4789
Free-Breathing 3D Cardiac Magnetic Resonance Elastography Using TURBINE-MRE1Department of Radiology, Mayo Clinic, Rochester, MN, United States, 2Department of Physiology and Biomedical Engineering, Mayo Clinic, Rochester, MN, United States, 3Department of Cardiovascular Medicine, Mayo Clinic, Rochester, MN, United States, 4Women's Health Research Center, Mayo Clinic, Rochester, MN, United States
Synopsis
Keywords: Elastography, Elastography, Cardiac, free-breathing, 3D
Motivation: Cardiac magnetic resonance elastography (cMRE) has potential for clinically vital quantitative imaging of myocardial stiffness, but for it to become clinically viable in patients with heart failure or shortness of breath, free-breathing techniques need to be developed.
Goal(s): To demonstrate the feasibility of 3D free-breathing cMRE.
Approach: A 3D MRE sequence (TURBINE-MRE) was utilized for data acquisition. Physiologic signals were recorded and used to partition data into distinct cardiac and respiratory states. With a specified signal model, we iteratively reconstructed image volumes for all states.
Results: Stiffness estimates throughout the cardiac cycle were successfully obtained in two volunteers, demonstrating successful free-breathing 3D cMRE.
Impact: Free-breathing cMRE will enable quantitative imaging of myocardial stiffness in a significant number of patients who are not able to perform long breath-holds. A 3D TURBINE-MRE acquisition enables temporal resolution of the heart's elastic properties throughout the cardiac cycle.
Introduction
Magnetic resonance elastography (MRE)1,2 is a quantitative imaging method enabling estimation of tissue stiffness and elastic properties. Cardiac MRE (cMRE) is very challenging due to factors including (but not limited to) motion, thin-walled tissues, and limited wave penetration. cMRE has been demonstrated primarily with 2D multislice imaging, potentially limiting temporal resolution, and introducing vulnerability to interslice phase variation3. cMRE has also primarily been pursued with electrocardiogram gating, limiting stiffness estimates to fewer cardiac states; and with breath-held scans4–7, which are unreliable in patients with shortness of breath.Recently, an MRE sequence employing hybrid radial-Cartesian 3D encoding of k-space (TURBINE8) has enabled free-breathing elastography of the brain9, liver10, and kidneys11. TURBINE-MRE employs repeated echo planar imaging (EPI) readouts rotated about the kz axis by golden angle increments. This provides efficient and balanced k-space coverage through time, and thereby through varying physiologic and MRE-encoding states. In this work we show that free-breathing, 3D cMRE is feasible using TURBINE-MRE with data partitioning of distinct respiratory and cardiac states.
Methods
Acquisition: Following IRB-approval and written informed consent, volunteers were scanned on a GE 1.5T Signa scanner. A custom cardiac MRE passive driver5 was placed on each subject’s chest during the scan. Respiratory belt and photoplethysmogram (PPG) data were collected during scanning. TURBINE-MRE imaging parameters were: matrix (readout/phase-encode/coils/blades per MRE-encoding)=(250/32/26/198), 2x phase-encoded acceleration, TR/TE=70/22.8-ms, 6 motion-encoding directions, 4 phase offsets, 100-Hz driving frequency, 384x192-mm FOV, 3-mm isotropic spatial resolution, with one repeat of all 24 MRE-encodings after their initial scan for 2x overall acquisition and total scan time 11:20 m:s.Pre-processing: TURBINE-MRE data were pre-processed with vendor-provided Nyquist ghost correction. Respiratory data were binned into distinct states according to position along the belt waveform. Cardiac data were binned into states utilizing custom beat-to-beat detection with PPG data.
Reconstruction: Targeting an unknown tensor volume $$$X\in\mathbb{C}^{N_s\times N_{t_R}\times N_{t_C}\times N_p\times N_m}$$$ where $$$N_s,N_{t_R},N_{t_C},N_p$$$, and $$$N_m$$$ respectively denote numbers of spatial voxels, respiratory states, cardiac states, phase offsets, and motion-encodings respectively, we work directly with the mode-1 unfolding12 $$$X_{(1)}\in\mathbb{C}^{N_s\times (N_{t_R}N_{t_C}N_pN_m)}$$$ and index this matrix's columns by $$$i\in[0,N_{t_R}N_{t_C}N_pN_m\overset{\Delta}{=}N_i)$$$. The observed signal for an $$$i$$$th encoded physiologic state is modeled as
$$g_i=A_iSX_{(1)}\delta_i+\epsilon_i$$
where $$$A_i$$$ is the TURBINE-MRE encoding operator applicable to the $$$i$$$th state set (as numbers of EPI blades and non-Cartesian trajectories vary according to state), $$$S$$$ are block-diagonal coil sensitivity profiles, $$$\delta_i$$$ is Kronecker's delta, and $$$\epsilon_i$$$ is an instance of complex Gaussian noise. We reconstruct $$$X$$$ by solving
$$\underset{X}{\text{arg min}}\sum_{i=0}^{N_i-1}\lVert A_iSX_{(1)}\delta_i-g_i\rVert_2^2+\lambda\sum_{i=0}^{N_i-1}\lVert X_{(1)}\delta_i\rVert_2^2$$
with 50 iterations of a conjugate gradient solver, where $$$\lambda$$$ is a Tikhonov regularization parameter (here $$$10^{-3}$$$). Jeffrey Fessler's NUFFT13 package was utilized in Matlab (Mathworks, Natick, MA, USA). Data from two subjects were reconstructed with $$$N_{t_R}=3$$$ respiratory and $$$N_{t_C}=5$$$ cardiac states.
Post-Processing: Reconstructed images were corrected for gradient nonlinearity using vendor-provided tools, and sinc-interpolated to 1-mm isotropic resolution (384/384/192 matrix size). Displacement data were obtained and used in computing curl wave images, and elastograms were computed with local frequency estimation (LFE)14.
Analysis: Images from a respiratory state of interest and all cardiac states were assessed. Left ventricular myocardium was manually segmented from axial images; stiffness values within the resulting masks were compared with reference estimates obtained from a separate short-axis 2D multislice EPI-MRE acquisition4.
Results
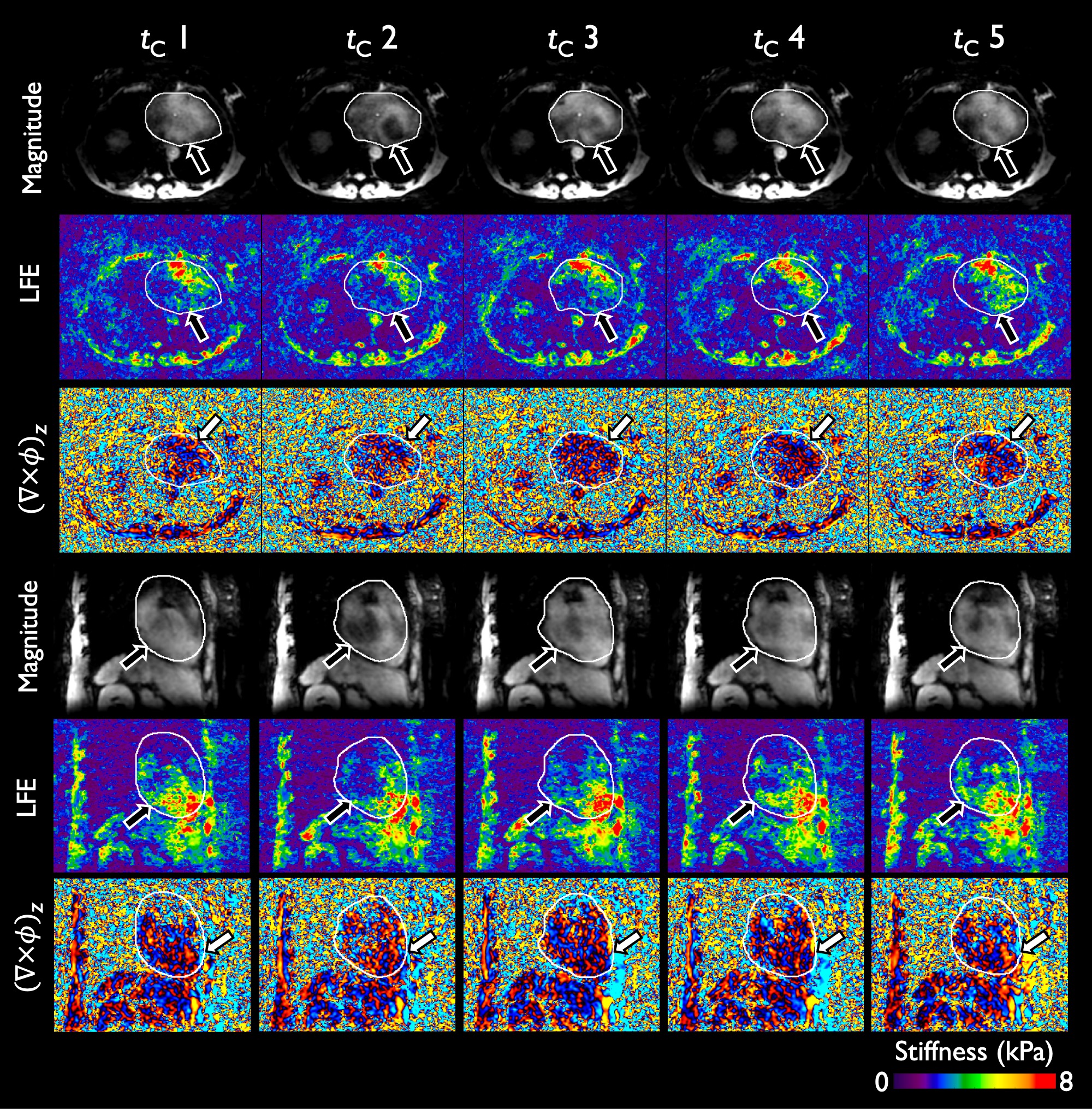
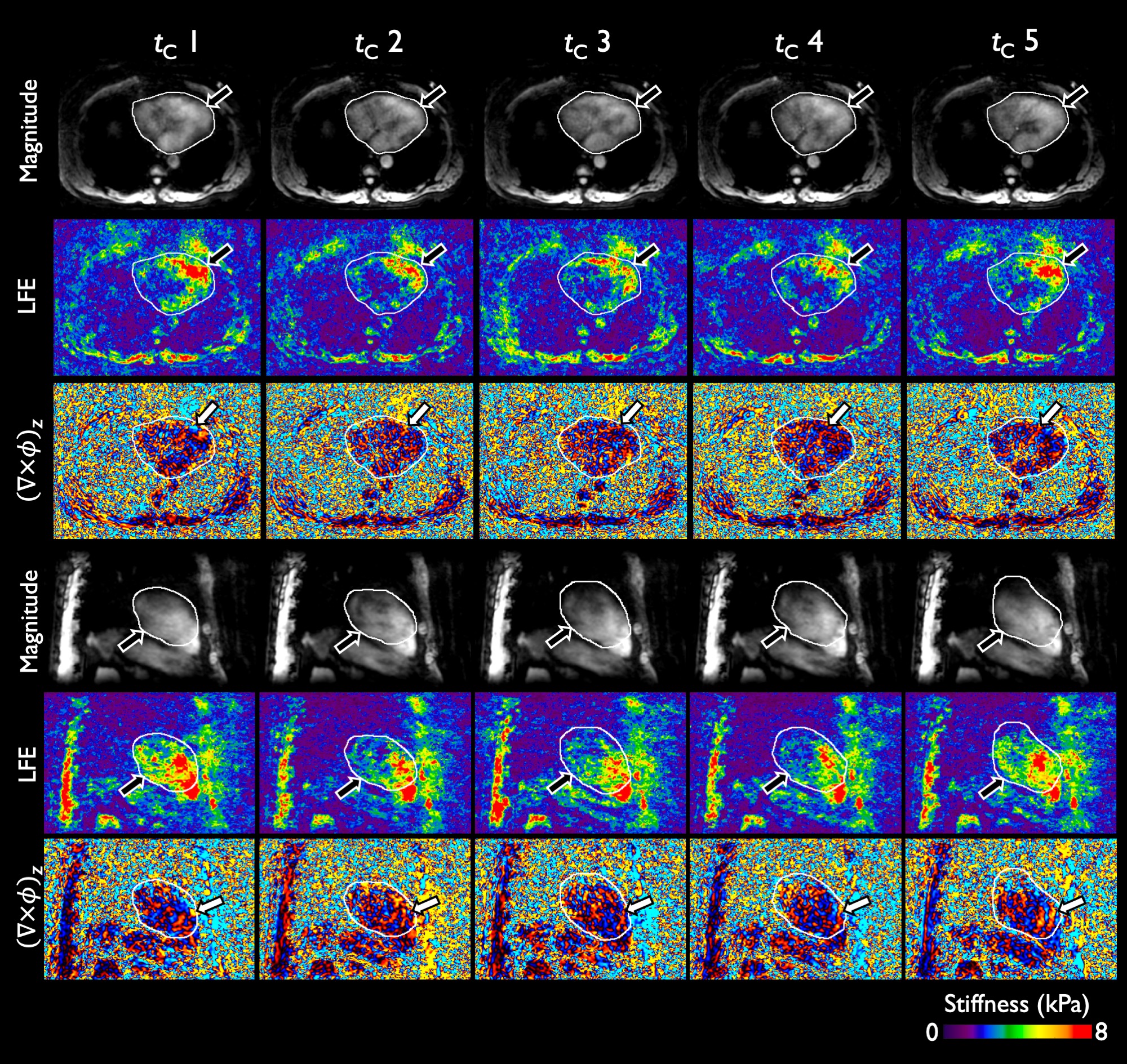
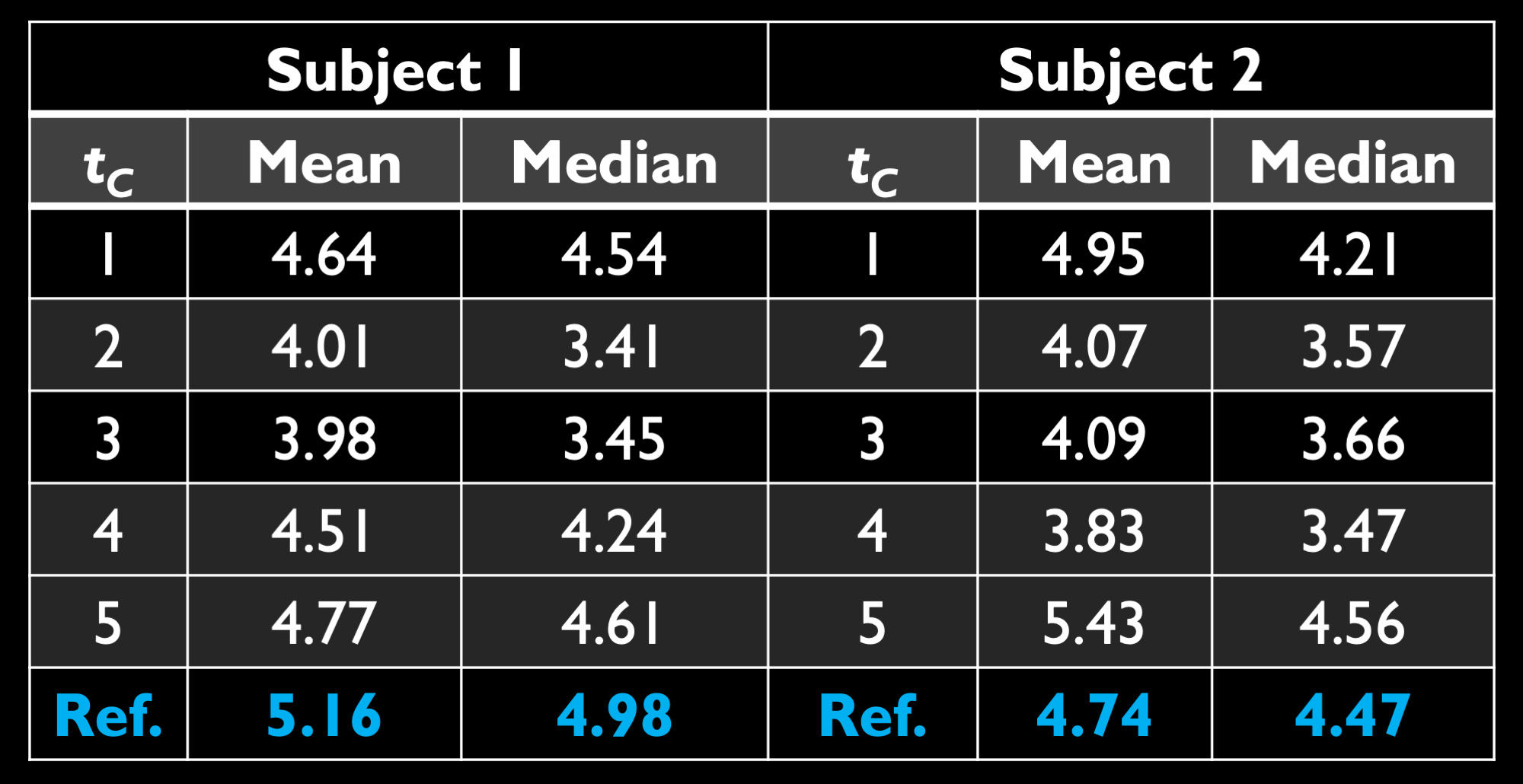
Figure 1 shows magnitude images, elastograms, and curl wave images for one respiratory state (inhaled lungs), and all cardiac states, in axial and sagittal orientations. Figure 2 visualizes results for a second participant in inhalation. In each case, magnitude images show the heart’s changing structure and contrast through cardiac states. Elastograms exhibit clear evolution of stiffness throughout the cardiac cycle, with considerable stiffening of the myocardium in systole. Curl wave images demonstrate increased wavelengths within stiffer tissue in systolic states, and shortened wavelengths in diastole. Figure 3 tabulates stiffness measurements from both subjects, showing changes throughout the cardiac cycle and agreement with reference values.Discussion
This work demonstrates that free-breathing 3D cardiac MRE is feasible with TURBINE-MRE and a suitable reconstruction. Partitioning data into distinct physiologic and MRE-encoded states, combined with golden angle sampling in 3D k-space, yields data sufficient for estimation of elastic properties for distinct respiratory and cardiac phases. Stiffness increased in systolic states and decreased in diastolic states, consistent with prior measurements in animals15. A limitation of this preliminary work is a long scan time, coupled with a basic reconstruction solver to show proof of concept. A reconstruction, which is regularized to further accelerate data acquisition and leverage data redundancy inherent to TURBINE-MRE, is in active development. We anticipate this will also enable reconstruction of additional physiologic states.Acknowledgements
We would like to acknowledge our MR technologists, Jessica Magnuson, and Maria Halverson, for all their assistance with data collection and our study coordinator Kathy Brown for consenting, scheduling, and recruiting all our participants. This study was funded by the NIH K12HD65987-12, 5R01HL115144, 1R01HL151379 grants, and the Mayo Clinic Department of Radiology RDCRAFA1 grant.References
1. Muthupillai R, Lomas DJ, Rossman PJ, et al. Magnetic Resonance Elastography by Direct Visualization of Propagating Acoustic Strain Waves. Science 1995;269(5232):1854-1857.
2. Manduca A, Oliphant TE, Dresner MA, et al. Magnetic resonance elastography: Non-invasive mapping of tissue elasticity. Med Image Anal. 2001;5(4):237-254.
3. Murphy MC, Huston III J, Glaser KJ, et al. Phase Correction for Interslice Discontinuities in Multislice EPI MR Elastography. Proc Intl Soc Magn Reson Med. 2012:3426.
4. Arani A, Arunachalam SP, Chang ICY, et al. Cardiac MR elastography for quantitative assessment of elevated myocardial stiffness in cardiac amyloidosis. J Magn Reson Imaging. 2017;46(5):1361-1367.
5. Arani A, Glaser KJ, Arunachalam SP, et al. In vivo, high-frequency three-dimensional cardiac MR elastography: Feasibility in normal volunteers. Magn Reson Med. 2017;77(1):351-360.
6. Sui Y, Arunachalam SP, Arani A, et al. Cardiac MR elastography using reduced-FOV, single-shot, spin-echo EPI. Magn Reson Med. 2018;80(1):231-238.
7. Arani A, Shivaram AP, Rossman PJ, et al. Cardiac Magnetic Resonance Elastography for the Diagnosis of Patients with Heart Failure with Preserved Ejection Fraction. Proc Intl Soc Magn Reson Med. 2018:0285.
8. McNab JA, Gallichan D, Miller KL. 3D steady-state diffusion-weighted imaging with trajectory using radially batched internal navigator echoes (TURBINE). Magn Reson Med. 2010;63(1):235-242.
9. Sui Y, Arani A, Trzasko JD, et al. TURBINE-MRE: A 3D hybrid radial-Cartesian EPI acquisition for MR elastography. Magn Reson Med. 2021;85(2):945-952.
10. Sui Y, Li J, Trzasko JD, et al. Respiratory Motion-Resolved Free-Breathing MR Elastography Of Liver. Proc Intl Soc Magn Reson Med. 2021:0029.
11. Sui Y, Li J, Zhu Z, et al. Free-Breathing MR Elastography of the Kidneys Using TURBINE-MRE. Proc Intl Soc Magn Reson Med. 2022:2236.
12. Kolda TG, Bader BW. Tensor Decompositions and Applications. SIAM Rev. 2009;51(3):455-500.
13. Fessler JA, Sutton BP. Nonuniform fast Fourier transforms using min-max interpolation. IEEE Trans Signal Process. 2003;51(2):560-574.
14. Manduca A, Muthupillai R, Rossman PJ, et al. Local wavelength estimation for magnetic resonance elastography. Proceedings of 3rd IEEE International Conference on Image Processing. Vol 3.; 1996:527-530.
15. Kolipaka A, Araoz PA, McGee KP, et al. Magnetic resonance elastography as a method for the assessment of effective myocardial stiffness throughout the cardiac cycle. Magn Reson Med. 2010;64(3):862-870.
Figures