4823
Intravoxel incoherent motion diffusion-weighted imaging in diagnosing perineural invasion status of rectal cancer: a histogram analysis study1Department of Radiology, The First Affiliated Hospital of Shandong First Medical University & Shandong Provincial Qianfoshan Hospital, Jinan, China, 2GE Healthcare,MR Research, Beijing, China, 3Department of General Surgery, The First Affiliated Hospital of Shandong First Medical University & Shandong Provincial Qianfoshan Hospital, Jinan, China
Synopsis
Keywords: fMRI Analysis, Diffusion/other diffusion imaging techniques, histogram analysis
Motivation: Currently, perineural invasion (PNI) of rectal cancer (RC) can only be confirmed by pathological examination of postoperative specimens.
Goal(s): It aimed to investigate the intravoxel incoherent motion (IVIM) diffusion-weighted imaging (DWI) in diagnosing the PNI status of RC by histogram analysis.
Approach: We extracted histogram features from 7 parametric maps derived from IVIM-DWI. The independent predictive histogram features of rectal cancer PNI were combined with the percentage of rectal wall
enclosure(PCI ) reported by MRI to construct a combined model for preoperative diagnosis of PNI.
Results: The AUC of the combined model is higher than that of each single-parameter model and histogram model.
Impact: This study demonstrated that full-volume histogram parameters basing on IVIM-DWI can be used to assess PNI status in rectal cancer. Histogram analysis, as a non-invasive tool, may be more valuable not only in rectal cancer research in the future.
Introduction
Rectal cancer (RC) with the same TNM-stage may have different responses and outcomes. Therefore, accurate and individualized treatment decisions need to be supported by additional prognostic factors 1 . Perineural invasion (PNI) has been proved to be significantly associated with high recurrence rate and low survival rate in RC patients3-5, and is a useful indicator to guide patients in choosing preoperative and postoperative adjuvant therapy 2,5-7. The morphologic MRI is however, unfortunately unable to determine PNI status. In comparison, IVIM, as a multi-b-value DWI, can provide quantitative parameters to reflect the microscopic characteristics of tumors sensitively than normal DWI8,such as predicting tumor deposition and differentiating between benign and malignant lymph nodes in RC 9-10. Meanwhile, texture analysis is a non-invasive analytic method to extract quantitative features from medical images, aiming to avoid subjective evaluation and achieve objective measurements of tumor heterogeneity11-14. Histogram features, used to describe the distribution of signal intensity values within tumor tissue, have higher reproducibility than higher-order texture features 12-15. It has been applied in a number of rectal cancer studies reported in literature. It remains unknown if combined IVIM and histogram analysis to diagnose PNI in RC. Therefore, the purpose of this study was to investigate the potential of IVIM-DWI-derived primary tumor-based whole-volume histogram parameters for assessing PNI status.Materials and Methods
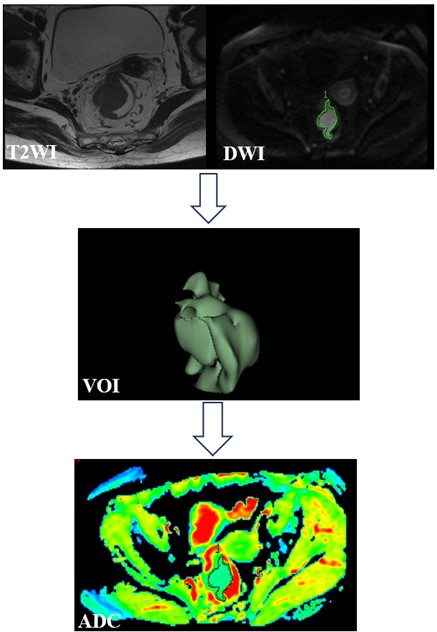
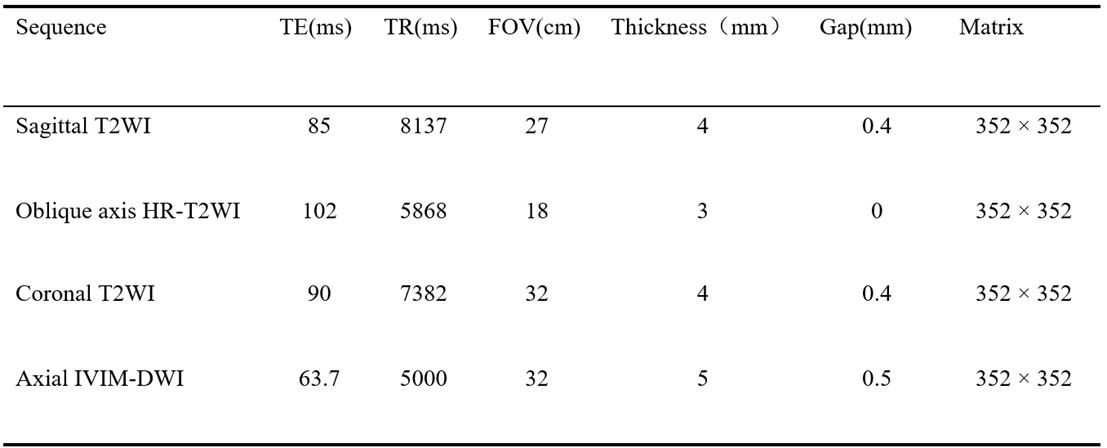
Patients 175 RC patients confirmed by postoperative pathology were enrolled. All patients underwent preoperative rectal MRI examinations within 2 weeks before surgery, including IVIM-DWI. PNI was assessed by pathological examination. Patients were divided into positive and negative groups based on PNI status. The clinical and MRI features of the study population were recorded accordingly. MRI acquisition All patients underwent MRI measurements on a 3.0 T system (Discovery 750w; GE Healthcare) using an eight-channel phased-array body coil in the supine position. Fast spin-echo (FSE)-based T2WI scans were first performed for anatomic imaging. According to the sagittal T2WI images, the IVIM-DWI scans in the axial view was performed using 11b-values. Image post-processing Two senior radiologists, who blinded to the pathological results, independently assessed the MRI findings of tumor. Six parameter maps (ADC, D, D *, f, DDC and α) from the three models of IVIM-DWI were derived in the vendor-provided software in GE advanced workstation 4.6. The whole tumor was manually drawn layer by layer on DWI (b value = 1000s / mm2 ) as VOI using the open source software 3D Slicer, and copied onto the parameter map to extract histogram features. Fig. 1 displays the process of tumor segmentation and feature extraction. Statistical analyses All statistical analyses were performed using MedCalc and SPSS software. Univariate and multivariate logistic regression analysis were used to identify the clinical risk factors significantly associated with PNI. Collinearity analysis was used to exclude parameters with severe collinearity in the univariate analysis. Receiver operating characteristic (ROC) curve analysis evaluated the diagnostic performance of each parameter and the combined model. DeLong test was used to compare the differences in AUC between each two models. P< 0.05 was considered statistical significance.Results
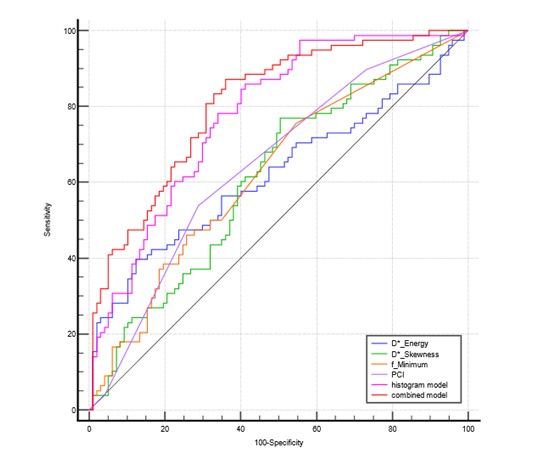
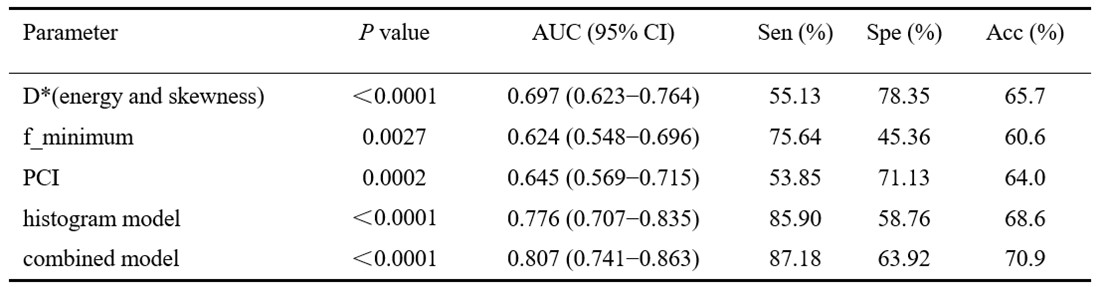
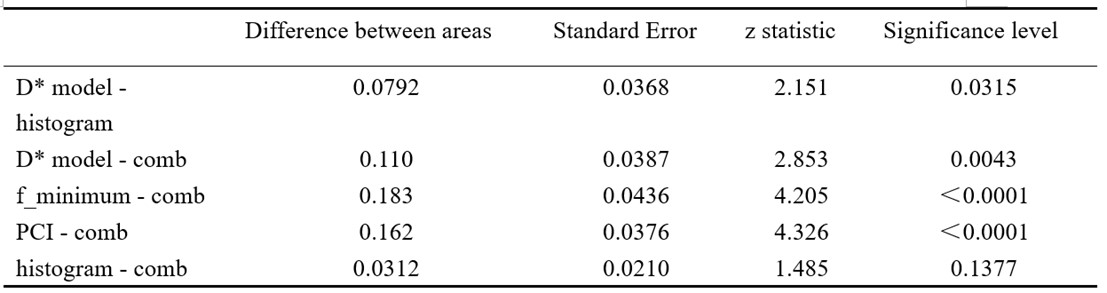
The percentage of rectal wall invasion(PCI)and 8 histogram features were significantly different between patients with positive and negative PNI. The collinearity diagnostic output results suggested that DWI_maximum and DWI_skewness had VIF values of greater than 10, indicating a non-negligible collinearity problem with other parameters, and thus were excluded. Multivariate logistic regression analysis further identified D*_energy, D*_skewness, f_minimum and PCI as independent risk factors for PNI status, and the values of histogram features were significantly higher in PNI positive than in PNI negative. A combined model was constructed from these four parameters. The AUC of the combined model was higher than that of the single-parameter model and the histogram model(D*_energy+D*_skewness+f_minimum). The Delong test showed that the AUC of the combined model was significantly different from that of each single-parameter model, and no significant difference was found with the histogram model. However, the sensitivity, specificity and accuracy of the combined model were improved compared with the histogram model. Detailed results were shown in Table2-3 and Fig. 2.Discussion and Conclusions
This study applied histogram parameters extracted from IVIM-DWI, combining clinic-radiologic features, to diagnose the status of PNI in rectal cancer. Multivariate analysis showed that D*_energy, D*_skewness, f_ minimum and PCI were independent risk factors for the status of PNI. The combined model constructed from these four parameters was validated with better diagnostic performance than any single parameters or clinic-radiologic features. In conclusion, this study demonstrated that full-volume histogram parameters basing on IVIM-DWI may help for assessing PNI status in rectal cancer.Acknowledgements
Over the course of my researching and writing this paper, I would like to express my thanks to all those who have helped me. Rong He: Data curation, Writing – original draft. Gesheng Song: Data curation, Writing – original draft. Junyi Fu: Investigation. Wenqiang Dou: Methodology, Software. Aiyin Li: Conceptualization, Writing – review & editing, Project administration. Jingbo Chen: Conceptualization, Writing – review & editing.References
1. Amin MB, Greene FL, Edge SB, et al. The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more "personalized" approach to cancer staging. CA Cancer J Clin 2017;67(2):93-99.
2. Stojkovic Lalosevic M, Milovanovic T, Micev M, et al. Perineural invasion as a prognostic factor in patients with stage I-III rectal cancer - 5-year follow up. World J Gastrointest Oncol 2020;12(5):592-600. 3. Kim S, Huh JW, Lee WY, et al. Lymphovascular invasion, perineural invasion, and tumor budding are prognostic factors for stage I colon cancer recurrence. Int J Colorectal Dis 2020;35(5):881-85.
4. Nikberg M, Chabok A, Letocha H, et al. Lymphovascular and perineural invasion in stage II rectal cancer: a report from the Swedish colorectal cancer registry. Acta Oncol 2016;55(12):1418-24.
5. Sung SY, Kim SH, Jang HS, et al. Pathologic Implications of Radial Resection Margin and Perineural Invasion to Adjuvant Chemotherapy after Preoperative Chemoradiotherapy and Surgery for Rectal Cancer: A Multi-Institutional and Case-Matched Control Study. Cancers (Basel) 2022;14(17).
6. Song JH, Yu M, Kang KM, et al. Significance of perineural and lymphovascular invasion in locally advanced rectal cancer treated by preoperative chemoradiotherapy and radical surgery: Can perineural invasion be an indication of adjuvant chemotherapy? Radiother Oncol 2019;133:125-31.
7. Kim CH, Yeom SS, Lee SY, et al. Prognostic Impact of Perineural Invasion in Rectal Cancer After Neoadjuvant Chemoradiotherapy. World J Surg 2019;43(1):260-72.
8. Le Bihan D, Breton E, Lallemand D, et al. MR imaging of intravoxel incoherent motions: application to diffusion and perfusion in neurologic disorders. Radiology 1986;161(2):401-7.
9. Hong Y, Song G, Jia Y, et al. Predicting tumor deposits in patients with rectal cancer: Using the models of multiple mathematical parameters derived from diffusion-weighted imaging. Eur J Radiol 2022;157:110573.
10. Zhao L, Liang M, Yang Y, et al. Histogram models based on intravoxel incoherent motion diffusion-weighted imaging to predict nodal staging of rectal cancer. Eur J Radiol 2021;142:109869.
11. Gatenby RA, Grove O, Gillies RJ. Quantitative imaging in cancer evolution and ecology. Radiology 2013;269(1):8-15. 12. Castellano G, Bonilha L, Li LM, et al. Texture analysis of medical images. Clin Radiol 2004;59(12):1061-9.
13. Davnall F, Yip CS, Ljungqvist G, et al. Assessment of tumor heterogeneity: an emerging imaging tool for clinical practice? Insights Imaging 2012;3(6):573-89.
14. Wan L, Peng W, Zou S, et al. Predicting perineural invasion using histogram analysis of zoomed EPI diffusion-weighted imaging in rectal cancer. Abdom Radiol (NY) 2022;47(10):3353-63.
15. Gourtsoyianni S, Doumou G, Prezzi D, et al. Primary Rectal Cancer: Repeatability of Global and Local-Regional MR Imaging Texture Features. Radiology 2017;284(2):552-61.
Figures