4794
Impact of Oral Contrast Agents on Terminal Ileum Viscoelastic Properties Assessed by MR Enterography and MR Elastography1Radiology, Charité – Universitätsmedizin Berlin, Berlin, Germany, 2BIH Charité Digital Clinician Scientist Program, Berlin Institute of Health at Charité – Universitätsmedizin Berlin, BIH Biomedical Innovation Academy, Berlin, Germany, 3Surgery, Charité – Universitätsmedizin Berlin, Berlin, Germany, 4Gastroenterology, Infectious Disease, Rheumatology, Charité – Universitätsmedizin Berlin, Berlin, Germany, 5iPATH.Berlin-Immunopathology for Experimental Models, Charité – Universitätsmedizin Berlin, Berlin, Germany, 6Internal Medicine, Gemeinschaftskrankenhaus Havelhöhe, Berlin, Germany, 7Medical Informatics, Charité – Universitätsmedizin Berlin, Berlin, Germany, 8Radiology, Helios Klinikum Emil von Behring, Berlin, Germany
Synopsis
Keywords: Elastography, Elastography
Motivation: Although the feasibility of intestinal MR elastography has recently been demonstrated, the influence of bowel distension through oral contrast agents on gut viscoelastic properties remains elusive.
Goal(s): To investigate the influence of oral contrast agent-based bowel distension on the viscoelastic properties of the gut in healthy volunteers.
Approach: Healthy volunteers were scanned using MR enterography and MR elastography before and after the ingestion of 1000 ml of 2 % mannitol solution as oral contrast agent.
Results: Our results suggest that the bowel distension in MR enterography has no systematic impact on viscoelastic tissue properties of the terminal ileum.
Impact: This study suggests that bowel distension in MR enterography has no systematic impact on the assessment of viscoelastic tissue properties of the terminal ileum. Consequently, future studies investigating inflammatory bowel disease using intestinal MR elastography do not need to account for potential biases related to pre-stretched bowel walls after oral ingestion of contrast agents.
Introduction
While conventional MR enterography has been established for detecting inflammatory bowel disease (IBD), its ability to characterize strictures for therapeutic planning is limited (1,2). Standard clinical MR enterography protocols involve the ingestion of 450-1000 ml hyperosmolar oral contrast agents about 45 minutes before the MRI scan (1-3). MR elastography has been established in clinical practice for staging hepatic fibrosis (4) while more recently, its feasibility in the gut has been demonstrated (5-8). However, bowel distension may systematically impact the assessment of IBD-related lesions and influence the design of future studies. Hence, our study aimed to investigate healthy volunteers before and after the ingestion of an oral contrast agent using MR elastography.Methods
This prospective single-center study was approved by the local IRB and all volunteers gave informed written consent. A total of 20 healthy volunteers were investigated. Multifrequency MR elastography with tomoelastography post-processing has been performed as previously described (5). Scans were performed at 1.5 Tesla (Magnetom Aera, Siemens Healthineers, Erlangen, Germany) with mechanical drive frequencies of 40, 50, 60 and 70 Hz. Moreover, conventional coronal and axial T2-weighted half-Fourier acquisition single-shot turbo spin-echo sequences were acquired to assess the distribution of the oral contrast agent within the gut, and to ensure inclusion of the terminal ileum on MR elastography scans. All volunteers were scanned twice with the same set of sequences: before and approximately 45 min after the ingestion of 1000 ml of a 2 % mannitol solution as oral contrast agent. Maps of shear wave speed (c in ms-1) as a representation of stiffness, and maps of loss angle (φ in rad) as a representation of viscous behavior were generated (9). A board-certified radiologist (S.R.) drew volumes of interest (VOIs) based on c-maps in conjunction with magnitude images.Results
Mean age of participants was 33.2 ± 8.2 years and mean body mass index was 23.3 ± 2.2 kg/m2 (n = 20, 10 women and 10 men). Representative viscoelastic maps and conventional MR images are shown in figure 1. For the terminal ileum, the mean VOI was 21.25 ± 12.09 cm3. For mean c and φ, there was no significant difference before vs. after the ingestion of an oral contrast agent for the terminal ileum (mean c: 1.47 ± 0.24 ms-1 vs. 1.40 ± 0.25 ms-1 with p = 0.37; and mean φ: 0.70 ± 0.12 rad vs. 0.68 ± 0.12 rad with p = 0.61). Corresponding boxplots are shown in figure 2. No significant correlation was found between MR elastography parameters (c and φ) and age (before: p = 0.64 and 0.58; after: p = 0.65 and 0.53; respectively) or body mass index (before: p = 0.92 and 0.32; after: p = 0.45 and 0.24; respectively).Discussion
This pilot study was aimed at investigating the influence of oral contrast agent-based bowel distension on the viscoelastic properties of the terminal ileum in healthy volunteers using MR elastography. After the ingestion of oral contrast agents, there was no statistically significant difference of viscoelastic properties for the terminal ileum. Moreover, no correlation was found between MR elastography parameters and age or body mass index. Our results suggest that the bowel distension in MR enterography has no systematic impact on the assessment of the viscoelastic properties of the terminal ileum.Standard clinical MR enterography has been assessed by many studies which has led to the development of several scoring systems for disease activity such as the Magnetic Resonance Index of Activity (10) or the Acute Inflammation Score (11). Those scores –which are mainly used for study purposes– were developed and validated using oral contrast agents which emphasizes the need to investigate its impact on biomechanical tissue properties of the gut.
This study has limitations. First, only a small number was included in this pilot study. Second, no antispasmodic medication was applied to healthy volunteers for ethical reasons. Finally, despite recent advances of spatial resolution and noise robustness of elastograms, regions of interest were smaller in healthy volunteers with a mural thickness of approximately 1-3 mm compared to inflammatory bowel disease patients with increased mural thickness >3 mm (11). To reduce this technical limitation, we have assessed the bowel wall on multiple slices (volumes of interest).
Conclusion
This study suggests that bowel distension in MR enterography has no systematic impact on the assessment of biomechanical tissue properties of the terminal ileum.Acknowledgements
This study was funded by the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation): SFB 1340/1 “Matrix in Vision” project number 372486779 (Bernd Hamm, Jürgen Braun, Ingolf Sack), GRK 2260 BIOQIC (Ingolf Sack, Jürgen Braun). Rolf Reiter is a participant of the BIH-Charité Digital Clinician Scientist Program funded by Charité – Universitätsmedizin Berlin, Berlin Institute of Health and the DFG.
References
1. Maaser C, Sturm A, Vavricka SR, Kucharzik T, Fiorino G, Annese V, et al. ECCO-ESGAR Guideline for Diagnostic Assessment in IBD Part 1: Initial diagnosis, monitoring of known IBD, detection of complications. J Crohns Colitis. 2019;13(2):144-64.
2. Sturm A, Maaser C, Calabrese E, Annese V, Fiorino G, Kucharzik T, et al. ECCO-ESGAR Guideline for Diagnostic Assessment in IBD Part 2: IBD scores and general principles and technical aspects. J Crohns Colitis. 2019;13(3):273-84.
3. Loch FN, Kamphues C, Beyer K, Klauschen F, Schineis C, Weixler B, et al. Diagnostic Accuracy of Magnetic Resonance Enterography for the Evaluation of Active and Fibrotic Inflammation in Crohn's Disease. Front Surg. 2022;9:872596.
4. Reiter R, Tzschatzsch H, Schwahofer F, Haas M, Bayerl C, Muche M, et al. Diagnostic performance of tomoelastography of the liver and spleen for staging hepatic fibrosis. Eur Radiol. 2020;30(3):1719-29.
5. Reiter R, Loch FN, Kamphues C, Bayerl C, Marticorena Garcia SR, Siegmund B, et al. Feasibility of Intestinal MR Elastography in Inflammatory Bowel Disease. J Magn Reson Imaging. 2022;55(3):815-22.
6. Jensen L, Loch FN, Kamphues C, Shahryari M, Garcia SRM, Siegmund B, et al. Feasibility of In Vivo MR Elastography of Mesenteric Adipose Tissue in Crohn’s Disease. Quant Imaging Med Surg. 2023;13(8):4792-4805.
7. Loch FN, Kamphues C, Beyer K, Schineis C, Asbach P, Reiter R, Sack I, Braun J. Ex vivo magnetic resonance elastography of the small bowel in Crohn's disease. Quant Imaging Med Surg. 2023;13(5):2895-2906.
8. van Schelt AS, Beek KJ, Wassenaar NPM, Schrauben EM, Runge JH, Gecse KB, van der Bilt JDW, Neefjes-Borst EA, Buskens CJ, Nederveen AJ, Stoker J. Viscoelastic properties of small bowel mesentery at MR elastography in Crohn's disease: a prospective cross-sectional exploratory study. Eur Radiol Exp. 2023;7(1):53.
9. Tzschätzsch H, Guo J, Dittmann F, Hirsch S, Barnhill E, Jöhrens K, Braun J, Sack I. Tomoelastography by multifrequency wave number recovery from time-harmonic propagating shear waves. Med Image Anal. 2016;30:1-10.
10. Rimola J, Ordas I, Rodriguez S, Garcia-Bosch O, Aceituno M, Llach J, et al. Magnetic resonance imaging for evaluation of Crohn's disease: validation of parameters of severity and quantitative index of activity. Inflamm Bowel Dis. 2011;17(8):1759-68.
11. Steward MJ, Punwani S, Proctor I, Adjei-Gyamfi Y, Chatterjee F, Bloom S, et al. Non-perforating small bowel Crohn's disease assessed by MRI enterography: derivation and histopathological validation of an MR-based activity index. Eur J Radiol. 2012;81(9):2080-8.
Figures
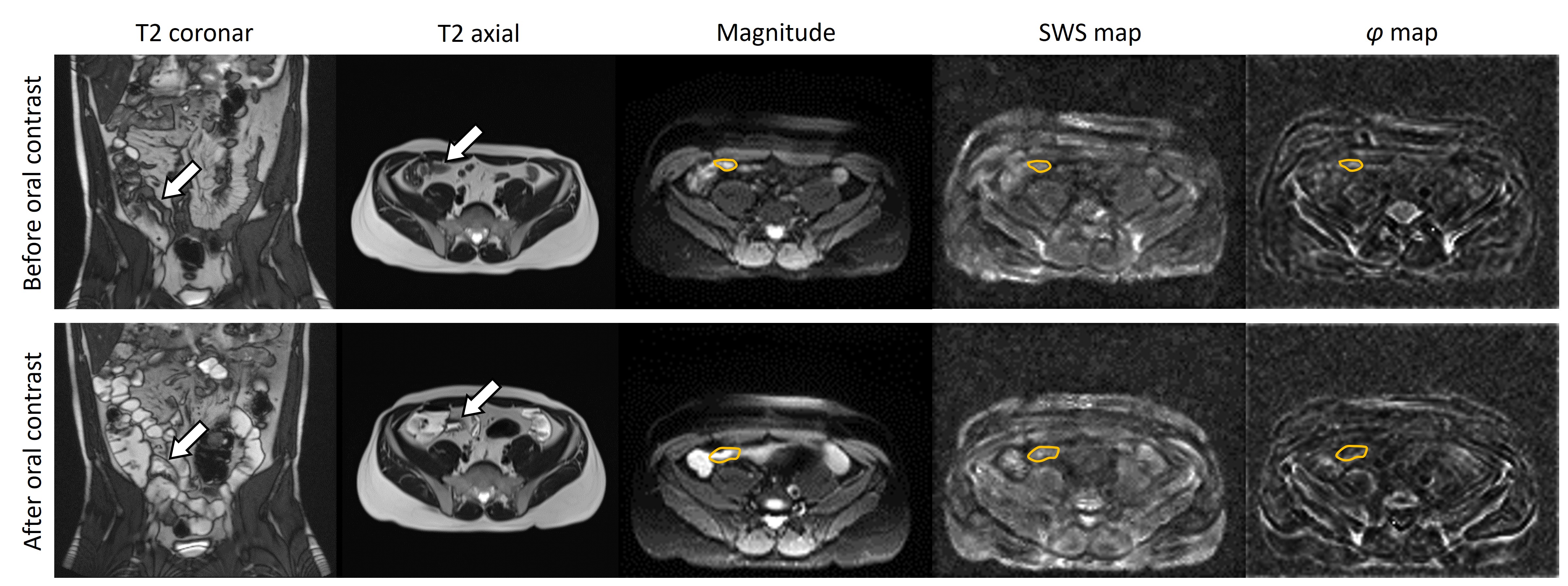
Figure 1. Healthy 31-year-old man before and after the ingestion of 1000 ml 2% mannitol solution as oral contrast. Before oral contrast: shear wave speed (SWS) of 1.21 ± 0.28 m/s and loss angle (φ) of 0.71 ± 0.23 rad. After oral contrast: SWS of 1.39 ± 0.40 m/s and loss angle (φ) of 0.68 ± 0.28 rad. White arrows indicate the terminal ileum on T2 images. Regions of interest are shown by orange lines on magnitude images, SWS and φ maps.
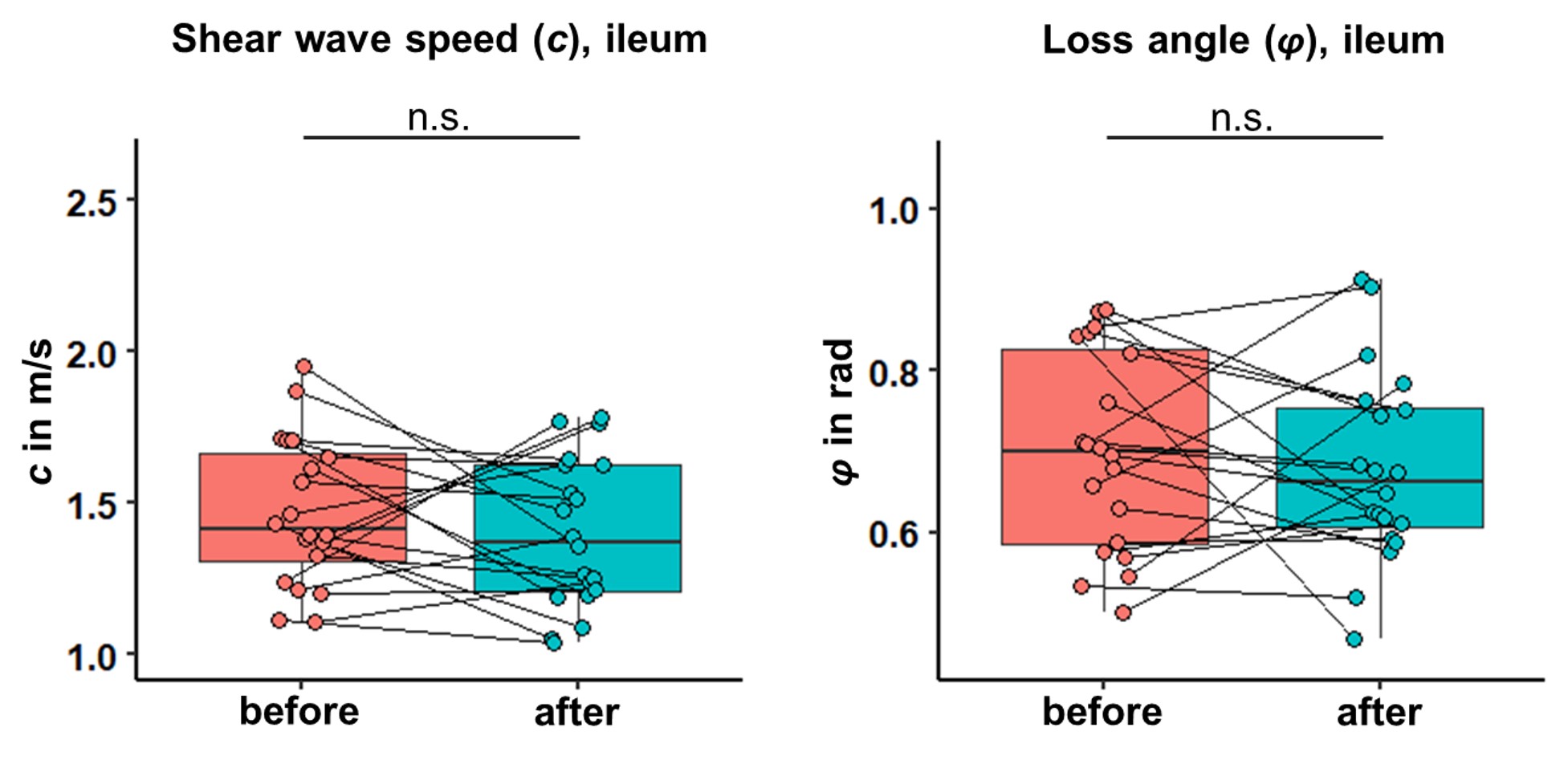
Figure 2. Box plots of shear wave speed and loss angle for the terminal ileum.