4810
Working Memory Prognostication After Concussion Using Glymphatic Biomarkers1Neuroscience Research Center, Taipei Medical University, Taipei, Taiwan, 2Translational Imaging Research Center, Taipei Medical University Hospital, Taipei, Taiwan
Synopsis
Keywords: Traumatic Brain Injury, Traumatic brain injury, concussion; glymphatic function; cerebral microbleeds; sleep disorder; cognitive impairment; machine learning
Motivation: Addressing persistent working-memory decline (PWMD) in concussion patients is crucial, but prognostic methods are limited. This study explores the potential of the glymphatic system as a novel biomarker.
Goal(s): Determine if early measurement of glymphatic dysfunction within 1 month post-concussion can predict PWMD.
Approach: A 1-year prospective observational study was conducted, assessing glymphatic function, microhemorrhage, sleep quality, and neurocognitive tests within 1-month of injury.
Results: Significant correlations were found between 1-year digit span scores and glymphatic diffusivity and sleep quality. Lower glymphatic function and poor sleep quality correlated with unfavorable long-term working memory outcomes. The 1-year digit span score could be reliably predicted.
Impact: This research highlights the importance of monitoring sleep quality and glymphatic function, offering potential therapeutic targets to prevent persistent working-memory decline in concussion patients.
Introduction
Concussions, or mild traumatic brain injuries (mTBI), often result in postconcussive symptoms, including cognitive deficits [1-3] and sleep disturbances [4-6]. Approximately half of mTBI patients experience persistent postconcussive working memory decline (PWMD), which negatively impacts their quality of life [1-3]. However, the underlying causes remain unclear, limiting diagnostic and prognostic approaches. This study aims to explore the potential of glymphatic function as diagnostic and prognostic biomarkers for PWMD. We further investigate the relationships between cerebral microbleeds (CMBs), sleep quality, glymphatic functionality, and long-term PWMD following mTBI.Method
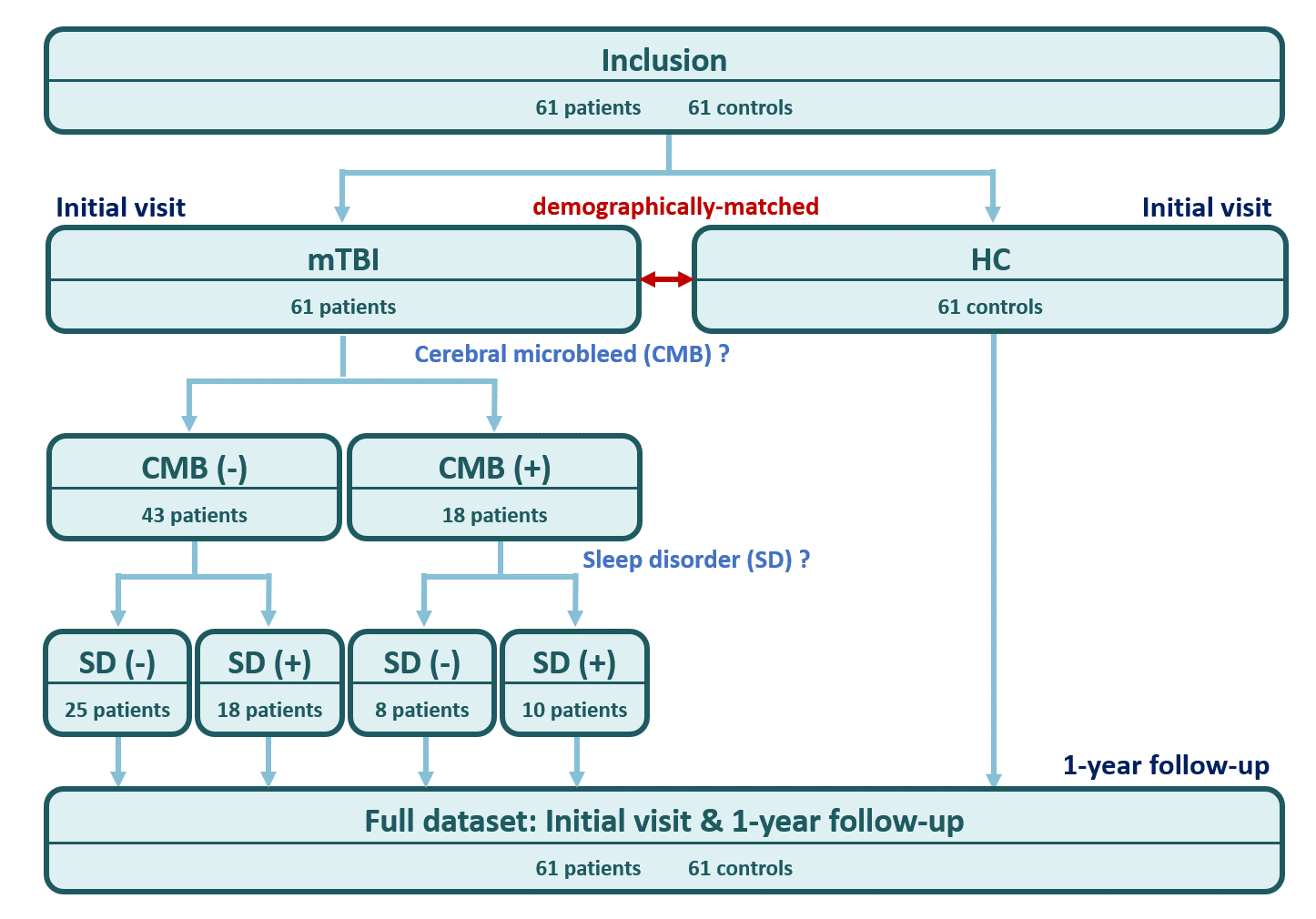
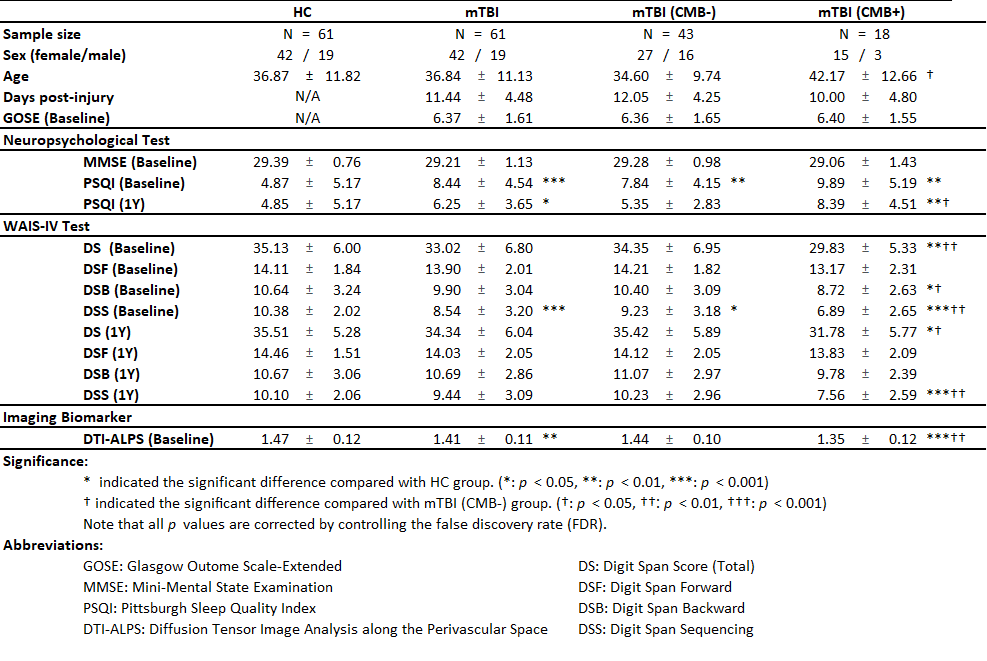
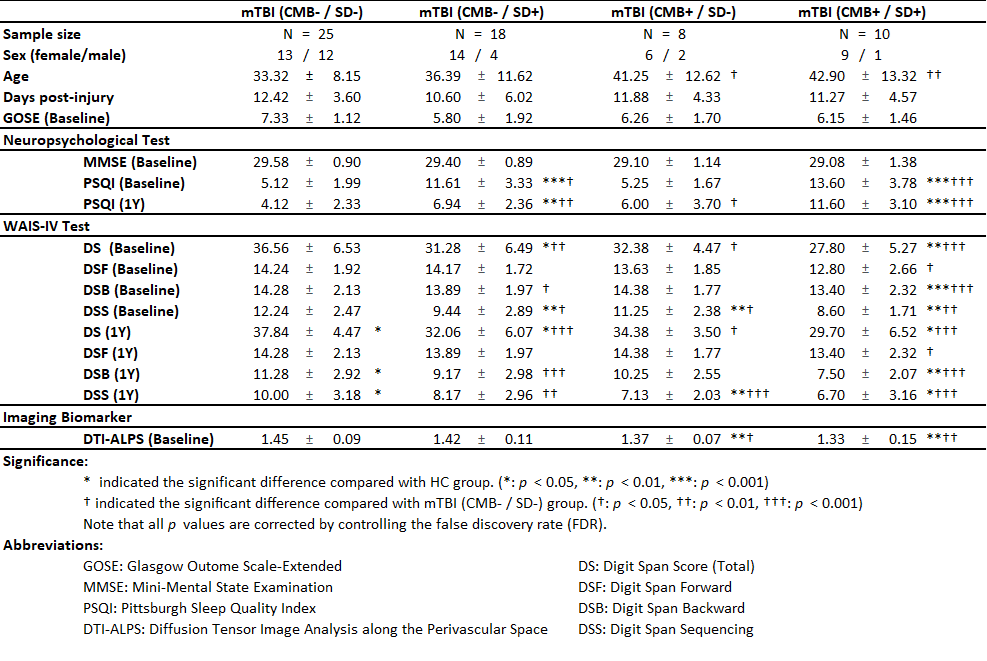
This study involved 61 mTBI patients and 61 demographically-matched healthy controls (Figure 1). Participants underwent MRI scans, including susceptibility-weighted imaging (SWI) and diffusion tensor imaging (DTI). The mTBI patients were categorized into two groups (Table 1): one with CMBs (N=18) and one without CMBs (N=43) based on susceptibility-weighted MRI [7, 8]. We employed the diffusion tensor imaging – along with perivascular space (DTI-ALPS) technique [9] to assess glymphatic function (Figure 2). Neuropsychological assessments, such as the Pittsburgh Sleep Quality Index (PSQI) and digit span (DS) working memory tests, were administered at the initial visit and a 1-year follow-up. The patients were further categorized into those with sleep disorders (SD; N=44) and those without SD (N=17) using a predefined threshold of PSQI>8 [10, 11] (Table 2). Finally, machine learning models were used to predict 1-year cognitive outcomes based on these baseline factors.Result
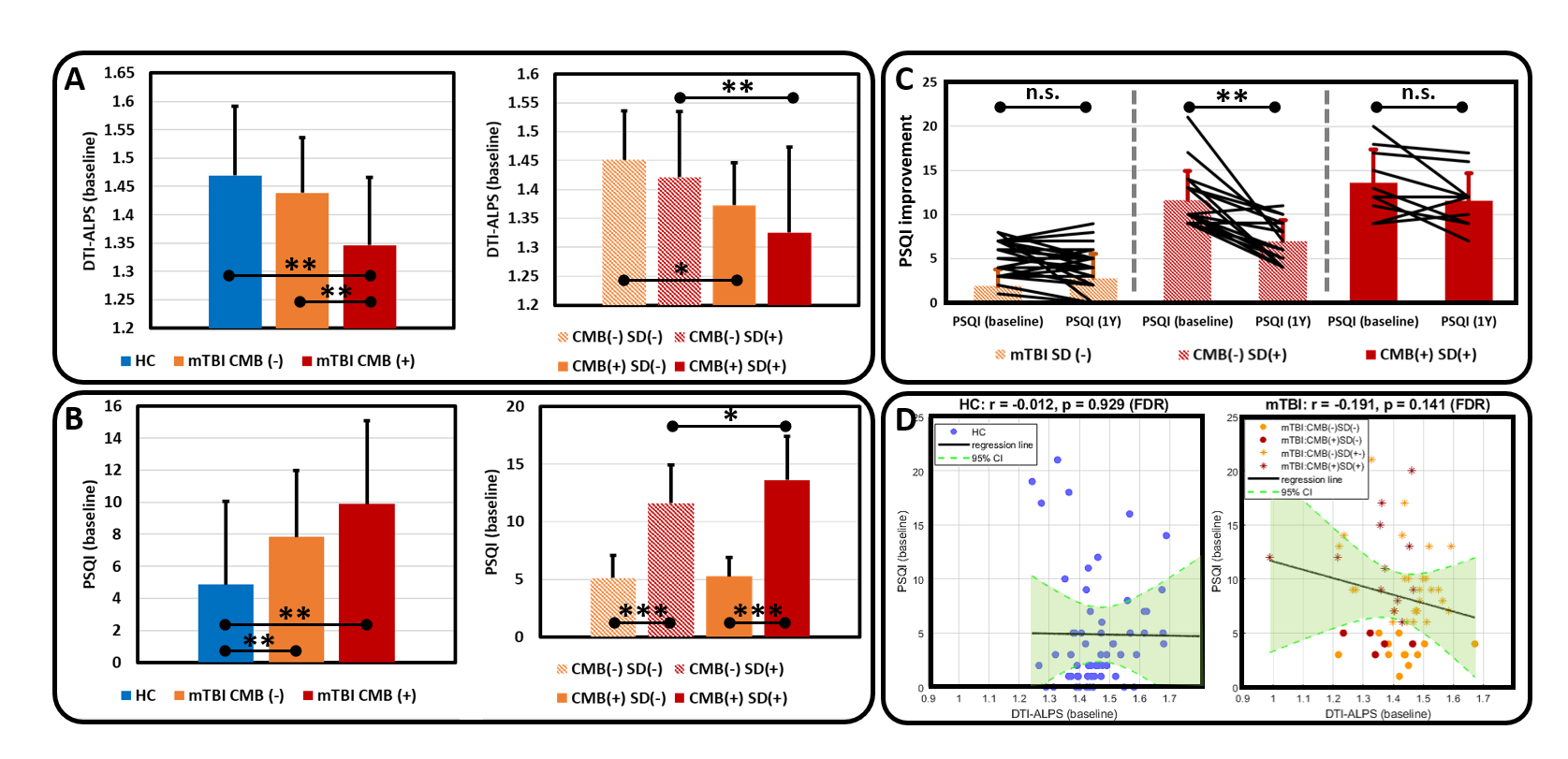
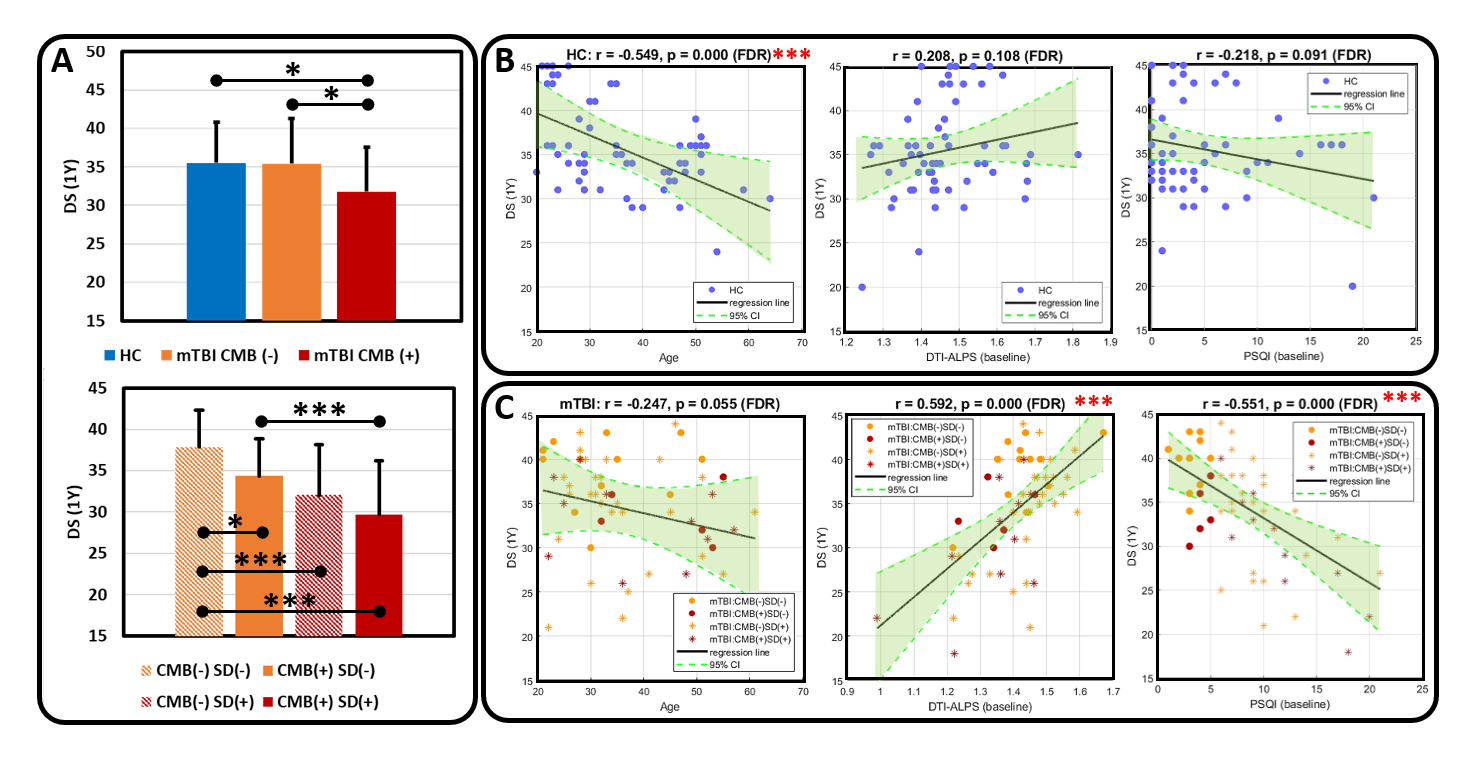
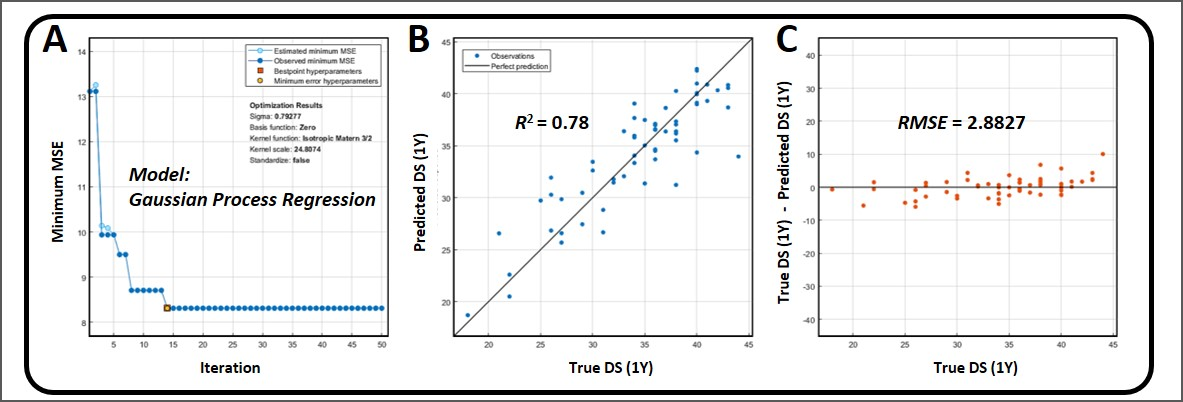
Traumatic CMBs were identified in 18 mTBI patients. Patients with CMBs exhibited lower baseline glymphatic function (DTI-ALPS index) and poorer sleep quality (PSQI scores) (Figure 3). The GLM analyses showed a significant relationship between the glymphatic diffusivity (DTI-ALPS index) and the number of CMBs (t = -4.128, p < 0.001), and no significant relationship with baseline PSQI score [t = -0.684, p = 0.497]), by controlling for confounding factors (i.e., age [t = -0.674, p = 0.503], sex [t = 0.39, p = 0.700], education level [t = 1.430, p = 0.159], GOSE [t = -1.756, p = 0.085], and duration from injury to MRI [t = 1.011, p = 0.316]). The models explained 41.98% of the variance in DTI-ALPS index assessed at baseline (R2 = 0.420). Overall, the results suggested that concussion-induced CMBs may be a key factor for postconcussive glymphatic dysfunction. Furthermore, CMB+ patients displayed significantly lower DS scores at both baseline and the 1-year follow-up (Figure 4). The correlation between glymphatic function, sleep quality, and working memory was significant, with glymphatic dysfunction and poor sleep quality contributing to cognitive decline (Figure 4). Furthermore, the GLM analyses demonstrated a significant relationship between the 1-year DS score and the baseline DS measure (t = 4.368, p < 0.001), and two baseline predictor variables (i.e., DTI-ALPS index [t = 6.105, p = 0.014] and PSQI score [t = -2.546, p = 0.014]), and no significant relationship with number of CMBs [t = 0.926, p = 0.359]), by controlling for confounding factors (i.e., age [t = 0.148, p = 0.883], sex [t = -1.092, p = 0.280], education level [t = 0.665, p = 0.509], GOSE [t = 0.357, p = 0.722], and duration from injury to MRI [t = 1.863, p = 0.068]). The models explained 68.59% of the variance in DS score assessed at 1-year follow-up (R2 = 0.686). The machine learning model effectively predicted 1-year cognitive outcomes (Figure 5), with an R2 value of 0.78 and a root-mean-squared error of 2.8827, and with baseline glymphatic function, sleep quality, and sex as key predictors.Discussion
Cognitive impairment following mTBI appears to be associated with CMBs, glymphatic dysfunction, and sleep quality. Traumatic CMBs are linked to diffuse axonal injury (DAI), which is a known contributor to cognitive deficits [12, 13]. The glymphatic dysfunction, mediated by the aquaporin-4 (AQP4) water channel, may play a pivotal role in this relationship. Traumatic CMBs could reflect damage to perivascular-space structures, resulting in poor glymphatic function [14]. Notably, sleep quality, a critical factor in glymphatic function [14], appears to support the restoration of cognitive function, even when glymphatic clearance is compromised.Conclusion
This study underscores the intricate interplay between traumatic CMBs, glymphatic system function, and sleep quality in mTBI patients. Understanding these relationships provides valuable insights into the pathophysiology of persistent cognitive impairment following mTBI. The machine learning model, utilizing baseline factors, presents a promising approach for individualized predictions of long-term cognitive function, ultimately enhancing the care and prognosis of mTBI patients.Acknowledgements
This work was partially supported by the Ministry of Science and Technology, Taiwan (MOST108-2321-B-038-008, MOST110-2314-B-038-086-MY3), and Taipei Medical University, Taiwan (TMU109-AE1-B18).References
1. Rabinowitz AR, Levin HS. Cognitive sequelae of traumatic brain injury. Psychiatric Clinics. 2014;37(1):1-11.
2. McInnes K, Friesen CL, MacKenzie DE, Westwood DA, Boe SG. Mild Traumatic Brain Injury (mTBI) and chronic cognitive impairment: A scoping review. PloS one. 2017;12(4):e0174847.
3. Chen Y-C, Chen Y-L, Kuo D-P, et al. Personalized prediction of postconcussive working memory decline: a feasibility study. Journal of personalized medicine. 2022;12(2):196.
4. Ouellet M-C, Savard J, Morin CM. Book review: Insomnia following traumatic brain injury: A review. Neurorehabilitation and Neural Repair. 2004;18(4):187-198.
5. Ouellet M-C, Morin CM. Subjective and objective measures of insomnia in the context of traumatic brain injury: a preliminary study. Sleep medicine. 2006;7(6):486-497.
6. Ayalon L, Borodkin K, Dishon L, Kanety H, Dagan Y. Circadian rhythm sleep disorders following mild traumatic brain injury. Neurology. 2007;68(14):1136-1140.
7. Yates PA, Villemagne VL, Ellis KA, Desmond PM, Masters CL, Rowe CC. Cerebral microbleeds: a review of clinical, genetic, and neuroimaging associations. Frontiers in neurology. 2014;4:205.
8. Nandigam R, Viswanathan A, Delgado P, et al. MR imaging detection of cerebral microbleeds: effect of susceptibility-weighted imaging, section thickness, and field strength. American Journal of Neuroradiology. 2009;30(2):338-343.
9. Taoka T, Masutani Y, Kawai H, et al. Evaluation of glymphatic system activity with the diffusion MR technique: diffusion tensor image analysis along the perivascular space (DTI-ALPS) in Alzheimer’s disease cases. Japanese journal of radiology. 2017;35:172-178.
10. Fichtenberg NL, Putnam SH, Mann NR, Zafonte RD, Millard AEJAjopm, rehabilitation. Insomnia screening in postacute traumatic brain injury: utility and validity of the Pittsburgh Sleep Quality Index. 2001;80(5):339-345.
11. Dj B, Reynolds C, Monk T, Berman S, Kupfer DJPR. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. 1989;28(2):193-213.
12. Sugiyama K, Kondo T, Oouchida Y, et al. Clinical utility of diffusion tensor imaging for evaluating patients with diffuse axonal injury and cognitive disorders in the chronic stage. Journal of neurotrauma. 2009;26(11):1879-1890.
13. Scheid R, Walther K, Guthke T, Preul C, von Cramon DY. Cognitive sequelae of diffuse axonal injury. Archives of neurology. 2006;63(3):418-424.
14. Hablitz LM, Nedergaard M. The glymphatic system. Current Biology. 2021;31(20):R1371-R1375.
Figures