4804
Aberrant Functional Connectivity Patterns in the Anterior Cingulate Cortex Subregions of Irritable Bowel Syndrome with Depressive Symptoms1The Affiliated Hospital of Hangzhou Normal University, Hangzhou, China, 2The Hangzhou Normal University, Hangzhou, China, 3MR Research, GE Healthcare, Shanghai, China
Synopsis
Keywords: Psychiatric Disorders, fMRI (resting state), Irritable bowel syndrome, Anterior cingulate cortex
Motivation: Atrophy and hyperactivity of the anterior cingulate gyrus (ACC) are key drivers of irritable bowel syndrome (IBS) and its psychiatric comorbidity.
Goal(s): Resting-state fMRI was performed to observe the functional connectivity (FC) patterns of ACC subregions in IBS with depressive symptoms patients to explore the potential neural mechanism of IBS and its comorbidity depression.
Approach: Seed-based whole-brain FC analysis was performed and distinct subregions of ACC showed different whole-brain connectivity patterns in IBS patients.
Results: The aberrant FC within the emotional arousal network, salience network and executive network may be characteristic neurobiological markers of IBS with comorbidity depression.
Impact: The aberrant FC within the emotional arousal network may be a characteristic neurobiological marker of IBS with comorbidity depression. In addition, the abnormal FC between the salience network and the executive network may be the underlying neural mechanism of IBS.
Introduction
Irritable bowel syndrome (IBS) is a common brain-gut interaction disorder that has a high comorbidity rate with depression1,2. However, the neurobiological basis underlying IBS with depressive symptoms (DEP-IBS) and how it mediates the relationship between IBS and depressive symptoms remains unclear. Atrophy and hyperactivity of the anterior cingulate gyrus (ACC) are key drivers of IBS and its psychiatric comorbidities3, and subregions of ACC play different roles in cognitive processing, emotion and pain regulation4,5. Resting-state fMRI (RS-fMRI) was performed in this study to observe the functional connectivity (FC) patterns of ACC subregions in DEP-IBS patients to explore the potential neural mechanism of IBS and its comorbidity depression.Methods
Forty-nine IBS patients who met Rome III criteria were divided into the DEP-IBS group (n = 28) and the IBS without depressive symptoms (nDEP-IBS) group (n = 21) according to the Hamilton Depression Scale score (HAMD). Thirty-six matched healthy controls (HC) were recruited. All subjects underwent a 3.0 T RS-fMRI scan (GE Discovery MR-750, Waukesha, WI). After data preprocessing, seed-based whole-brain FC analysis was performed using the pregenual anterior cingulate gyrus (pgACC) and anterior middle cingulate gyrus (aMCC, also known as dorsal ACC) as region of interest, respectively. One-way analysis of covariance (ANCOVA) and post hoc t test were applied to compare the differences of FC values among the three groups, and partial correlation and mediation analysis were performed between abnormal FC values and clinical scale scores. The receiver operating characteristic (ROC) curve was further drawn to classify the aberrant FC values of the IBS and its psychiatric comorbidity.Results
Compared with the nDEP-IBS group, the DEP-IBS group showed increased pgACC-related FC in the left medial prefrontal cortex (mPFC) and aMCC-related FC in the right middle frontal gyrus, angular gyrus and cerebellum, as well as decreased aMCC-related FC in the right precentral gyrus, superior parietal lobe (SPL) and precuneus. Compared with the HC group, both patient groups showed increased FC between aMCC and the left dorsolateral prefrontal cortex (dlPFC), and decreased FC between pgACC and left SPL. The ROC curve demonstrated that the FC between aMCC and DLPFC effectively distinguished IBS patients from HC (AUC=0.755). The partial correlation analysis revealed that some abnormal FC values were significantly correlated with gastrointestinal and/or depressive symptoms in all patients. Among them, the FC between pgACC and left mPFC served as a partial mediator between gastrointestinal and depressive symptoms, and this FC value could also effectively distinguish DEP-IBS and nDEP-IBS patients (AUC=0.808).Discussion
DEP-IBS patients exhibited hyperconnectivity within the emotional arouse network as well as abnormal FC between aMCC and regions related to the attention network, default mode network and sensorimotor network. Furthermore, IBS patients are associated with hyperconnectivity between the salience network and the executive control network as well as hypoconnectivity between the emotional arousal and the attention network.Conclusion
Distinct subregions of ACC show different whole-brain connectivity patterns in IBS patients with or without depressive symptoms. In particular, the aberrant FC within the emotional arousal network may be a characteristic neurobiological marker of IBS with comorbidity depression. In addition, the abnormal FC between the salience network and the executive network may be the underlying neural mechanism of IBS.Acknowledgements
No acknowledgement found.References
1. Black CJ, Ford AC. Global burden of irritable bowel syndrome: trends, predictions and risk factors. Nat Rev Gastroenterol Hepatol. 2020 Aug;17(8):473–86.
2. Hadjivasilis A. New insights into irritable bowel syndrome: from pathophysiology to treatment. aog [Internet]. 2019 [cited 2023 Sep 1]; Available from: http://www.annalsgastro.gr/files/journals/1/earlyview/2019/ev-10-2019-09-AG4742-0428.pdf
3. Matisz CE, Gruber AJ. Neuroinflammatory remodeling of the anterior cingulate cortex as a key driver of mood disorders in gastrointestinal disease and disorders. Neuroscience & Biobehavioral Reviews. 2022 Feb;133:104497
4. Shackman AJ, Salomons TV, Slagter HA, Fox AS, Winter JJ, Davidson RJ. The integration of negative affect, pain and cognitive control in the cingulate cortex. Nat Rev Neurosci. 2011 Mar;12(3):154–67.
5. Stevens FL. Anterior Cingulate Cortex: Unique Role in Cognition and Emotion. J Neuropsychiatry Clin Neurosci. 2011.
Figures
Figure 1. ANCOVA (A) and post hoc t-test (B-D) results of whole-brain functional connectivity analysis using aMCC as seed region (GRF-corrected, cluster-level: P <0.005, voxel-level: P <0.05). IBS, irritable bowel syndrome; DEP-IBS, IBS patients with depressive symptoms; nDEP-IBS, IBS patients without depressive symptoms; HC, healthy controls; aMCC, anterior middle cingulate cortex; dlPFC, dorsal lateral prefrontal cortex; SPG, superior parietal gyrus; MFG, middle frontal gyrus; IFG, inferior frontal gyrus.
Figure 2. ANCOVA (A) and post hoc t-test (B-D) results of whole-brain functional connectivity analysis using pgACC as seed region (GRF-corrected, cluster-level: P <0.005, voxel-level: P <0.05). IBS, irritable bowel syndrome; DEP-IBS, IBS patients with depressive symptoms; nDEP-IBS, IBS patients without depressive symptoms; HC, healthy controls; pgACC, pregenual anterior cingulate cortex; mPFC, medial prefrontal cortex; SPG, superior parietal gyrus; IFG, inferior frontal gyrus; STG, superior temporal gyrus; pINS, posterior insula.
Figure 3. (A). The results of correlation and mediated analysis between pgACC-mPFC FC values and clinical symptoms in IBS patients. (B-C). Receiver-operating-characteristic (ROC) curve and the area under the ROC curve (AUC) that pgACC-mPFC FC values could be used to differentiate between DEP-IBS and the nDEP-IBS patients as well as aMCC-dlPFC FC values could distinguish IBS patients from HC. GSRS: gastrointestinal symptoms rating scale; HAMD: Hamilton Depression Rating Scale
Table 1. Demographic and Clinical Characteristics of Participants.
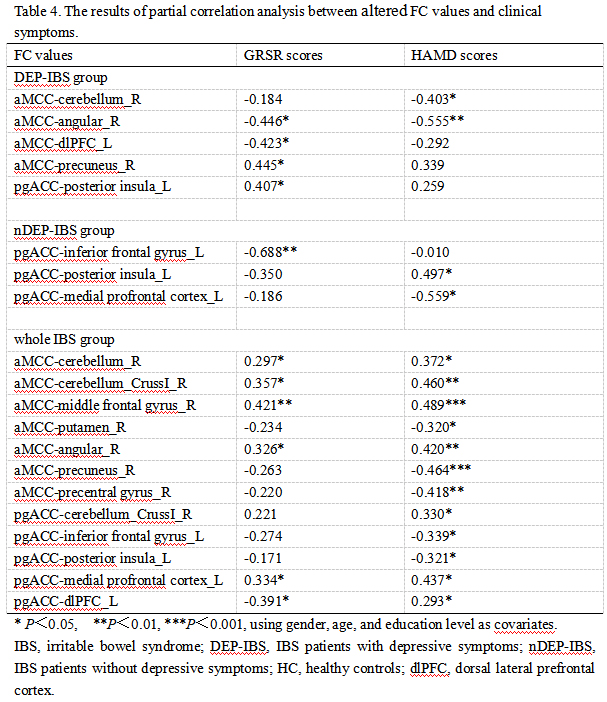
Table 4. The results of partial correlation analysis between altered FC values and clinical symptoms, using gender, age, and education level as covariates.