4816
Bi-regional quantitative DCE-MRI for prediction of microvascular invasion in hepatocellular carcinoma and its significance for treatment1Department of Diagnostic Radiology, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China, 2Department of Pathology, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China, 3Department of Hepatobiliary Surgery, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China, 4GE Healthcare, MR Research China, Beijing, China
Synopsis
Keywords: Liver, Liver
Motivation: Accurately predicting microvascular invasion (MVI) risk in hepatocellular carcinoma before surgery could aid clinicians in selecting appropriate surgical approaches to improve the patient’s prognosis.
Goal(s): To construct DCE-MRI based nomogram for predicting MVI, and to assess its ability for stratifying the risk of recurrence after hepatectomy and guiding surgical approaches.
Approach: Quantitative DCE-MRI parameters from both intra-tumoral region (ITR) and peritumoral region (PTR), along with clinical-radiological (CR) features, were utilized to establish the nomogram.
Results: The nomogram presented AUC values of 0.966 in the training and 0.937 in the validation set for predicting MVI. High-risk patients could obtain survival benefit from anatomical resection.
Impact: We constructed and evaluated the performance of the bi-regional quantitative DCE-MRI based nomogram for predicting MVI risk in HCC. Our predictive model effectively predicts MVI risk and assists clinicians in selecting appropriate therapeutic strategies for patients.
Introduction
Prediction of microvascular invasion (MVI) in hepatocellular carcinoma (HCC) preoperatively is challenging but essential for reducing tumor recurrence [1-3]. Preoperative assessments of MVI via various imaging modalities mainly focused on features inside of tumor, while the peritumoral region (PTR) have been less explored [4, 5]. Quantitative dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) can provide tissue perfusion information [6, 7]. However, nomogram based on DCE-MRI perfusion parameters from both intra-tumoral region (ITR) and PTR has not been explored until now. Anatomical resection (AR) has the potential to improve the prognosis of individuals administered hepatectomy for HCC compared with non-anatomical resection (NAR) [8]. But not all HCC patients could benefit from AR. Consequently, whether the nomogram could represent a novel biomarker to identify patients who may benefit from AR was underexamined. Therefore, we aimed to construct a nomogram based on quantitative DCE-MRI parameters and clinical-radiological features for predicting MVI, and to assess its ability for stratifying the risk of recurrence after hepatectomy and guiding hepatectomy approaches.Methods
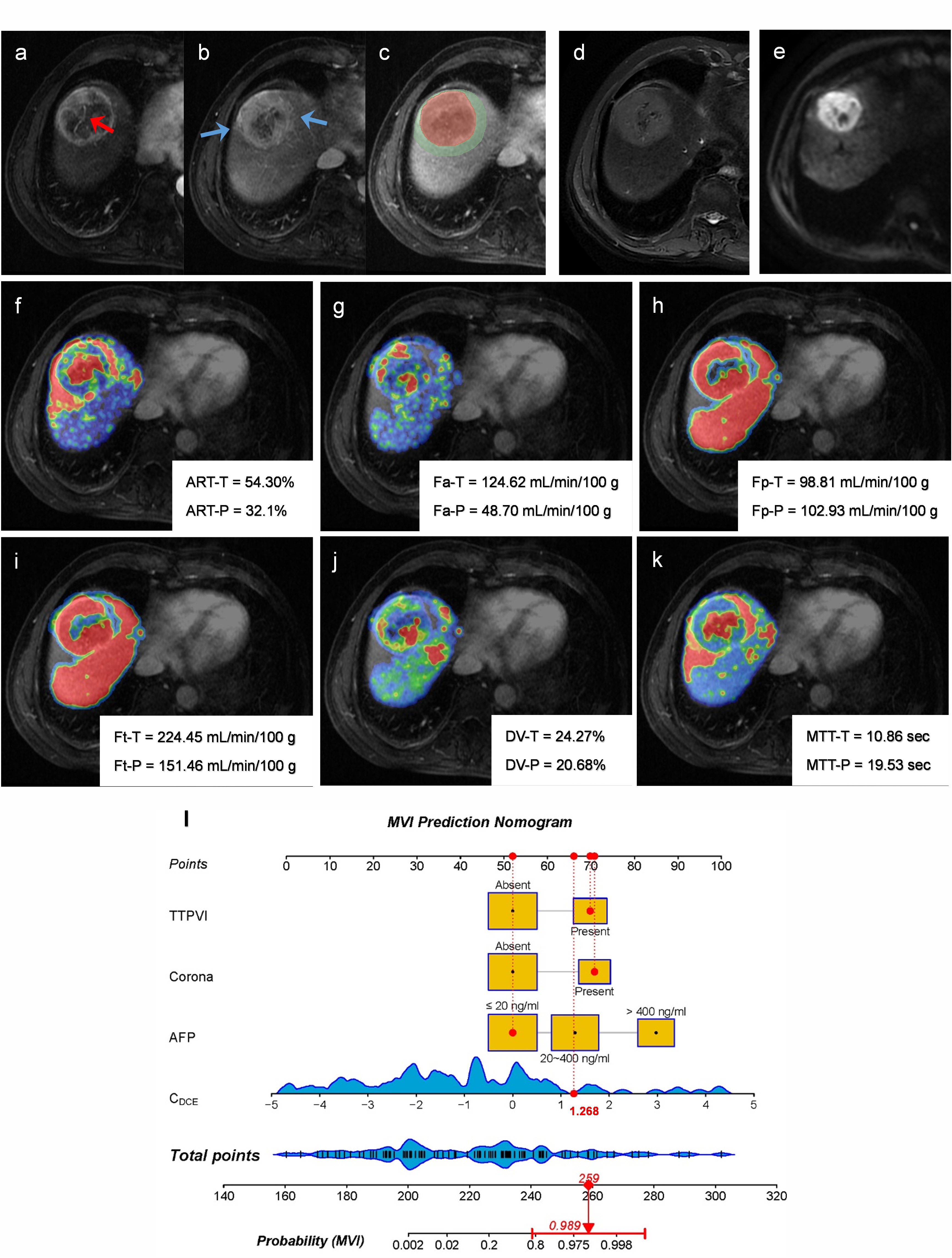
A total of 133 patients with solitary HCC less than 5.0 cm were prospective collected. The patients were randomly divided into training (n = 93) and validation set (n = 40). All patients underwent contrast enhanced MR examination on a 3.0T MRI system (SIGNATM Architect, GE Healthcare, Milwaukee, WI, USA) before hepatectomy. Quantitative DCE-MRI was performed by using LAVA-XV sequence with breath-hold. According to our previous study [9], a dynamic scan with 42 consecutive phases was performed with a temporal resolution of 6 s/phase. The DCE perfusion analysis was performed on MATLAB R2018b (Mathworks, Natick, MA, USA). A dual-input single compartment model was used to fit the time activity curves [9]. The following pseudocolor maps of the perfusion parameters were generated: arterial fraction (ART, %), arterial flow (Fa, mL/min/100 g), portal venous flow (Fp, mL/min/100 g), total blood flow (Ft, mL/min/100 g), distribution volume (DV, %), and mean transit time (MTT, s). Perfusion parameters of ITR and 10 mm PTR were extracted (Figure 1). All statistical analyses were conducted using R software. Multivariate logistic regression analyses were performed to construct the combined model for MVI prediction. The receiver operating characteristic (ROC) curve was performed to evaluate the prediction performance. Survival curves of different risk groups and surgical approaches were calculated by Kaplan-Meier method and compared by log-rank test.Results
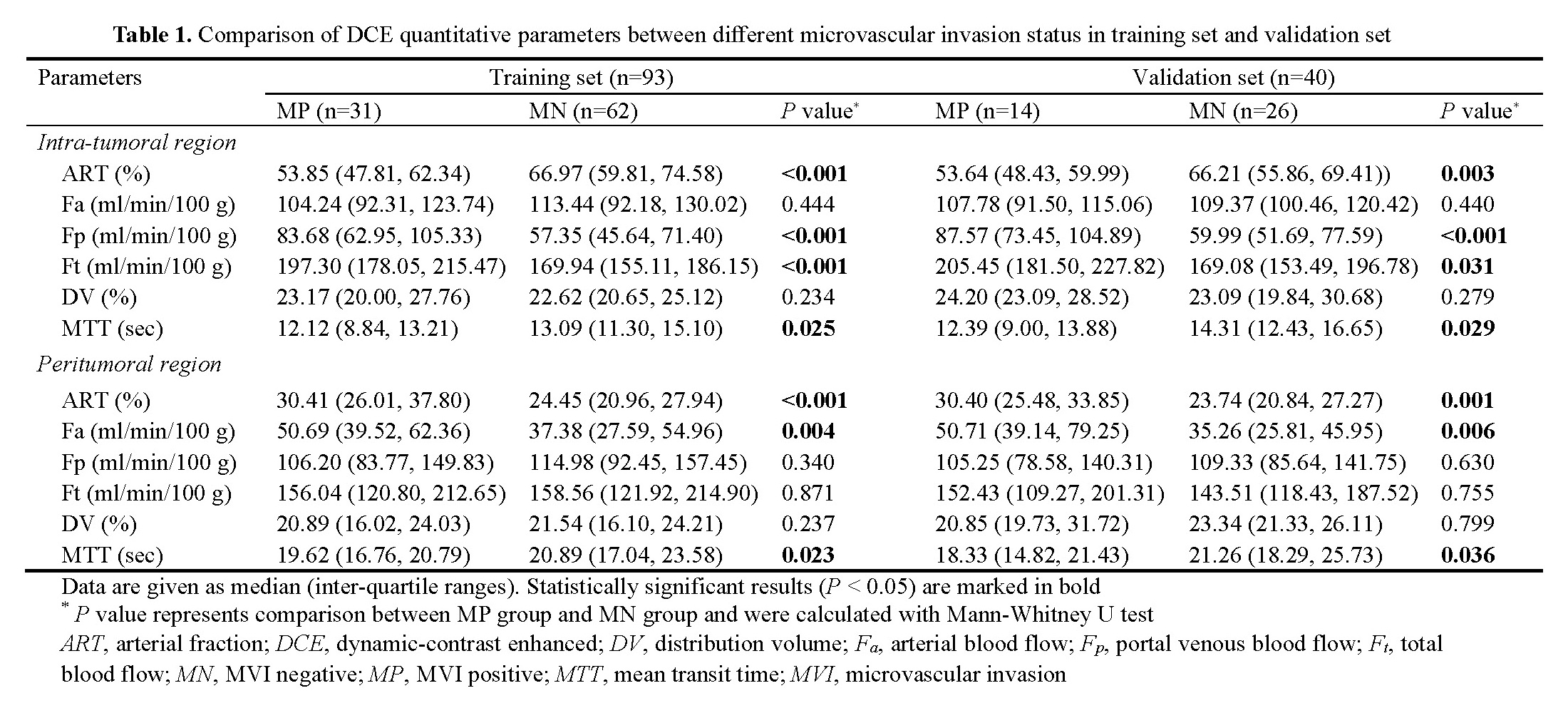
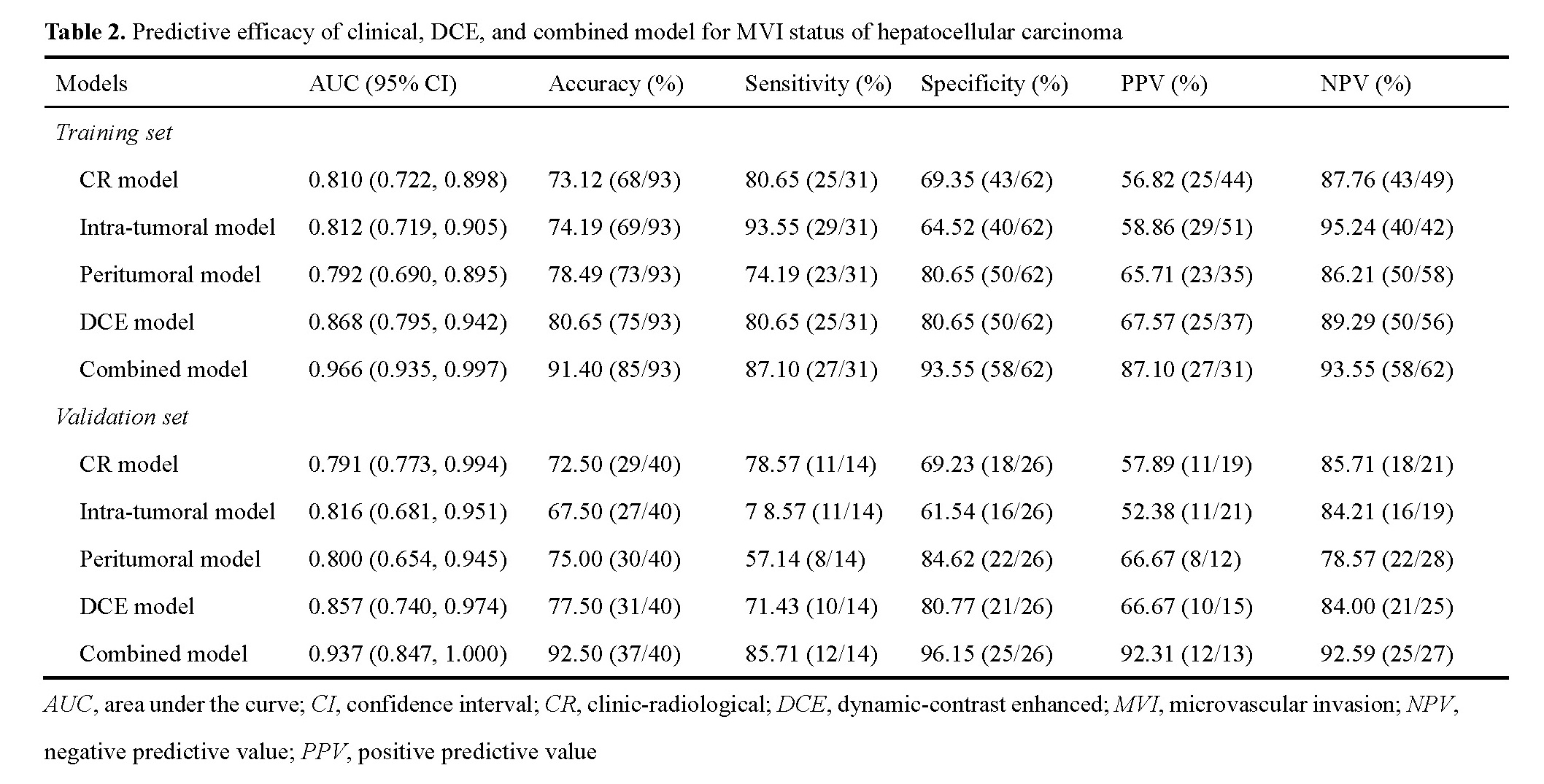
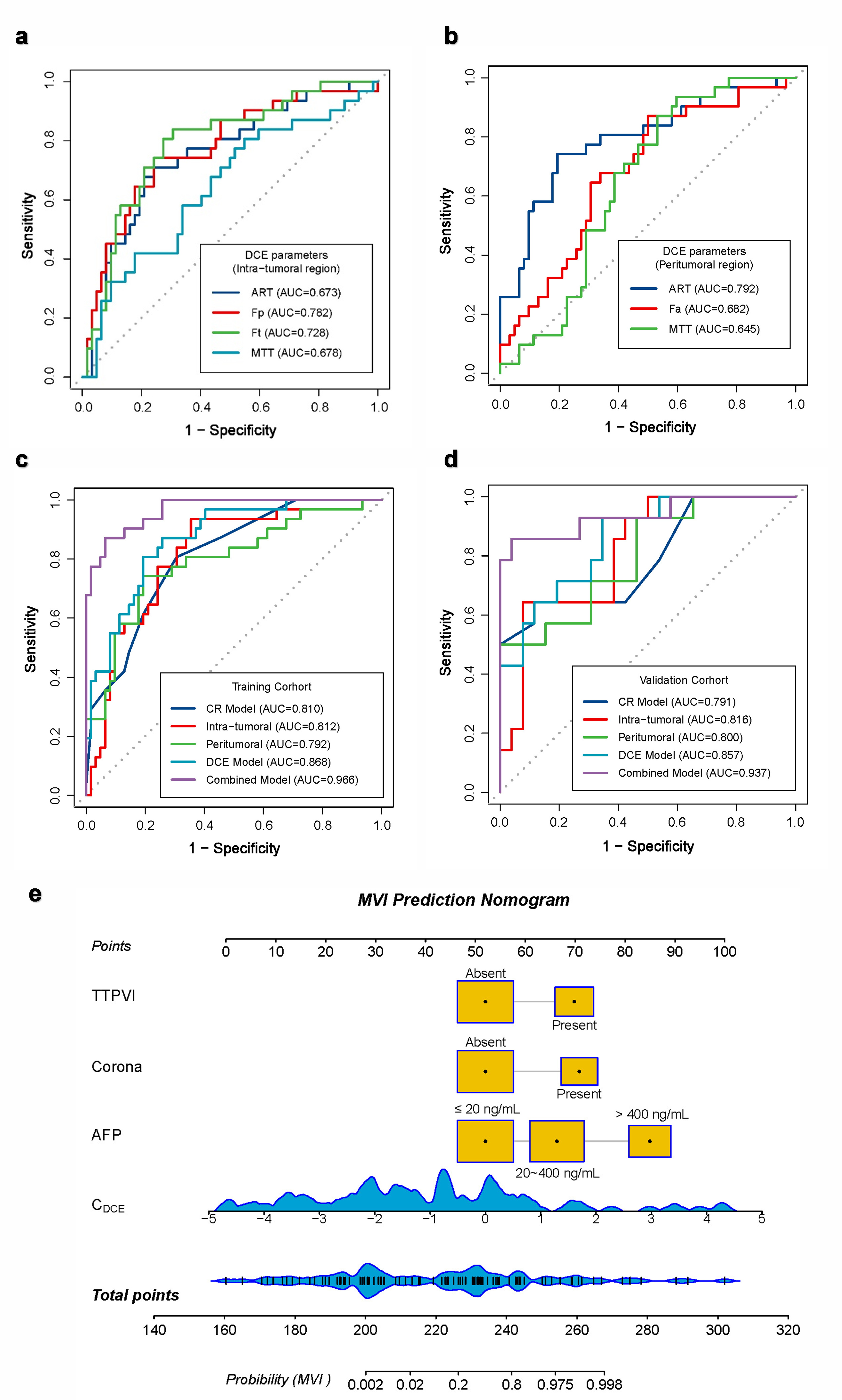
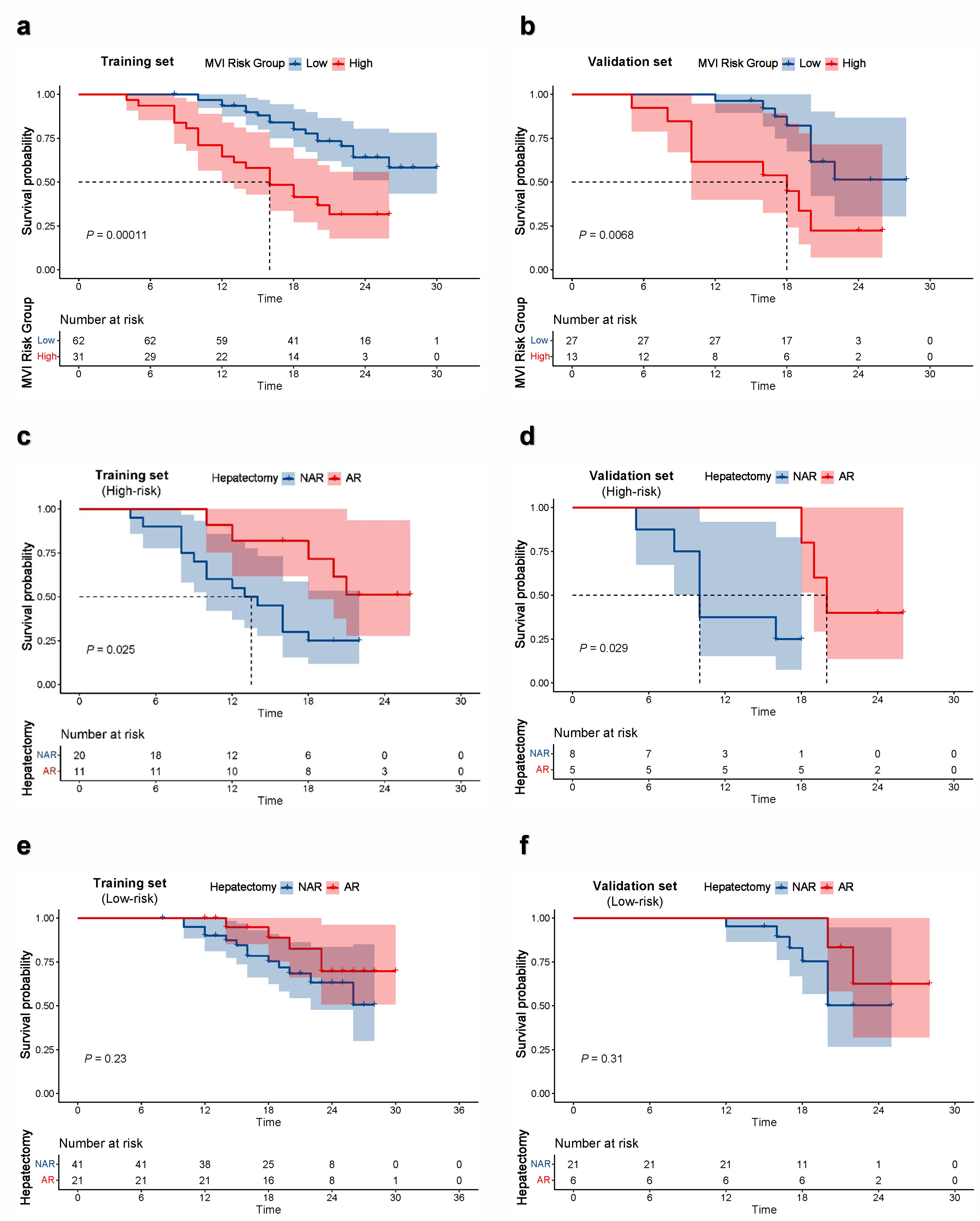
Of the 133 HCC patients enrolled in this study, 34.44% (31/90) in the training set and 35.00% (14/40) in the validation set were MVI-positive (MP). AFP, corona enhancement, and two-trait predictor of venous invasion (TTPVI) were demonstrated as the independent risk factors for MVI. The comparison of quantitative DCE-MRI parameters between MP group and MVI-negative (MN) groups are summarized in Table 1. The predictive performance of models was described in Table 2 and Figure 2. Example of HCC with MVI positive is shown in Figure 1. The AUC of the combined model were 0.966 in the training set and 0.937 in the validation set, respectively. The median RFS of high-risk of MVI group was significant shorter than that of low-risk of MVI group. In terms of clinical benefit from different surgical approaches, patients with high-risk of MVI who received AR exhibited a better prognosis than those who received NAR (Figure 3). However, no significant difference between AR and NAR was observed in patients with low-risk group.Discussion
This study evaluated the DCE-MRI perfusion parameters derived from dual-input single-compartment model to discriminate MVI status in small solitary HCC. A combined nomogram was successfully constructed with a satisfactory predictive performance. The results suggest that the DCE-MRI perfusion parameters can be used to differentiate the MVI status preoperatively and noninvasively. Our result implied that the ITR and PTR might have different perfusion changes in different MVI status groups in HCC. Parameters in PTR could predict MVI status. This was consistent with the fact that peritumoral areas is the main site of MVI occurrence [1-3]. The tumor thrombus in peritumoral small vessels could influence the perfusion and hemodynamic of this liver parenchyma [10, 11]. In clinical practice, the combined ITR and PTR DCE-MRI perfusion parameters might improve the predictive performance in predicting MVI status compared with ITR or ITR alone. Kaplan-Meier survival analysis demonstrated that RFS could be stratified based on predicted MVI risk classification. For patients at high risk for MVI, implementing AR might yield greater survival benefits.Conclusion
Quantitative DCE-MRI perfusion parameters provide an efficient approach to predicting MVI status. The predicted MVI risk classification can stratify the risk of recurrence after radical hepatectomy and aid in selection of optimal surgical approaches.Acknowledgements
NoneReferences
[1] Rodríguez-Perálvarez M, Luong TV, Andreana L, Meyer T, Dhillon AP, Burroughs AK (2013) A systematic review of microvascular invasion in hepatocellular carcinoma: diagnostic and prognostic variability. Ann Surg Oncol 20(1):325-339
[2] Erstad DJ, Tanabe KK (2019) Prognostic and Therapeutic Implications of Microvascular Invasion in Hepatocellular Carcinoma. Ann Surg Oncol 26(5):1474-1493
[3] Lee S, Kang TW, Song KD, Lee MW, Rhim H, Lim HK, et al (2021) Effect of Microvascular Invasion Risk on Early Recurrence of Hepatocellular Carcinoma After Surgery and Radiofrequency Ablation. Ann Surg 273(3):564-571
[4] Zhu Y, Feng B, Cai W, Wang B, Meng X, Wang S, et al (2023) Prediction of Microvascular Invasion in Solitary AFP-Negative Hepatocellular Carcinoma ≤ 5 cm Using a Combination of Imaging Features and Quantitative Dual-Layer Spectral-Detector CT Parameters. Acad Radiol Suppl 1:S104-S116
[5] Zheng R, Zhang X, Liu B, Zhang Y, Shen H, Xie X, et al (2023) Comparison of non-radiomics imaging features and radiomics models based on contrast-enhanced ultrasound and Gd-EOB-DTPA-enhanced MRI for predicting microvascular invasion in hepatocellular carcinoma within 5 cm. Eur Radiol 33(9):6462-6472
[6] Cao Y, Wang X, Shi J, Zeng X, Du L, Li Q, et al (2023) Multiple parameters from ultrafast dynamic contrast-enhanced magnetic resonance imaging to discriminate between benign and malignant breast lesions: Comparison with apparent diffusion coefficient. Diagn Interv Imaging 104(6):275-283
[7] Huang N, Chen Y, She D, Xing Z, Chen T, Cao D (2022) Diffusion kurtosis imaging and dynamic contrast-enhanced MRI for the differentiation of parotid gland tumors. Eur Radiol 32(4):2748-2759
[8] Liu J, Zhuang G, Bai S, Hu Z, Xia Y, Lu C, et al (2023) The Comparison of Surgical Margins and Type of Hepatic Resection for Hepatocellular Carcinoma with Microvascular Invasion. Oncologist oyad124
[9] Zhu Y, Zhou Y, Zhang W, Xue L, Li Y, Jiang J, et al (2021) Value of quantitative dynamic contrast-enhanced and diffusion-weighted magnetic resonance imaging in predicting extramural venous invasion in locally advanced gastric cancer and prognostic significance. Quant Imaging Med Surg 11(1):328-340
[10] Li H (2021) Angiogenesis in the progression from liver fibrosis to cirrhosis and hepatocelluar carcinoma. Expert Rev Gastroenterol Hepatol 15(3):217-233
[11] Pandharipande PV, Krinsky GA, Rusinek H, Lee VS (2005) Perfusion imaging of the liver: current challenges and future goals. Radiology 234(3):661-673
Figures