4802
Predictive Potential of IVIM for Vessels Encapsulate Tumor Clusters and Recurrence-free Survival in Hepatocellular Carcinoma1Department of Radiology, Zhujiang Hospital of Southern Medical University, Guangzhou, China, 2Philips Healthcare, Guangzhou, China
Synopsis
Keywords: Liver, Diffusion/other diffusion imaging techniques, Vessels Encapsulate Tumor Clusters (VETC),IVIM,HCC
Motivation: To explore a more accurate non-invasive method for predicting VETC pattern in HCC.
Goal(s): To estimate the potential of preoperative IVIM in predicting of VETC pattern in HCC.
Approach: Investigating the correlation between IVIM-derived parameters and the VETC pattern, and constructing a predictive model.
Results: Our results showed that VETC HCC exhibited a declining f value trend and outperformed conventional imaging-clinical models when an integrated model was established, incorporating intratumoral necrosis and high-level AFP. Furthermore, this model is capable of identifying individuals at high risk of postoperative recurrence.
Impact: To our knowledge, this study marks the first time diffusion sequences have been used to predict VETC in HCC, which offers a fresh perspective and paves the way for more accurate VETC direction in the future.
Introduction
Hepatocellular carcinoma (HCC) with vessels encapsulating tumor clusters (VETC) pattern is now recognized to be associated with a higher risk of recurrence and metastasis[1]. Previous case-control studies have found that VETC HCC demonstrates a more favorable response to treatments such as sorafenib, resection after recurrence, and adjuvant transcatheter arterial chemoembolization(TACE), leading to improved prognosis[2-4]. Hence, preoperative identification of VETC holds significant importance in tailoring individualized therapy for hepatocellular carcinoma. However, obtaining pathological tissue through liver biopsy is limited in reflecting the VETC status of the whole tumor, and the operation carries certain risks. Therefore, we are committed to finding non-invasive methods to predict VETC before surgery.The VETC pattern is characterized by a continuous lining of sinusoid-like vessels that isolate and encapsulate individual tumor clusters, forming a cobweb-like pattern. one study has indicated that higher intra-tumoral microvessel density is significantly associated with the VETC pattern[5], suggesting that its unique vascular structure has an impact on the tumor’s perfusion microenvironment. Intravoxel Incoherent Motion (IVIM) can be used to quantify tissue perfusion. However, there have been no previous studies demonstrating the potential of IVIM in predicting the VETC pattern. Consequently, our study aims to evaluate the potential of preoperative IVIM in predicting VETC in HCC and further explore its predictive value for recurrence in HCC patients undergoing surgical resection.
Methods
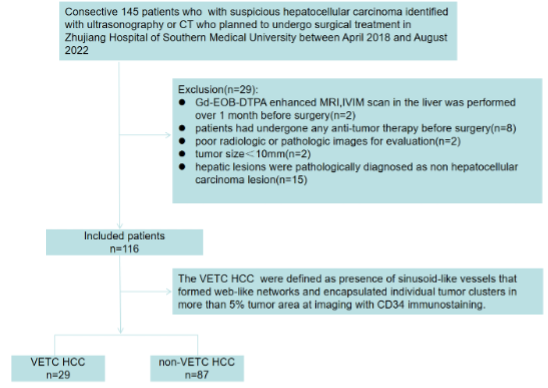
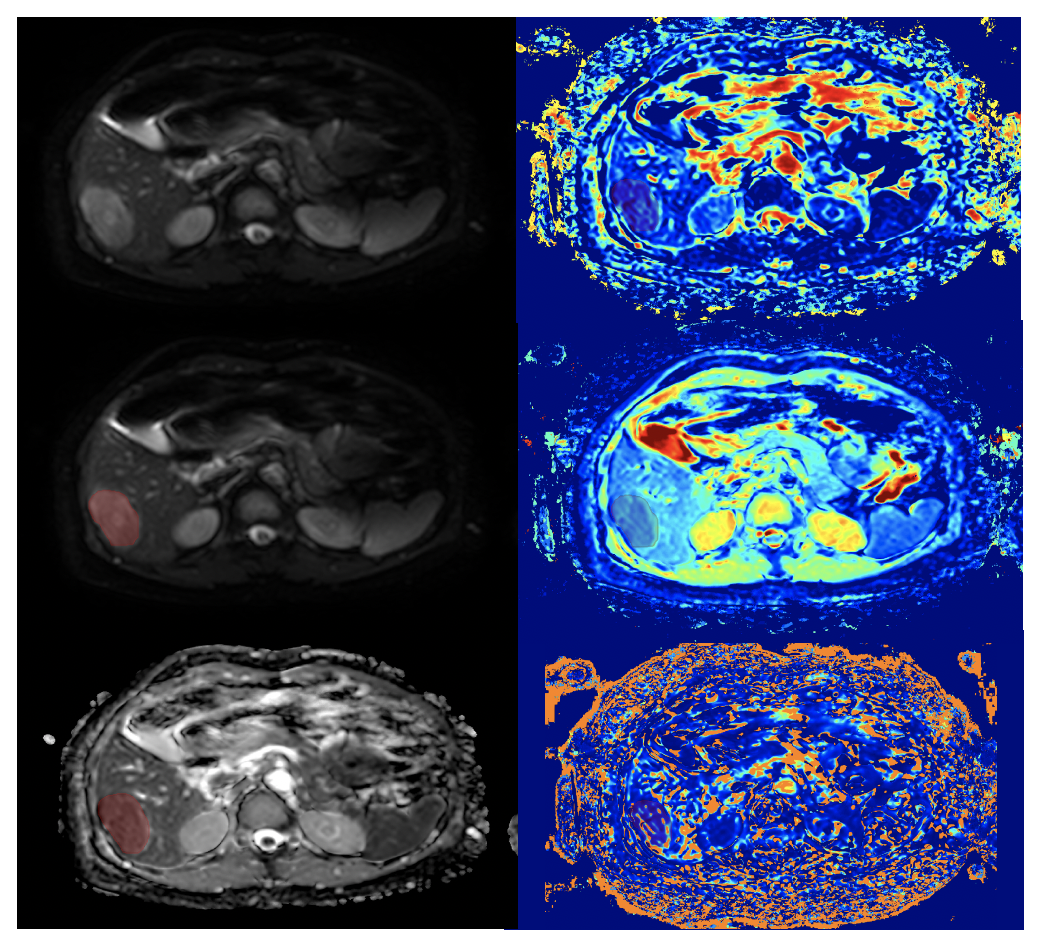
The study included patients who underwent surgical resection for HCC and underwent preoperative MRI scans with IVIM between April 2018 and August 2022 at Zhujiang Hospital of Southern Medical University in Guangzhou, China (Fig 1). Two radiologists independently reviewed the radiologic features of the HCC tumors. They measured the following IVIM parameters: apparent diffusion coefficient (ADC), true diffusion coefficient (D), pseudodiffusion coefficient (D*), and pseudodiffusion component fraction (f). Predictors associated with the VETC pattern were determined using logistic regression analyses (Fig 2). To evaluate the predictive performance, receiver operating characteristics (ROC) curve analyses were conducted, and the Delong test was performed to compare the prediction models. Recurrence-free survival (RFS) was evaluated using Kaplan-Meier analysis and the Log-rank test.Results
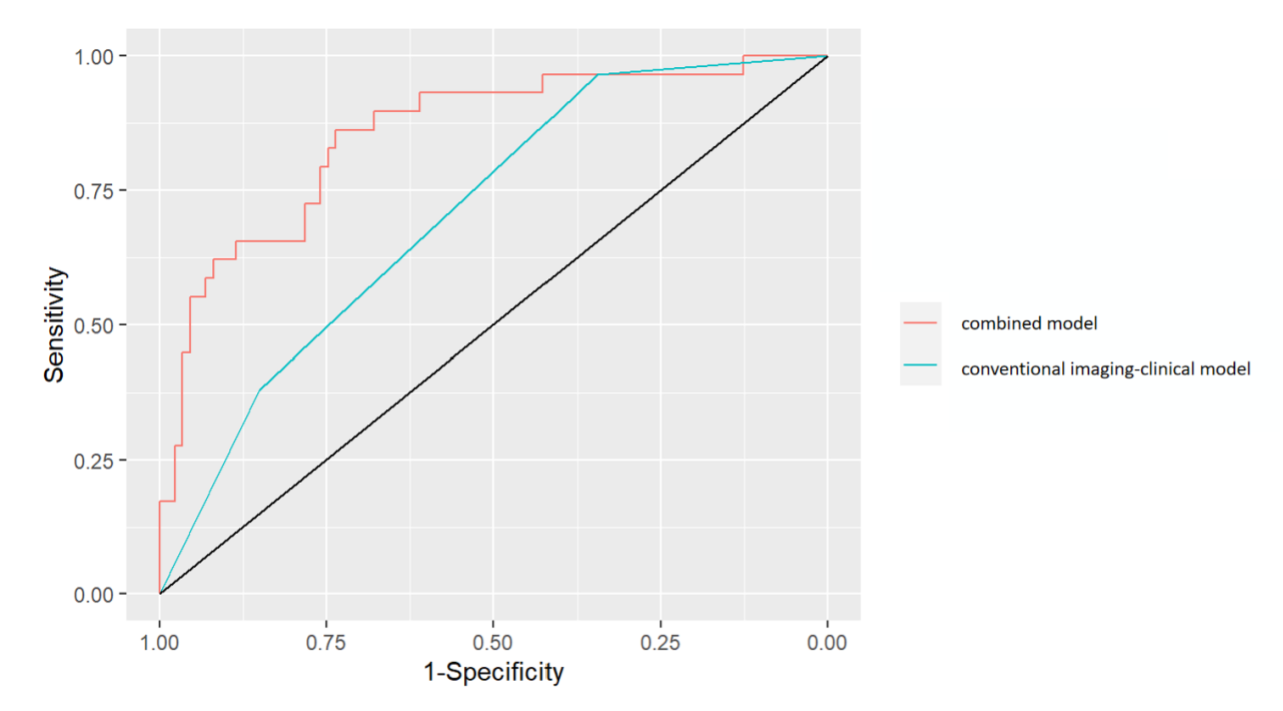
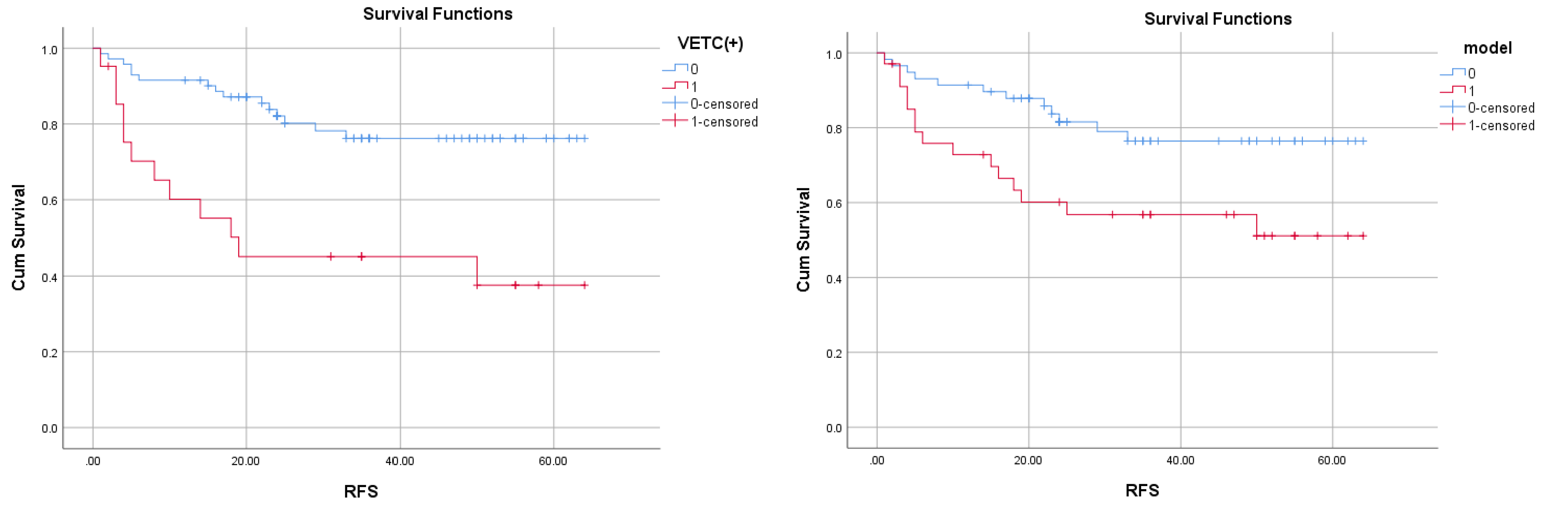
The consecutive cohort included 116 patients with HCC with a median age of 54 years, of which 94 were men. Among these, 29 out of 116 HCCs (25%) were classified as VETC HCC.The f value (OR, 0.79; 95% CI: 0.70, 0.90; P<0.001), high serum a-fetoprotein (AFP) level (>400 ng/mL)(OR, 2.96; 95% CI: 1.04, 8.45; P=0.042), and intratumor necrosis (OR, 6.02; 95% CI: 1.43, 25.41; P=0.015) were identified as independent predictors for the VETC pattern. These features were used to establish a prediction model, and the area under the ROC curve for this model was 0.85 (95% CI: 0.77~0.94). Additionally, the Delong test showed that adding the f value to the model significantly improved its predictive performance compared to the conventional imaging-clinical model(p<0.001) (Fig 3). The Log-rank test demonstrated that patients with VETC HCC had a higher risk of recurrence compared to those with non-VETC HCC (p<0.001). Moreover, patients with the model classified as VETC HCC also had a higher risk of recurrence than those with the model classified as non-VETC HCC (p=0.014) (Fig 4).
Discussion
The study’s findings revealed that VETC HCC tends to exhibit lower f values on IVIM compared to non-VETC HCC. The ROI chosen in this study focused on tumor parenchyma while avoiding the tumor necrotic area. This choice aligns with the pathological characteristics of VETC HCC, where the parenchymal region is associated with vigorous tumor growth, higher cell density, and increased oxygen demand. These factors can influence the perfusion microenvironment of VETC HCC. VETC HCC is known to metastasize primarily through tumor clusters enclosed by endothelial cells[1], which can obstruct small blood vessels and impact tumor perfusion.Prior studies have indicated that poor histologic differentiation HCC has a lower f value, and VETC HCC is more likely to be poorly differentiated[6-8]. This may explain the lower f value observed in VETC HCC. Additionally, our results suggest that intratumoral necrosis is independently correlated with VETC patterns, consistent with previous findings[6]. Furthermore, the prediction model for VETC HCC, when based on the optimal cut-off value, was linked to a higher risk of postoperative recurrence. This implies that the prediction model has the potential to identify individuals at a higher risk of postoperative recurrence, which can be valuable for clinical decision-making.
Conclusion
In conclusion, our findings indicate that IVIM can serve as a promising noninvasive biomarker for predicting VETC HCC and can provide helpful prognostic information to assist in VETC HCC diagnosis and clinical treatment strategy.Acknowledgements
No acknowledgements found.References
[1] Fang, J. H., Zhou, H. C., Zhang, C., Shang, L. R., et al. A novel vascular pattern promotes metastasis of hepatocellular carcinoma in an epithelial-mesenchymal transition-independent manner. Hepatology. 2015, 62(2): 452-465.
[2] Fang, J. H., Xu, L., Shang, L. R., Pan, C. Z., et al. Vessels That Encapsulate Tumor Clusters (VETC) Pattern Is a Predictor of Sorafenib Benefit in Patients with Hepatocellular Carcinoma. Hepatology. 2019, 70(3): 824-839.
[3] Chen, Z. Y., Guo, Z. X., Lu, L. H., Mei, J., et al. The predictive value of vessels encapsulating tumor clusters in treatment optimization for recurrent early-stage hepatocellular carcinoma. Cancer Med. 2021, 10(16): 5466-5474.
[4] Wang, J. H., Li, X. S., Tang, H. S., Fang, R. Y., et al. Vessels that encapsulate tumor clusters (VETC) pattern predicts the efficacy of adjuvant TACE in hepatocellular carcinoma. J Cancer Res Clin Oncol. 2023, 149(8): 4163-4172.
[5] Huang, C. W., Lin, S. E., Huang, S. F., Yu, M. C., et al. The Vessels That Encapsulate Tumor Clusters (VETC) Pattern Is a Poor Prognosis Factor in Patients with Hepatocellular Carcinoma: An Analysis of Microvessel Density. Cancers (Basel). 2022, 14(21).
[6] Feng, Z., Li, H., Zhao, H., Jiang, Y., et al. Preoperative CT for Characterization of Aggressive Macrotrabecular-Massive Subtype and Vessels That Encapsulate Tumor Clusters Pattern in Hepatocellular Carcinoma. Radiology. 2021, 300(1): 219-229.
[7] Wu, B., Jia, F., Li, X., Li, L., et al. Comparative Study of Amide Proton Transfer Imaging and Intravoxel Incoherent Motion Imaging for Predicting Histologic Grade of Hepatocellular Carcinoma. Front Oncol. 2020, 10: 562049.
[8] Zhang, Y., Kuang, S., Shan, Q., Rong, D., et al. Can IVIM help predict HCC recurrence after hepatectomy? Eur Radiol. 2019, 29(11): 5791-5803.
Figures