fluid dynamics (CFD).Methods
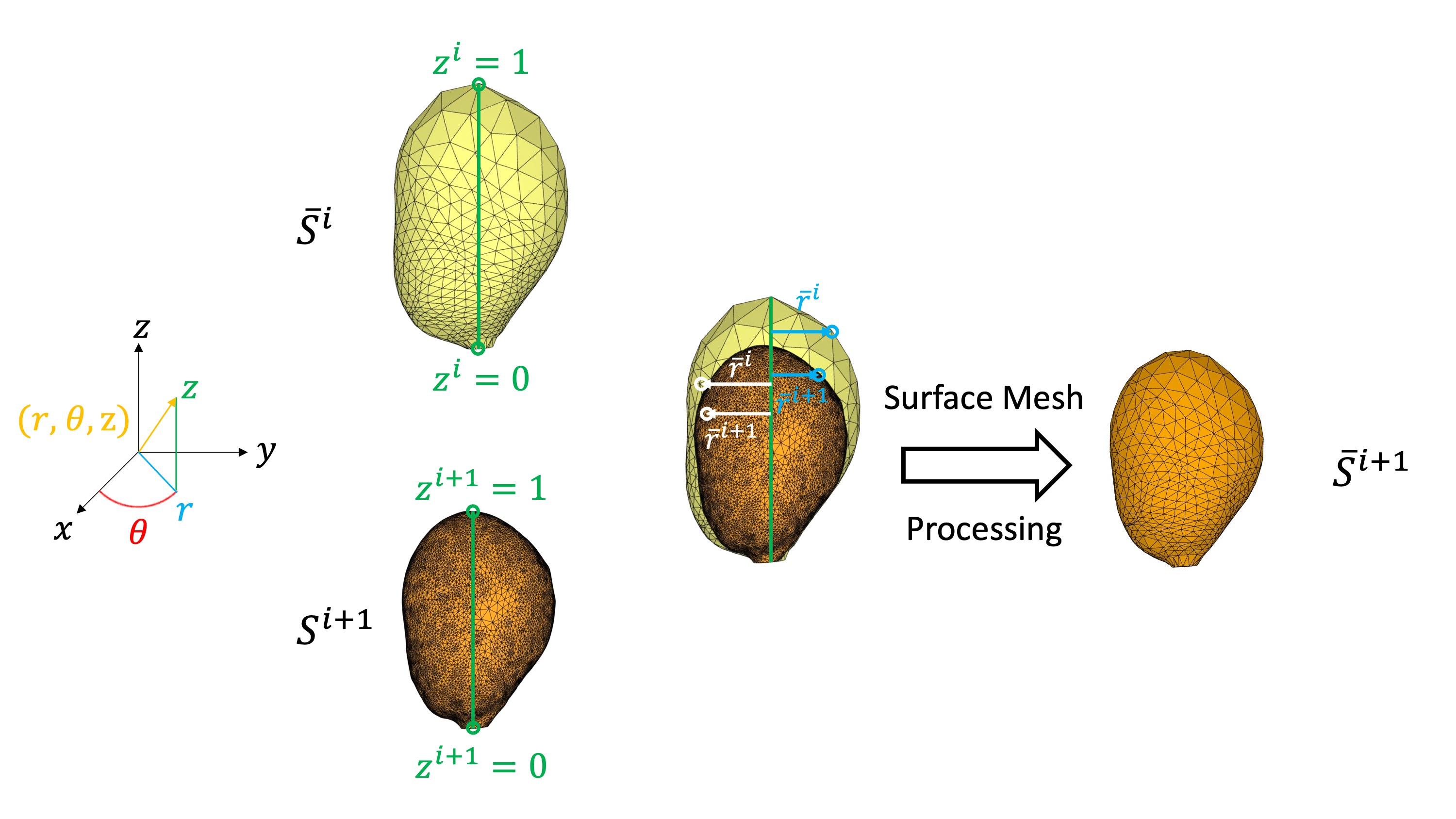
One healthy subject with no history of BPH/LUTS (29 years old) was recruited following an IRB-approved HIPAA-compliant protocol. Subject underwent pelvic MRI on a clinical 3T scanner (Premier, GE Healthcare, Waukesha, WI, USA). 1/3 of a single weight-based dose (0.1 mmol/kg) of gadolinium-based contrast was slowly hand injected intravenously 15 minutes prior to the start of the imaging session. Immediately before the scan, the subject was equipped with a condom catheter to allow micturition while scanning. Volumetric dynamic images of the bladder and urethra were acquired throughout the voiding event in supine position using 3D Differential Subsampling with Cartesian Ordering (DISCO) Flex with spatial resolution = 1 mm x 1 mm x 2 mm, temporal resolution = 3.8 s. The 3D images were manually segmented using Mimics (Materialise NV, Leuven, Belgium), providing an anatomical geometry of the bladder and urethra at each time point. The urine flow rate was calculated as the time rate of change of bladder volume and was used to execute a CFD simulation of the urethra. Each bladder anatomy was represented as a surface mesh composing of discrete triangular surface elements. We developed a MATLAB script that processes the surface meshes such that all bladder anatomies have identical surface topologies (number of triangles, connectivity, etc.) while preserving the shape of the bladder from MRI (Figure 1). Wall-driven CFD simulation of the bladder were executed in CONVERGE CFD solver where the wall motion is the transition of the bladder anatomy between successive time phases. The outlet pressure boundary condition at the bladder neck was the solution from the urethra simulation. The maximum flow rate (Qmax) and bladder pressure from CFD were used to calculate bladder outlet obstruction index (BOOI) and bladder contractility index (BCI), which are nomograms used to diagnose BPH/LUTS. We also calculated the energy expended to void using pressure-volume relation derived from CFD results. Figure 2 illustrates the methodology pipeline from in-vivo MRI to bladder voiding CFD simulation.Results
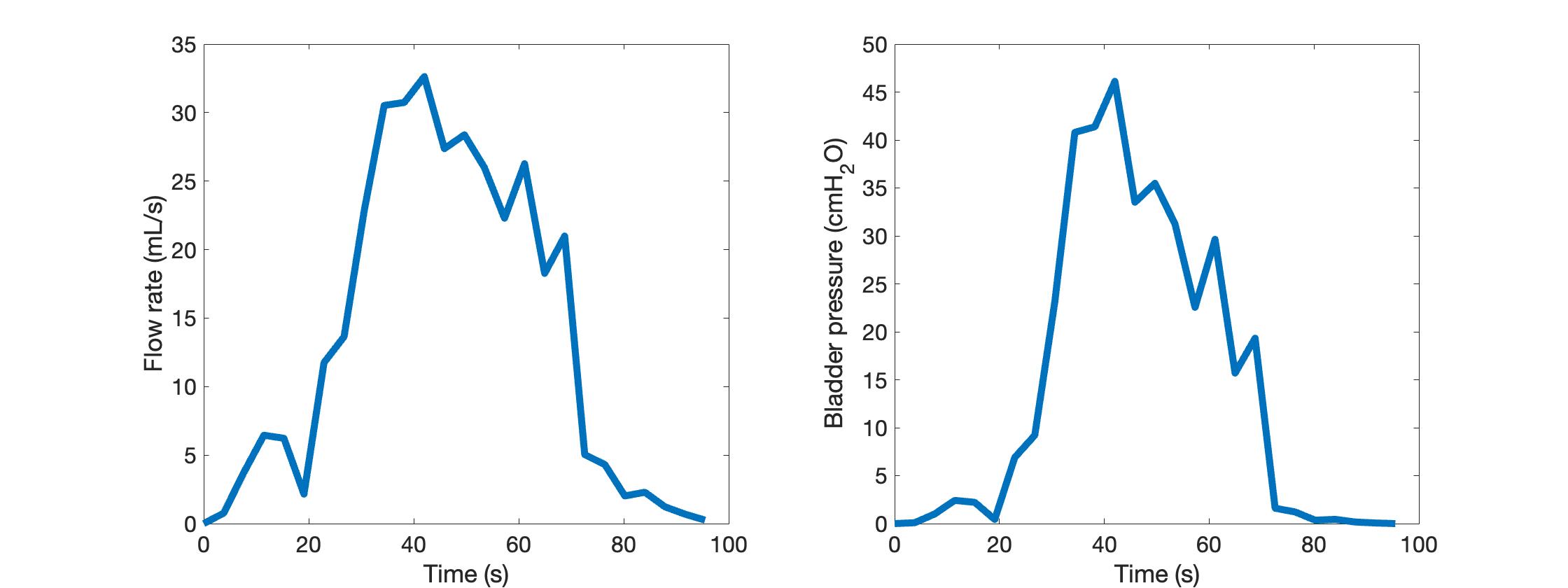
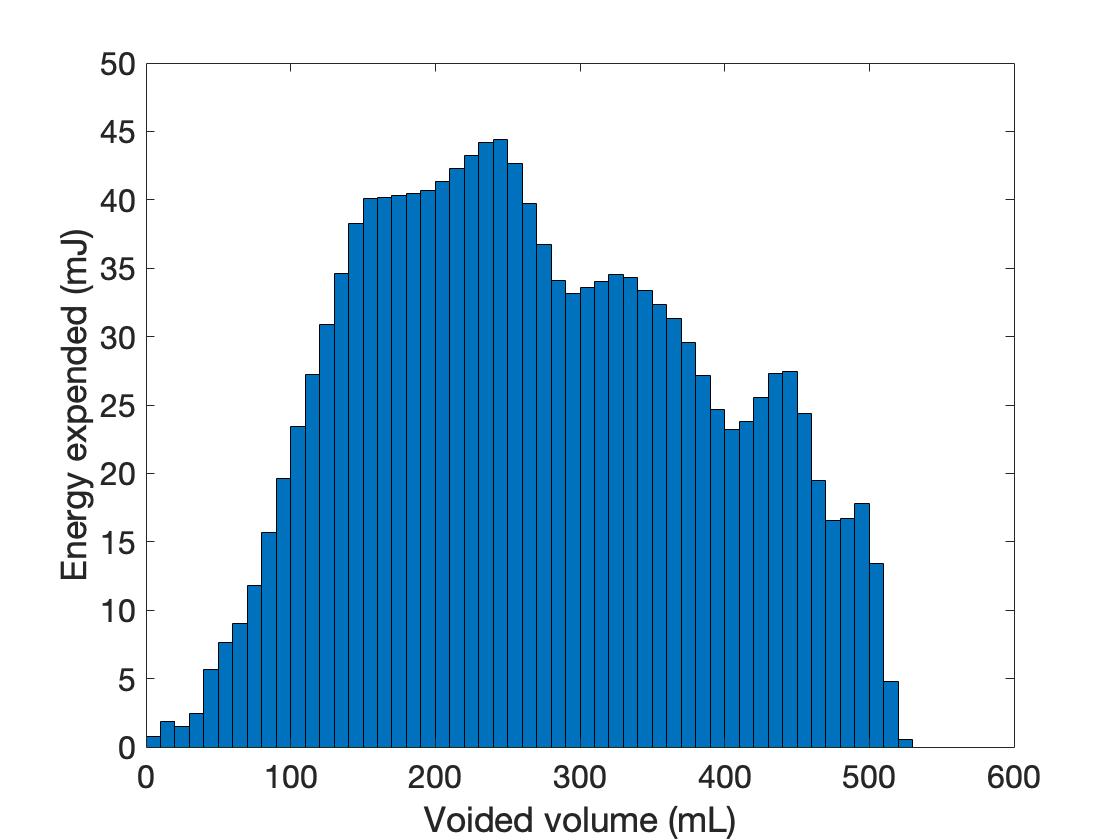
Successful image acquisition was obtained in the healthy subject where 3D dynamic images of the bladder and urethra during voiding were obtained in a single MRI session. The voided volume was 532 mL, post-void residual volume was 9 mL, and Qmax was 13.1 mL/s. Using the urethra anatomy and flow rate, we simulated flow in the urethra. The bladder anatomies were processed, and wall-motion driven CFD simulation of voiding were executed. Figure 3 shows the flow rate and bladder pressure during voiding. Figure 4 visualizes the velocity in the urethra and bladder. BOOI was 19.9 and BCI was 111.6. The total energy expended to void was 1391 mJ and Figure 5’s bar graph shows the amount of energy required to void every 10 mL of urine.Discussion
In clinical practice, bladder function, including BOOI and BCI, are assessed using invasive UDS. Previous work in our laboratory introduced a method that coupled 2D dynamic imaging and interpolation of bladder volumes with CFD to study bladder biomechanics6. Here, we introduced a fully three-dimensional MRI-based CFD method that enabled a non-invasive method to comprehensively characterize bladder biomechanics by quantifying and visualizing urodynamics. Execution of CFD simulations is a result of the successful surface mesh processing we developed. Our results show unobstructed bladder (BOOI < 20) and normal contractility (100 < BCI < 150) which agrees with the subject being healthy. To our knowledge, this is the first time 3D dynamic MRI was used to inform a bladder CFD simulation that quantifies BOOI and BCI non-invasively, and also the first time energy expended to void was calculated.Conclusion
The goal of this study was to implement a non-invasive methodology to comprehensively assess bladder biomechanics using MRI and CFD. To impose bladder motion in our CFD simulation, we processed the bladder anatomies at successive time points. This study successfully simulated, quantified, and visualized bladder voiding in one subject. Future studies would apply this procedure to multiple healthy and BPH/LUTS subjects, and validate urodynamic data against benchmark UDS.Acknowledgements
NIH R01 DK126850-01A1 and Wisconsin Partnership Program WPP; AAM3497
GE Healthcare which provides research support to the University of Wisconsin-Madison.
References
1. Roehrborn, C. G. Benign Prostatic Hyperplasia: An Overview. Rev Urol 7, S3 (2005).
2. Thorpe, A. & Neal, D. Benign prostatic hyperplasia. in Lancet vol. 361 1359–1367 (Elsevier, 2003).
3. Nitti, V. W. Pressure Flow Urodynamic Studies: The Gold Standard for Diagnosing Bladder Outlet Obstruction. Rev Urol 7, S14 (2005).
4. Blaivas, J. Multichannel urodynamic studies. Urology 23, 421–438 (1984).
5. Bushman, W. Etiology, Epidemiology, and Natural History. Urologic Clinics of North America vol. 36 403–415 Preprint at https://doi.org/10.1016/j.ucl.2009.07.003 (2009).
6. Pewowaruk, R. et al. A pilot study of bladder voiding with real-time MRI and computational fluid dynamics. PLoS One 15, e0238404 (2020).
Figures