4796
Evaluation of Spin-Echo EPI MR Elastography for Rapid Free-Breathing Quantification of Liver Stiffness1Radiological Sciences, University of California, Los Angeles, Los Angeles, CA, United States, 2Bioengineering, University of California, Los Angeles, Los Angeles, CA, United States, 3US MR R&D Collaborations, Siemens Medical Solutions USA, Inc., Salt Lake City, UT, United States, 4Physics and Biology in Medicine Interdepartmental Program, University of California, Los Angeles, Los Angeles, CA, United States, 5US MR R&D Collaborations, Siemens Medical Solutions USA, Inc., Austin, TX, United States, 6US MR R&D Collaborations, Siemens Medical Solutions USA, Inc., Houston, TX, United States, 7Medical Imaging, The University of Arizona, Tucson, AZ, United States, 8Biomedical Engineering, The University of Arizona, Tucson, AZ, United States, 9Interventional Radiology, University of California, Los Angeles, Los Angeles, CA, United States, 10Transplant Hepatology, University of California, Los Angeles, Los Angeles, CA, United States, 11Pediatrics, University of California, Los Angeles, Los Angeles, CA, United States
Synopsis
Keywords: Elastography, Pediatric, Liver Fibrosis
Motivation: Hepatic stiffness (HS), detected by MR elastography (MRE), is a biomarker for hepatic fibrosis. Liver MRE requires breath-holding (BH), which is challenging in children or people with liver disease. Spin-echo echo-planar-imaging (SE-EPI) MRE can quantify HS rapidly(~10 s), even with iron overload.
Goal(s): To evaluate free-breathing (FB) SE-EPI MRE without respiratory triggering or motion compensation in terms of agreement, repeatability, and measurable liver area [%] with respect to BH SE-EPI MRE.
Approach: BH and FB SE-EPI MRE were acquired in 23 children and 2 adults with liver biopsy.
Results: FB SE-EPI MRE provided fast, accurate, and repeatable HS with high measurable liver area.
Impact: The free-breathing (FB) MR elastography (MRE) of the liver based on spin-echo echo-planar-imaging (SE-EPI) produced accurate and repeatable hepatic stiffness with respect to standard breath-held SE-EPI MRE. FB SE-EPI MRE can be useful for populations who cannot hold their breath.
Introduction
MR elastography of the liver measures hepatic stiffness (HS) to assess fibrosis. Liver MRE typically uses either gradient echo (GRE) or spin-echo echo-planar imaging (SE-EPI) sequences (1–4) and requires breath-holding (BH) to mitigate motion artifacts. BH can be challenging in children, elderly, and people with liver disease. BH GRE-MRE requires 4 BHs for 4 slices at 10-20 seconds/slice. BH SE-EPI-MRE, in contrast, is a fast single BH acquisition (10 seconds). BH SE-EPI-MRE also performs better than BH GRE-MRE in the presence of iron overload in adults with chronic liver disease (5). Various studies tested the performance of GRE-MRE or SE-EPI-MRE under free-breathing (FB) conditions (6, 7). For Cartesian FB GRE-MRE, levels of agreement of HS compared to BH GRE-MRE varied dramatically between studies. Radial FB GRE-MRE tested in children reported close agreement and good repeatability, but smaller measurable liver area. Respiratory-triggered FB SE-EPI-MRE tested in adults showed close agreement with BH SE-EPI-MRE, but at the expense of smaller measurable liver area and variable scan time (8). Here, we evaluated FB SE-EPI-MRE (fixed scan time) without dedicated respiratory triggering or motion compensation in terms of agreement, repeatability, and measurable liver area [%] compared to BH SE-EPI-MRE.Methods
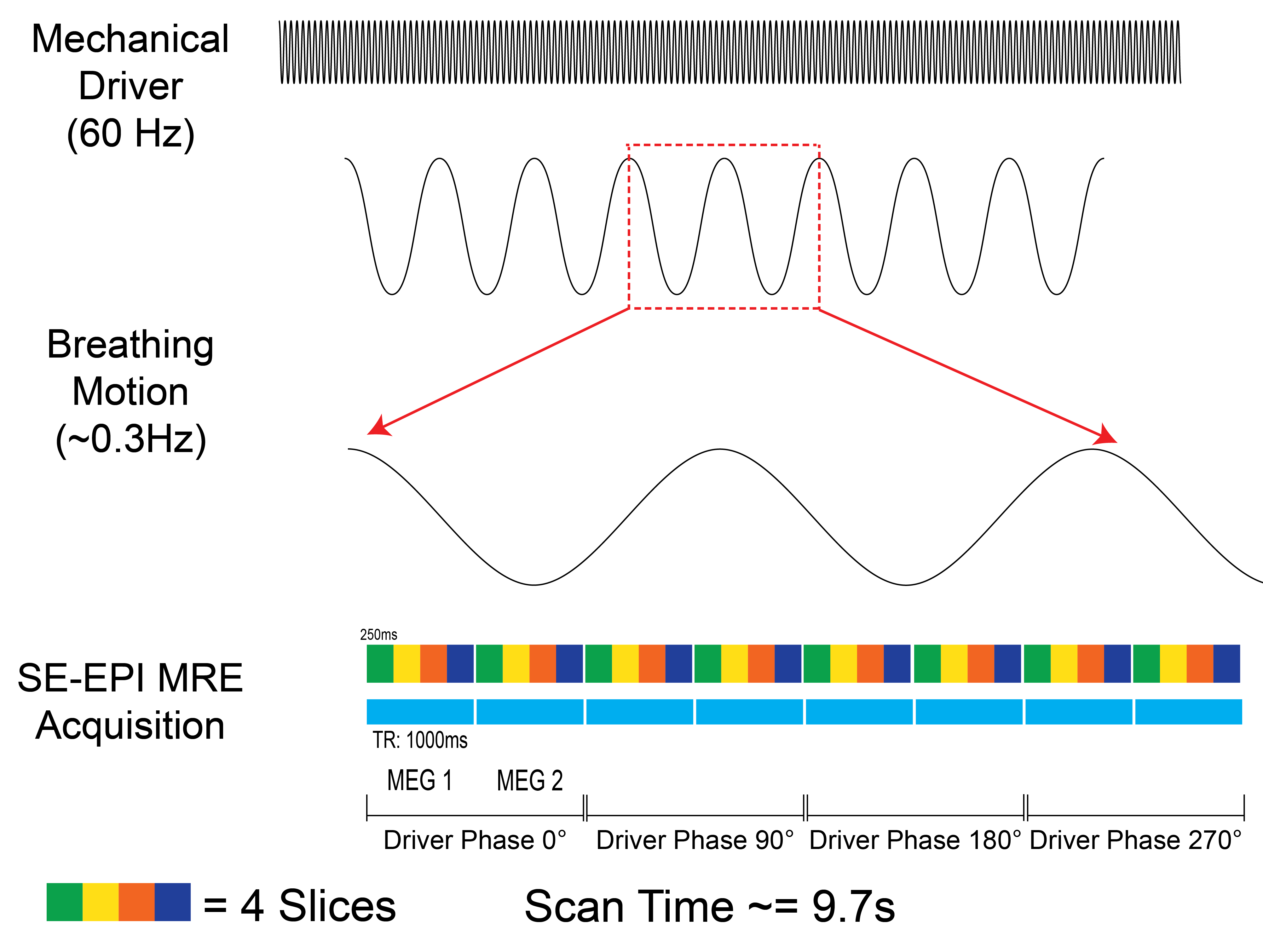
Study Cohort and MRE Experiments:This IRB-approved HIPAA-compliant study enrolled 11 healthy children (7F, 4M) and 12 overweight children (body mass index [BMI] >85th percentile; 4F, 8M), and 2 adults with suspected/confirmed fatty liver disease (2F, BMI1: 25.5 kg/m2, BMI2:25.9 kg/m2, ages 63 and 65 years). For the pediatric cohort, the [median, interquartile range (IQR)] age was [13.3, 5.4] years and BMI was [84.6, 23.3] percentile. BH and FB SE-EPI-MRE were acquired at 3T (MAGNETOM PrismaFit, Siemens Healthcare GmbH, Erlangen, Germany). For the pediatric scans, a prototype flexible MRE passive driver (Mayo Clinic, Rochester, MN) was used to improve comfort. The imaging parameters for BH and FB SE-EPI-MRE were matched (TR: 1000 ms, TE: 47 ms, resolution: 1.4mmx1.4mmx5mm, 4 slices, scan duration: 9.7 s). In the pediatric cohort, each MRE sequence was acquired twice (scan 1 and 2) in the same exam to analyze repeatability.
MRE Reconstruction:
The relative timing of the mechanical driver, breathing motion, and the SE-EPI-MRE acquisition is shown in Figure 1. All MRE data were reconstructed inline. HS was measured with 90% confidence interval (CI)(9, 10) and averaged over 4 slices.
Analysis:
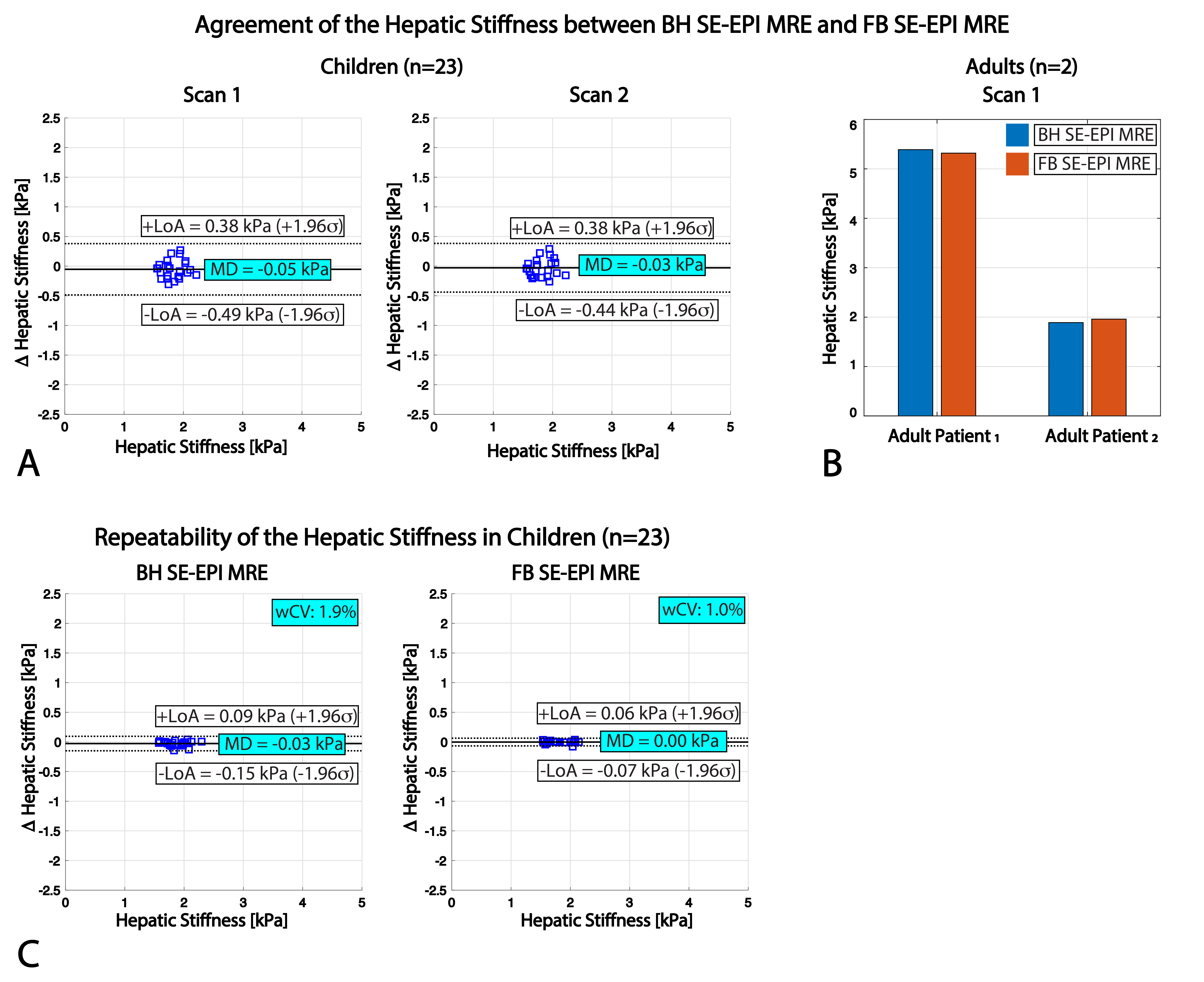
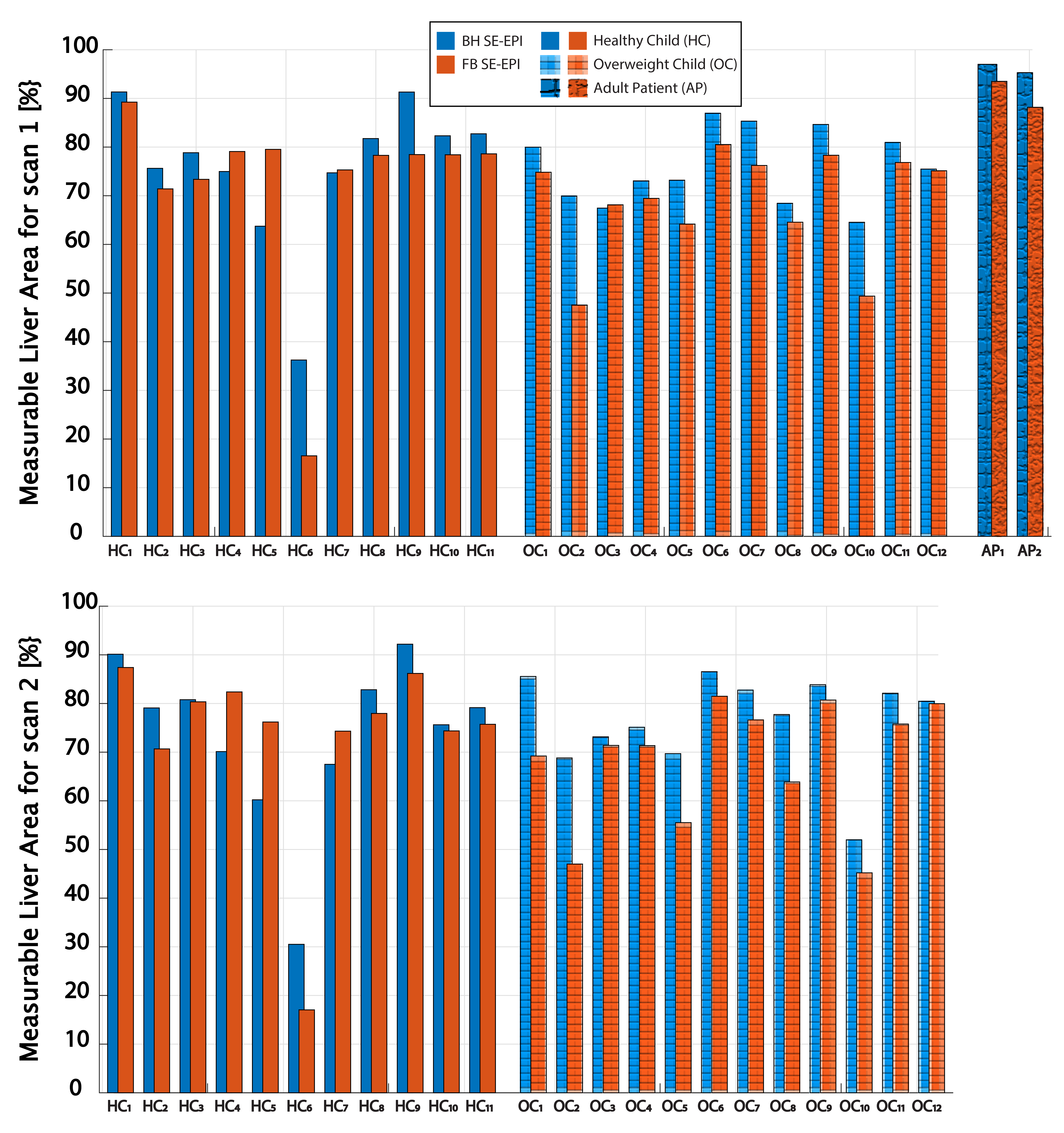
In children, Bland-Altman (BA) analysis of the mean differences (MD) and 95% limits of agreements (LoA) was used to evaluate the agreement between BH and FB SE-EPI-MRE(11, 12). Repeatability was assessed using BA analysis and the within-subject coefficient of variation (wCV). Bar plots were used to evaluate the agreement of HS in adults. We evaluated the quality of HS maps by the measurable liver area, defined as the ratio of the area 90% CI on the stiffness confidence mask to the total liver area.
Results
Figure 2 shows representative results in an adult. The HS from both BH and FB SE-EPI-MRE were consistent with biopsy findings of steatohepatitis and early cirrhosis. Images from a representative child are shown in Figure 3. Figure 4A-B illustrate close agreement of HS between BH and FB SE-EPI-MRE in 23 children and 2 adults, respectively. Scans in children showed smaller wCV and MD for FB than BH SE-EPI-MRE (Figure 4C). BH and FB SE-EPI-MRE led to similar measurable liver area in all scans (Figure 5).Discussion
We showed that FB SE-EPI-MRE can rapidly (9.7 s) quantify HS, with close agreement of HS vs. BH SE-EPI-MRE. The grading from the FB and BH SE-EPI-MRE imaging and biopsy results were consistent in the adult subjects.Both FB and BH SE-EPI-MRE achieved acceptable repeatability in children (<7%) as recommended by the Quantitative Imaging Biomarkers Alliance (QIBA) profile for MRE of the liver (13). FB SE-EPI-MRE produced more repeatable HS with smaller wCV and MD and tighter LoA.
The FB SE-EPI-MRE method evaluated in this study manages motion by acquiring “snapshots” of the motion-encoded slice with narrow temporal footprints compared to typical breathing motion. There could be a mixture of information due to displacement of liver tissue in/out of the imaging slice during respiration and motion encoding. This may still be adequate when calculating a mean HS value in the presence of diffuse liver disease, as seen in the initial results.
Conclusion
In this pilot study, FB SE-EPI-MRE without dedicated motion compensation could accurately quantify hepatic stiffness with good repeatability and large measurable liver area.Acknowledgements
This work was supported by the National Institutes of Health under Award Numbers NIH/NIDDK R01DK124417 and NIH/NIBIB U01EB031894, and the National Center for Advancing Translational Sciences under Award Number UL1TR001881.The authors thank investigators at the Mayo Clinic for providing the prototype flexible MRE passive driver suitable for children. The authors thank the clinicians, study coordinators and the MRI technologists at UCLA.References
1. Kim YS, Jang YN, Song JS: Comparison of gradient-recalled echo and spin-echo echo-planar imaging MR elastography in staging liver fibrosis: a meta-analysis. Eur Radiol 2018; 28:1709–1718.
2. Serai SD, Dillman JR, Trout AT: Spin-echo Echo-planar Imaging MR Elastography versus Gradient-echo MR Elastography for Assessment of Liver Stiffness in Children and Young Adults Suspected of Having Liver Disease. Radiology 2017; 282:761–770.
3. Wagner M, Besa C, Ayache JB, et al.: Magnetic resonance elastography of the liver: Qualitative and quantitative comparison of gradient echo and spin echo echoplanar imaging sequences. Invest Radiol 2016; 51:575–581.
4. Armstrong T, Santos SG, Ly K V, et al.: Assessment of Spin-Echo and Gradient-Echo Liver MRE in Healthy Children and Children with Suspected Fibrosis at 3 T. ISMRM 2019
5. Choi SL, Lee ES, Kannengiesser S, et al.: Technical success rates and reliability of spin-echo echo-planar imaging ( SE-EPI ) MR elastography in patients with chronic liver disease or liver cirrhosis. 2020:1730–1737.6. Murphy IG, Graves MJ, Reid S, et al.: Comparison of breath-hold, respiratory navigated and free-breathing MR elastography of the liver. Magn Reson Imaging 2017; 37:46–50.
7. Morin CE, Dillman JR, Serai SD, Trout AT, Tkach JA, Wang H: Comparison of Standard Breath-Held, Free-Breathing, and Compressed Sensing 2D Gradient-Recalled Echo MR Elastography Techniques for Evaluating Liver Stiffness. 2018(December):279–287.
8. Wang H, Tkach JA, Trout AT, Dumoulin CL, Dillman JR: Respiratory-triggered spin-echo echo-planar imaging-based mr elastography for evaluating liver stiffness. Journal of Magnetic Resonance Imaging 2019; 50:391–396.
9. Kafali SG, Bolster BD Jr, Shih S, et al.: Self-Navigated Radial Free-Breathing Magnetic Resonance Elastography of the Liver with Rapid Motion Encoding in Children at 3T. ISMRM 2022.
10. Kafali SG, Armstrong T, Shih SF, et al.: Free-breathing radial magnetic resonance elastography of the liver in children at 3 T: a pilot study. Pediatr Radiol 2022.
11. Obuchowski NA, Reeves AP, Huang EP, et al.: Quantitative imaging biomarkers: A review of statistical methods for computer algorithm comparisons. Stat Methods Med Res 2015; 24:68–106.
12. Raunig DL, McShane LM, Pennello G, et al.: Quantitative imaging biomarkers: A review of statistical methods for technical performance assessment. Stat Methods Med Res 2015; 24:27–67.
13. May CP: QIBA Profile: Magnetic Resonance Elastography of the Liver 5 Stage 2: Consensus Profile. 2018.
Figures