4800
Assessment of renal function with arterial spin labeling and intravoxel incoherent motion in type 2 diabetic patients1Shanxi Medical University, Taiyuan, China, 2GE Healthcare, Beijing, China, 3Shanxi Provincial People's Hospital, Taiyuan, China
Synopsis
Keywords: Kidney, Arterial spin labelling, type 2 diabetes mellitus,renal function
Motivation: Kidney injury could be occurred in the early stages of DM.
Goal(s): We aimed to evaluate the diagnostic values of ASL and IVIM for distinguishing early kidney dysfunction in T2DM.
Approach: All subjects were performed ASL and IVIM scans.
Results: The results demonstrated that cortical RBF, f values and medullary D, f values were lower in the DM group with normal level of albumin-to-creatinine rate (ACR) than in control group, and f is the optimal index for differentiating the DM from DKD and control, indicating that ASL and IVIM could be used to evaluate kidney impairment of T2DM.
Impact: When early kidney injury in T2DM could be evaluated with ASL and IVIM,early clinical intervention can be implemented, significantly delaying or preventing the progression of DKD and greatly improving the prognosis for patients with DKD.
Purpose
This study aims to investigate the capabilities of arterial spin labeling (ASL) and intravoxel incoherent motion (IVIM) to diagnose early kidney injury in type 2 diabetes(T2DM).Introduction
Diabetic kidney disease (DKD) is one of the leading causes of death in patients with diabetes mellitus (DM) [1]. Abnormal changes have been described in the early stages of DM[2].However, existing methods, including CT and MR T1-weighted (T1W) and T2-weighted (T2W), are not sensitive enough to detect early functional disturbances and don’t provide effective quantitative indices[3]. And the renal biopsy may lead to complications such as perinephric hematoma and infection. ASL and IVIM are considered to have potential in the noninvasive assessment of kidney disease. However, most reports focused on the application of ASL and IVIM in renal allografts and fibrosis, and few of them investigated the application in DKD. Therefore, this study aimed to prospectively investigate the capability of ASL and IVIM in identifying early kidney function injury in T2DM.Method
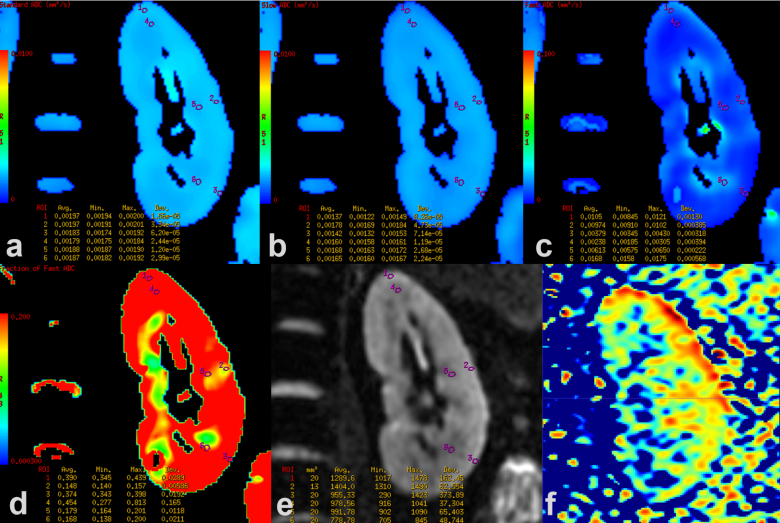
Forty-three T2DM patients(DM group: n=27,albumin-to-creatinine rate (ACR)<30mg/g, age 57.30±5.57 years; early DKD group: n=16,30≤ACR≤300mg/g, age 54.44±8.46 years) and 16 volunteers (age 54.00±4.66 years) were recruited. All participants were examined using ASL and IVIM with 3.0-T MRI (Discovery MR750,GE Healthcare, Milwaukee, WI, USA).ASL imaging parameters: TR=5450ms;TE=18.2ms; FOV=280×280mm2; matrix = 96×96; slice thickness=7.0mm; number of slices=10 slices; post-labeling delay=2000ms. IVIM imaging parameters: TR=2000ms;TE=76.8ms; FOV=380×380mm2; matrix = 160×128; slice thickness=4.0mm; number of slices=25 slices; b values(NEX) = 0(1), 30(1), 50(1), 80(1), 100(1), 150(1), 200(1), 300(1), 500(2), 800(5), 1000(6)s/mm2. The renal blood flow (RBF) from ASL imaging were analyzed with house-build software in Matlab R2018a,while the diffusion indices apparent diffusion coefficient (ADC), molecular diffusion (D), pseudo-diffusion (D*), perfusion fraction(f) from IVIM were calculated in the AW4.6 Workstation (GE Healthcare). Three ellipsoid regions of interest (ROIs) of 5-30 pixels were manually and separately placed in the upper, middle, and lower poles of the renal medulla, and three ellipsoid ROIs of 5-20 pixels were manually and separately placed in the upper, middle, and lower poles of the renal cortex for all the parametric maps. The average value of ROIs in medulla and cortex were used for the final analysis. Group comparison, correlation between each two indices (including ACR and imaging indices) and receiver operating characteristic (ROC) curves were performed using R Language (version 4.0.0).Results
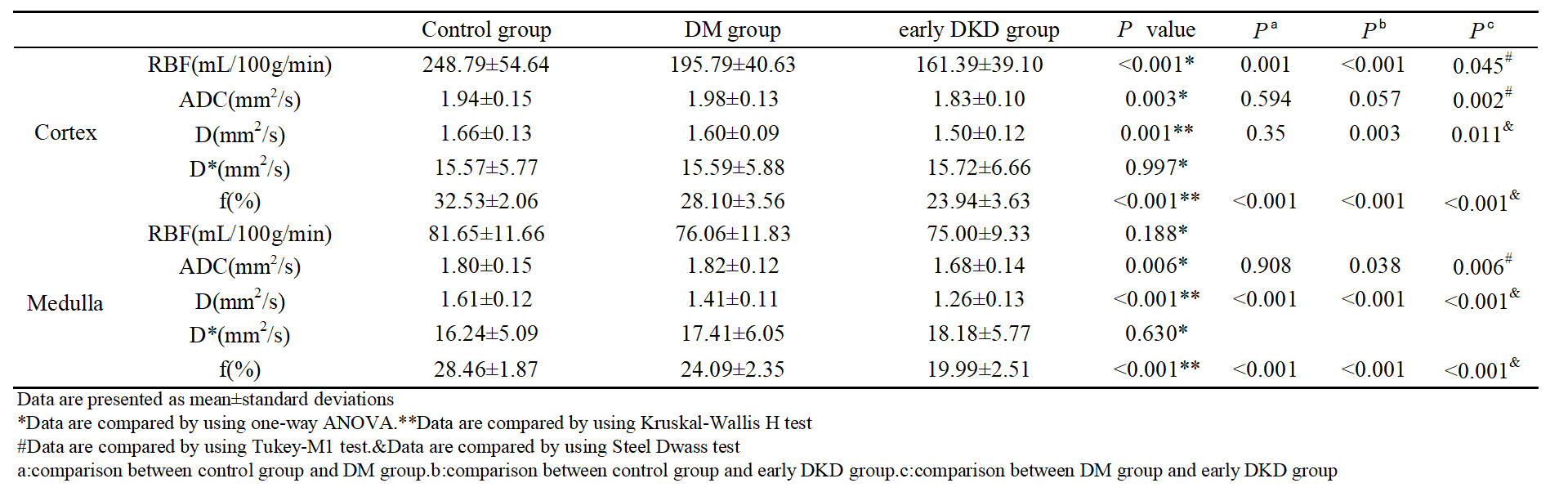
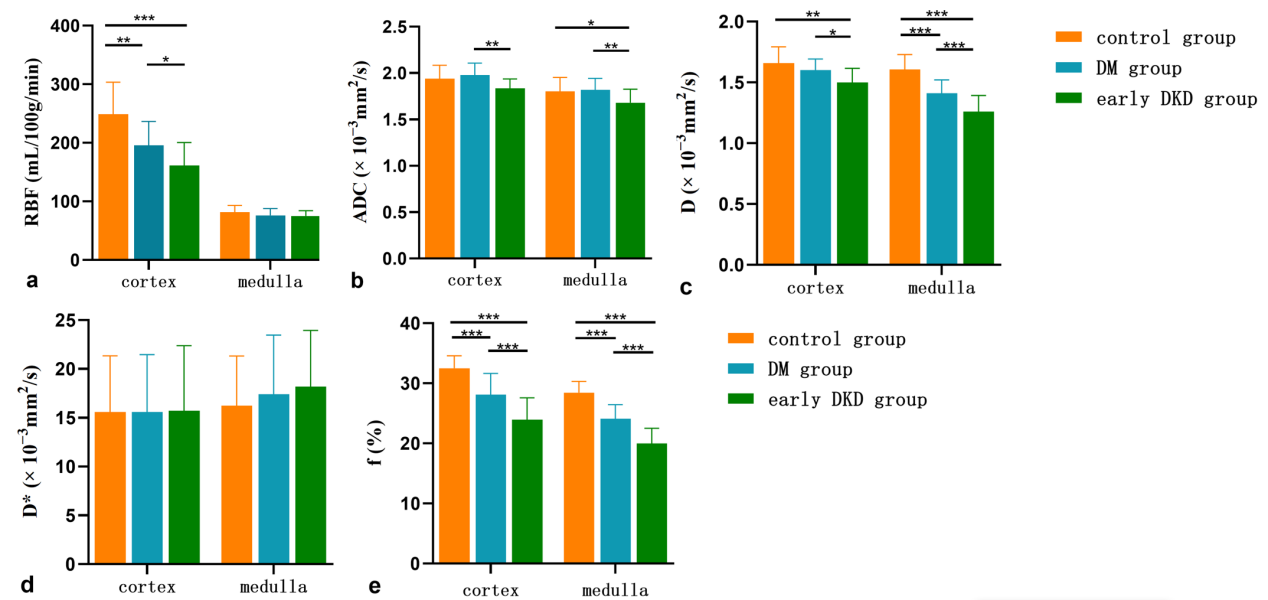
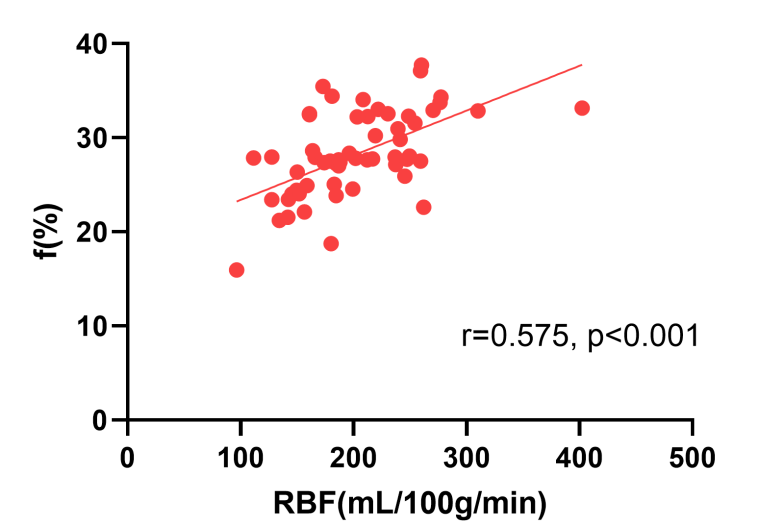
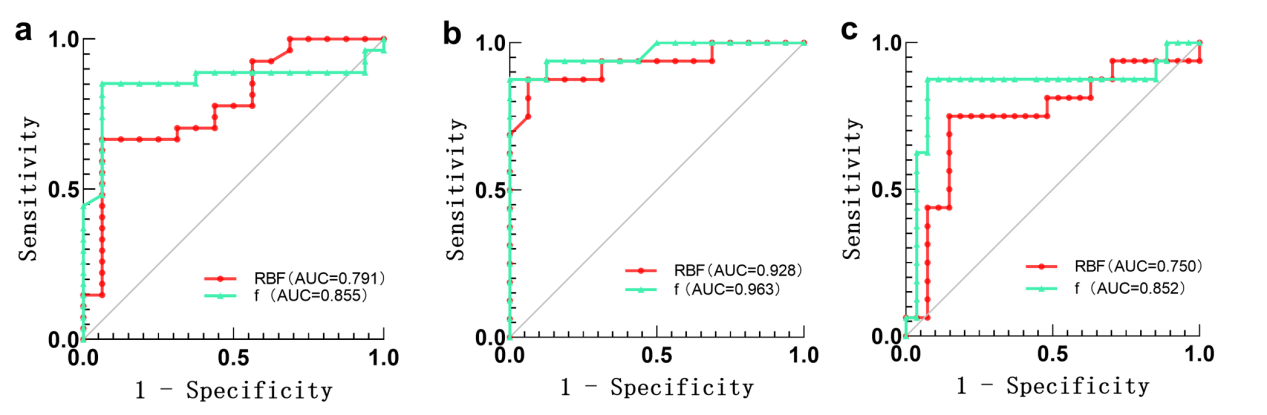
There were significant differences among the DM group, early DKD group, and control group for renal parenchyma ADC, D and f values and cortical RBF value (all p<0.05).The renal parenchyma f and cortical ADC were found negatively correlated with the ACR values (rs>-0.4,P<0.01), and the cortical RBF was positively correlated with the cortical f (rs=0.575,P<0.001). Optimal area under the curves (AUC) for differentiating DM group from control group (AUC = 0.944, sensitivity (sen.) = 96.30%, specificity (spe.) = 81.25%) and differentiating DM group from early DKD group (AUC = 0.910, sen.= 93.75%, spe. = 85.19%) were obtained with medullary f value.Discussion
It’s reported that part of DM patients have pathological changes in their kidneys, and some of them have poor prognosis [4,5]. Early detection and management of kidney injury in T2DM is important priority in avoiding the diabetic complications. Our findings demonstrated that cortical RBF, f values and medullary D, f values were significantly lower in the DM group than in control group, which indicates that decreased renal plasma flow and peritubular capillary flow [5], and diffusion of water molecules [6,7] may be limited in the DM stage. The results that renal parenchyma f value and cortical ADC value negatively correlated with the ACR value, suggest these two indices were able to be used to observe the changes during the progress of kidney injure in the diabetic population. Significant positive correlation between cortical RBF and cortical f value indicated similar perfusion change are shown by ASL and IVIM imaging for renal cortex. The medullary f as the best index for distinguishing the DM from control, and from DKD, which may be related to interstitial fibrosis.Conclusion
Abnormal micro-perfusion and diffusion can be sensitively detected by ASL and IVIM in early stage of T2DM development. The medullary f could act as the good indicator for DM and DKD diagnosis.Acknowledgements
The authors of this manuscript state that this work has not received any funding.References
[1] Zheng Y, Ley S H, Hu F B. Global aetiology and epidemiology of type 2 diabetes mellitus and its complications[J]. Nat Rev Endocrinol, 2018,14(2):88-98.
[2] Lin C H, Chang Y C, Chuang L M. Early detection of diabetic kidney disease: Present limitations and future perspectives[J]. World J Diabetes, 2016,7(14):290-301.
[3] Ku M C, Fernandez-Seara M A, Kober F, Niendorf T. Noninvasive Renal Perfusion Measurement Using Arterial Spin Labeling (ASL) MRI: Basic Concept[J]. Methods Mol Biol, 2021,2216:229-239.
[4] Klessens C Q, Woutman T D, Veraar K A, Zandbergen M, Valk E J, Rotmans J I, Wolterbeek R, Bruijn J A, Bajema I M. An autopsy study suggests that diabetic nephropathy is underdiagnosed[J]. Kidney Int, 2016,90(1):149-156.
[5] Furuichi K, Shimizu M, Okada H, Narita I, Wada T. Clinico-pathological features of kidney disease in diabetic cases[J]. Clin Exp Nephrol, 2018,22(5):1046-1051.
[6] Vora J P, Dolben J, Dean J D, Thomas D, Williams J D, Owens D R, Peters J R. Renal hemodynamics in newly presenting non-insulin dependent diabetes mellitus[J]. Kidney Int, 1992,41(4):829-835.
[7] Zhang H, Wang P, Shi D, Yao X, Li Y, Liu X, Sun Y, Ding J, Wang S, Wang G, Ren K. Capability of intravoxel incoherent motion and diffusion tensor imaging to detect early kidney injury in type 2 diabetes[J]. Eur Radiol, 2022,32(5):2988-2997.
[8] Feng Y Z, Chen X Q, Yu J, Liu X L, Cheng Z Y, Ren W W, Feng L, Cai X R. Intravoxel incoherent motion (IVIM) at 3.0 T: evaluation of early renal function changes in type 2 diabetic patients[J]. Abdom Radiol (NY), 2018,43(10):2764-2773.
Figures