4822
Quantitative Imaging Habitat Risk Score (HRS) Combined with PI-RADSv2 Improves Predictive Value of Prostate Lesion Identification on mpMRI1Department of Radiation Oncology, University of Miami Miller School of Medicine, Miami, FL, United States, 2Department of Urology, University of Miami Miller School of Medicine, Miami, FL, United States, 3Department of Radiology, University of Miami Miller School of Medicine, Miami, FL, United States, 4Department of Pathology, University of Miami Miller School of Medicine, Miami, FL, United States
Synopsis
Keywords: Software Tools, Cancer
Motivation: Discrimination between true and false positive targets identified using PI-RADSv2 is needed to avoid unnecessary biopsies.
Goal(s): To investigate how quantitative analysis of prostate mpMRI through Habitat Risk Scoring (HRS) combined with PI-RADS can improve prostate lesion identification compared to using PI-RADS alone.
Approach: In prospective clinical trials lesions identified by PI-RADS and/or HRS were targeted through MRI/ultrasound fusion biopsies.
Results: Using HRS yields 100% NPV in the PI-RADS 3 cohort and increases PPV by 7.4% in the PI-RADS 4-5 cohort with respect to clinically significant cancer. Overall, the NPV and PPV increased by 21.4% and 13.2% respectively.
Impact: We present a quantitative imaging approach to complement the current standard for assessing prostate cancer risk in mpMRI data and demonstrate that the use of HRS strengthens fidelity in both positive and negative detections.
Introduction
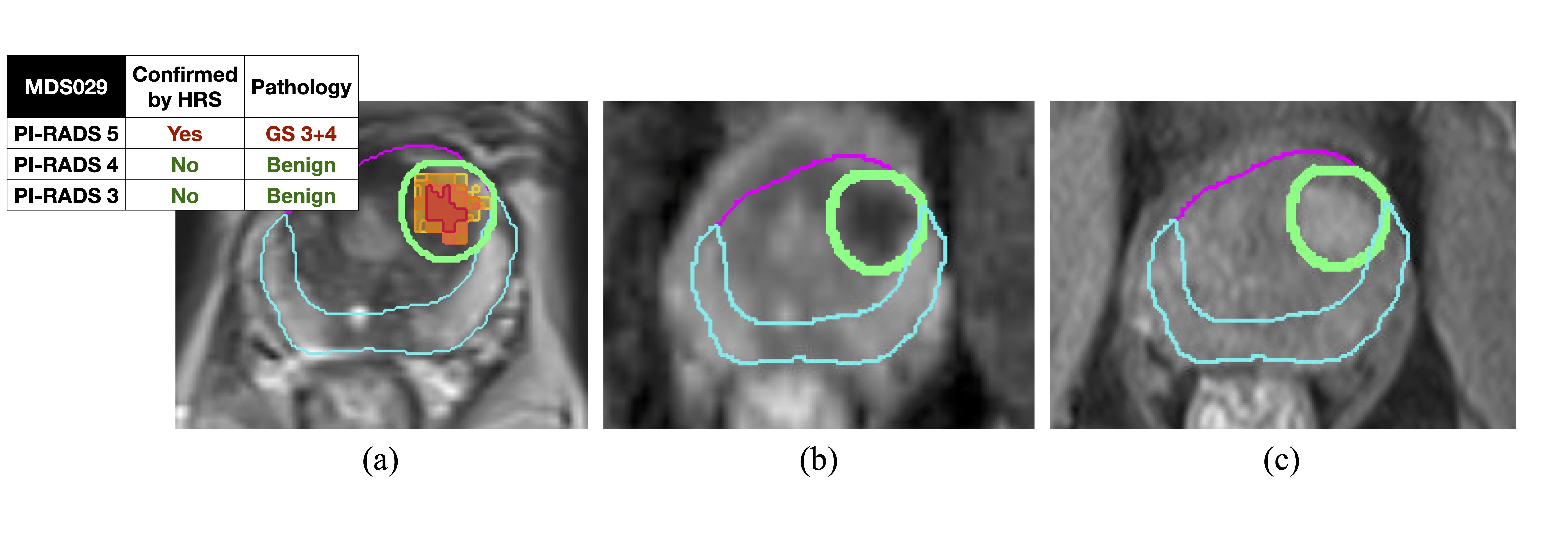
The Prostate Imaging Reporting and Data System (PI-RADS)1 harmonizes the interpretation of prostate multiparametric MRI (mpMRI) and is currently the standard of care format for assigning biopsy targets. A region-of-interest is assigned a score on a 5-point category scale based on the probability that a combination of findings on T2-weighted sequences, diffusion-weighted MRI and dynamic contrast-enhanced MRI correlates with the presence of clinically significant prostate cancer (csPCa), defined as Gleason Score (GS) ≥ 3+4, at that location2. The PI-RADS 3 category signifies equivocal presence of csPCa3, with a csPCa prevalence of only 32%4, causing many unnecessary biopsies. In addition, PI-RADS is susceptible to low inter-reader agreement (<50%)5,6. Quantitative mpMRI analysis may offer ways to combat the current shortcomings of PI-RADS. Our group has previously developed the prostate tumor habitat risk scoring (HRS) system7,8 by correlation with Gleason score (GS) from radical prostatectomy. The HRS algorithm assigns pixel-by-pixel risk on a 10-point scale based on diffusion through ADC sequences and perfusion through DCE sequences and displays HRS as a heat map overlaid on T2-weighted MRI (Figure 1).Materials and Methods
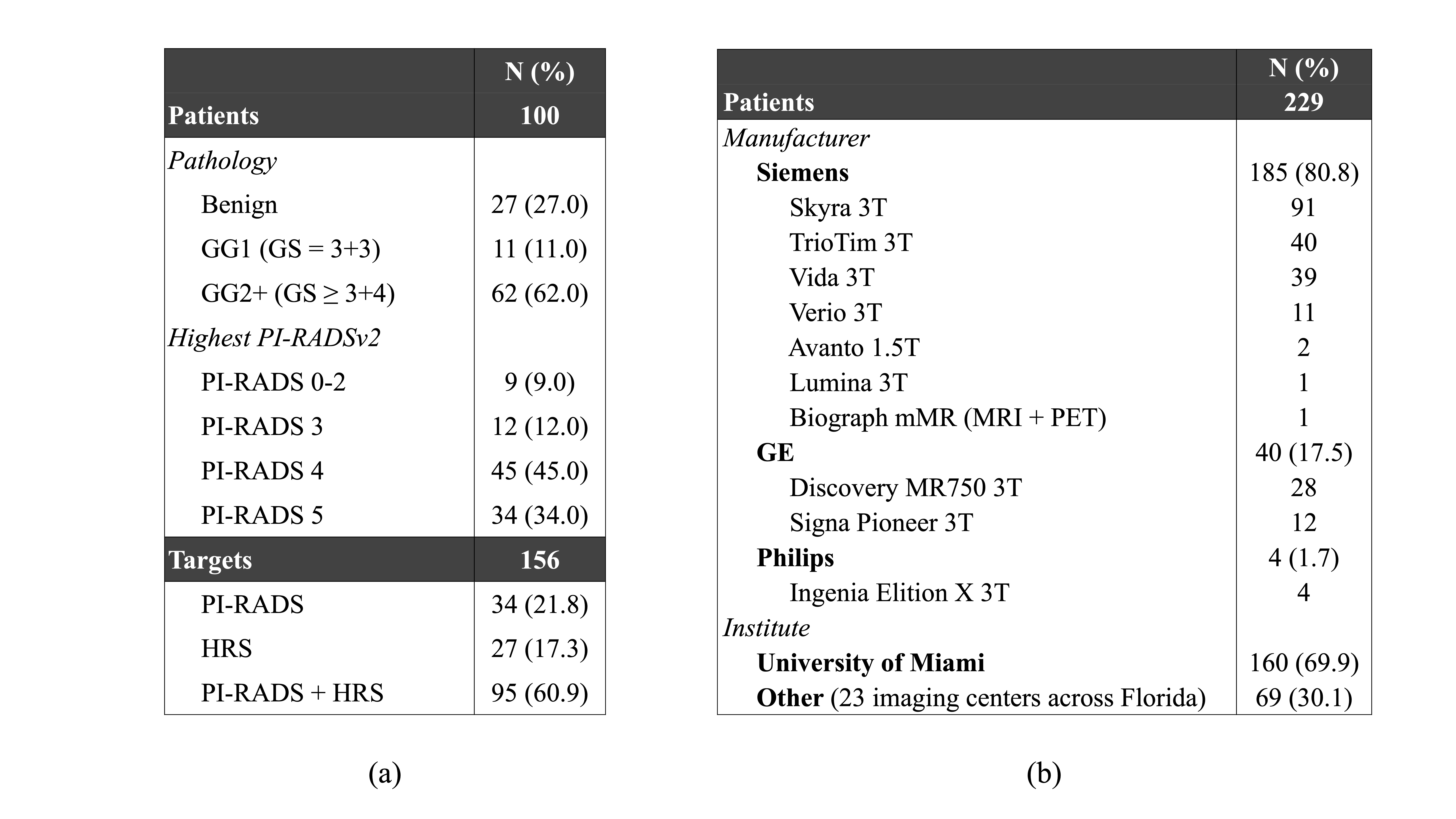
The Marker Driven Selection of Patients for Prostate Biopsy and Management (MDSelect) trial (NCT04240327) aims to investigate if the interpretation of mpMRI with the HRS algorithm combined with PI-RADS version 2 (PI-RADSv2) is more effective at detecting prostate cancer than PI-RADSv2 alone. MpMRI and MRI/ultrasound fusion biopsy data from 100 patients enrolled in the MDSelect trial, with 156 identified targets, were analyzed. The pathology prevalence and highest PI-RADS score among the patients are displayed in Table 1a along with the target category distribution of the individual targets, with the categories being PI-RADS – targets identified only by PI-RADSv2, (ii) HRS – targets identified only by the HRS algorithm, (iii) PI-RADS + HRS – targets identified both by PI-RADSv2 and HRS. The trial mpMRI data were collected on 10 different scanner models at 24 centers across South Florida (Table 1b). The dataset was stratified into three study cohorts based on the highest PI-RADS assessment category per patient: PI-RADS 0-2 (no to low level of suspicion of csPCa), PI-RADS 3 (intermediate level of suspicion of csPCa) and PI-RADS 4-5 (high to very high level of suspicion of csPCa). The PPV and NPV in each cohort was computed to assess the value of HRS when combined with PI-RADSv2.Results
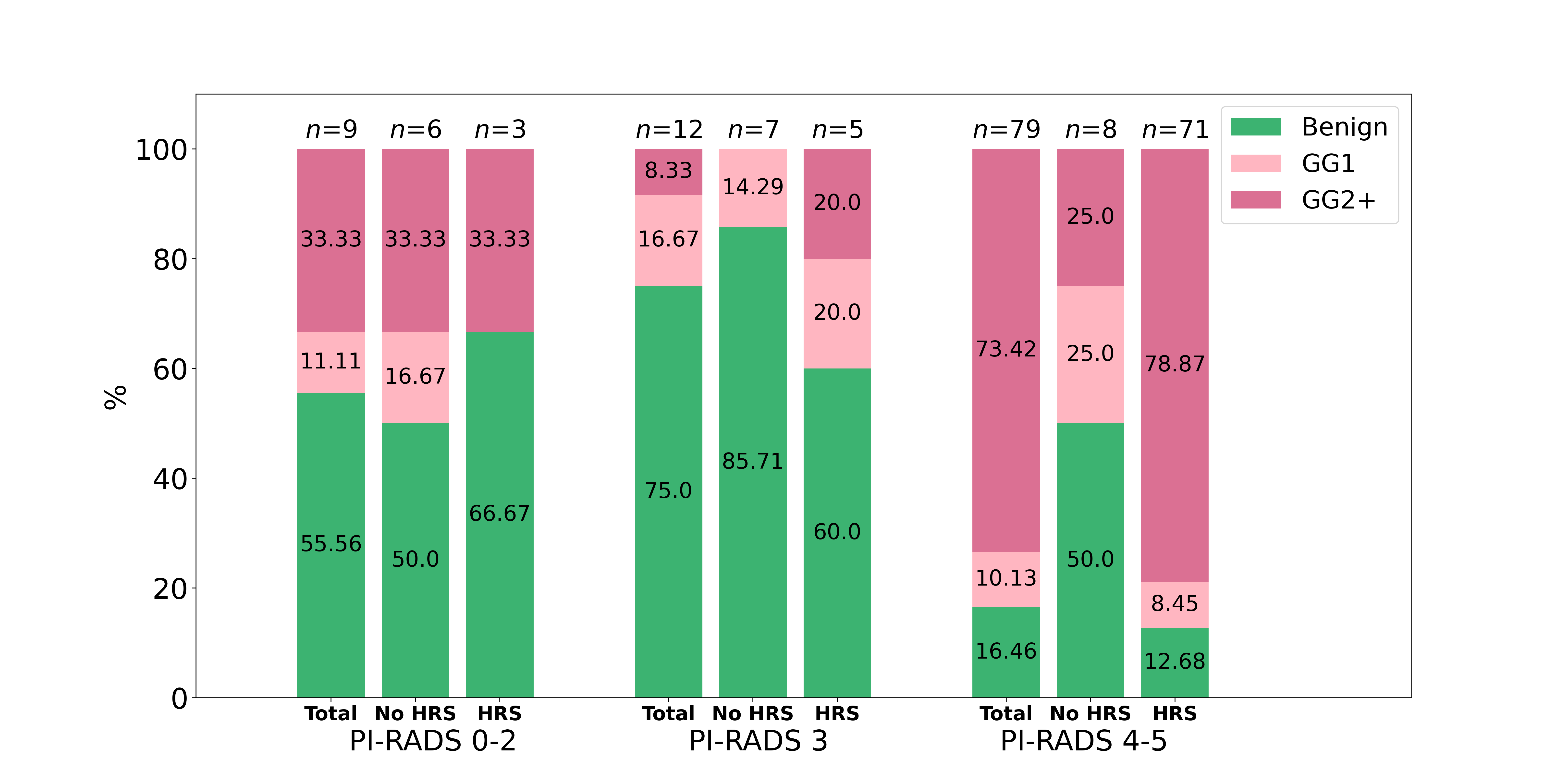
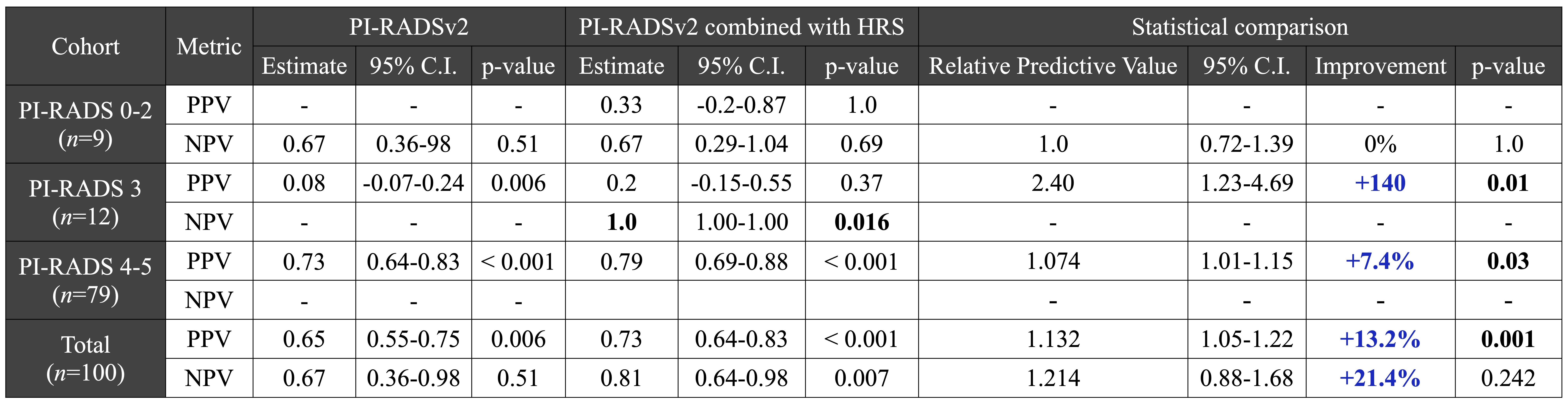
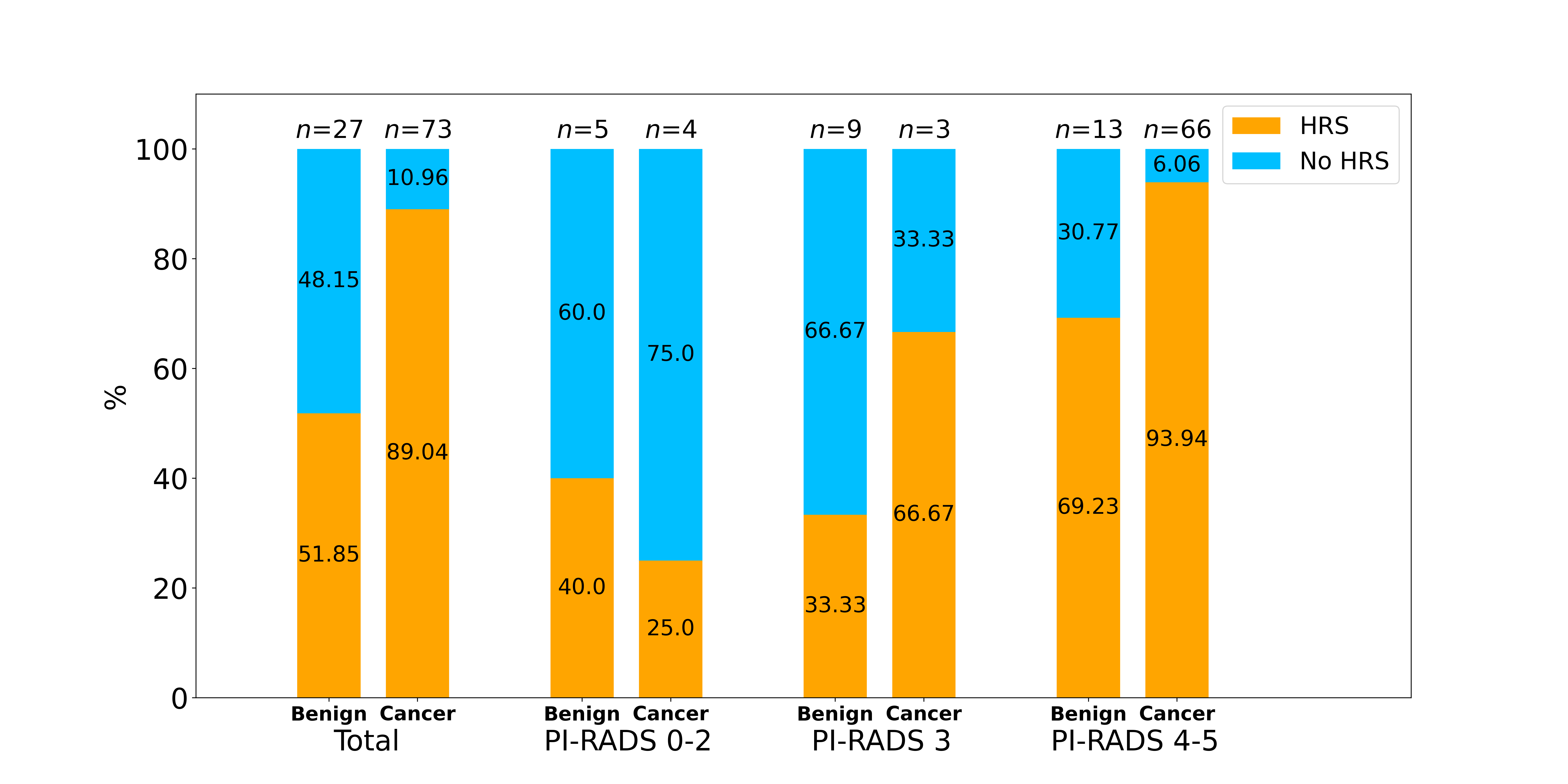
Figure 2 shows HRS to better discriminate between true and false positives than PI-RADS alone when PI-RADS ≥ 3, and that HRS in combination with PI-RADS increases both PPV and NPV in these cohorts. Table 2 demonstrates that the NPV in the PI-RADS 3 cohort is 100% and that the PPV in the PI-RADS 4-5 cohort increases with 7.4% with respect to clinically significant cancer when combined with HRS. Considering the total dataset, the PPV and NPV improvements are 13.2% and 21.4% respectively. Figure 3 shows that HRS in combination with PI-RADS has potential to reduce the number of biopsies with benign outcome by 66.7% for patients with a maximum PI-RADS 3.Discussion
HRS is powerful in discriminating between true and false positive targets identified by PI-RADSv2 and can reliably analyze data from a variety of magnets, which indicates the readiness of the software to be incorporated in a clinical setting (Table 1b). In addition to the high NPV and PPV, there is a promising trend observed in the potential of HRS to reduce the number unnecessary biopsies, although not yet established with statistically significance due to the size of the PI-RADS 3 cohort.The false detections (5/9) in the small PI-RADS 0-2 cohort can be attributed to: (i) false negatives due to few positive cores of low-grade cancer (3/3 GS ≤ 3+4, 2/3 only one positive core) (ii) false positives identified in the transition zone (2/2), which is more susceptible to false HRS detections as well as an area with higher likelihood of biopsy target misses and therefore more prone to true positives being interpreted as false positives. In addition to 3 true negatives detections, this cohort also contained 1 true positive with GS 4+3, which would have remained undetected without HRS as all systematic cores were benign.
Conclusions
Using HRS in combination with PI-RADSv2 to interpret prostate mpMRI data strengthens both NPV and PPV, and specifically provides high NPV in the PI-RADS 3 cohort while significantly improving PPV in the PI-RADS 4-5 cohort. Thus, HRS could assist clinical decision-making, both to increase confidence in identifying csPCa as well as to safely reduce the number of repeat biopsies in patients with benign pathology or low-risk cancer.Acknowledgements
The research was supported by the National Cancer Institute of the National Institutes of Health under Award Number P30CA240139, RO1CA189295, R01CA190105, and U01CA239141.References
1. Barentsz JO, Richenberg J, Clements R, et al. ESUR prostate MR guidelines 2012. Eur Radiol. 2012;22(4):746-757
2 Steiger P, Thoeny HC. Prostate MRI based on PI-RADS version 2: how we review and report. Cancer Imaging. 2016 Apr 11;16:9. doi: 10.1186/s40644-016-0068-2. PMID: 27067275; PMCID: PMC4828836.
3 Schoots IG. MRI in early prostate cancer detection: how to manage indeterminate or equivocal PI-RADS 3 lesions? Transl Androl Urol. 2018 Feb;7(1):70-82. doi: 10.21037/tau.2017.12.31. PMID: 29594022; PMCID: PMC5861283.
4 Camacho A, Salah F, Bay CP, et al. PI-RADS 3 score: A retrospective experience of clinically significant prostate cancer detection. BJUI Compass. 2023 Apr 11;4(4):473-481. doi: 10.1002/bco2.231. PMID: 37334024; PMCID: PMC10268585.
5 Rosenkrantz AB, Ginocchio LA, Cornfeld D, et al. Interobserver reproducibility of the PI-RADS version 2 lexicon: a multicenter study of six experienced prostate radiologists. Radiology. 2016 Sep;280(3):793-804.
6 Westphalen AC, McCulloch CE, Anaokar JM, et al. Variability of the positive predictive value of PI-RADS for prostate MRI across 26 centers: experience of the society of abdominal radiology prostate cancer disease-focused panel. Radiology. 2020 Jul;296(1):76-84.
7 Tschudi Y, Pollack A, Punnen S, et al. Automatic Detection of Prostate Tumor Habitats using Diffusion MRI. Sci Rep. 2018 Nov 14;8(1):16801. doi: 10.1038/s41598-018-34916-4. PID: 30429515; PMCID: PMC6235961.
8Stoyanova R, Chinea F, Kwon D, et al. An Automated Multiparametric MRI Quantitative Imaging Prostate Habitat Risk Scoring System for Defining External Beam Radiation Therapy Boost Volumes. Int J Radiat Oncol Biol Phys. 2018 Nov 15;102(4):821-829. doi: 10.1016/j.ijrobp.2018.06.003. Epub 2018 Jun 13. PMID: 29908220; PMCID: PMC6245650.
9 Moskowitz CS, Pepe MS. Comparing the predictive values of diagnostic tests: sample size and analysis for paired study designs. Clin Trials. 2006;3(3):272-9. doi: 10.1191/1740774506cn147oa. PMID: 16895044.
Figures