4787
Magnetic Resonance Elastography as a Prognostic Tool for Surgical Outcomes in Normal Pressure Hydrocephalus1Department of Radiology, Mayo Clinic College of Medicine, Rochester, MN, United States
Synopsis
Keywords: Diagnosis/Prediction, Brain, Dementia
Motivation: Normal pressure hydrocephalus (NPH) is a treatable cause of dementia. The treatment with ventriculoperitoneal shunt surgery can lead to sustained improvement in about 80% of cases. However, due to the invasive nature of surgery, improving the predictability of outcomes is imperative.
Goal(s): To assess magnetic resonance elastography (MRE) as a non-invasive tool to predict surgical outcomes in NPH.
Approach: Pre-surgical stiffness and damping ratio pattern scores were used as features to train classification models that predict clinical improvement following shunt placement.
Results: MRE is a promising noninvasive tool for prediction of surgical outcomes in normal pressure hydrocephalus.
Impact: MRE demonstrates promise as a prognostic tool for prediction of surgical outcomes in NPH. If successfully translated to clinic, this would provide patients with non-invasive alternative.
INTRODUCTION
Normal pressure hydrocephalus (NPH) is a CSF dynamics disorder1 with clinical symptoms of cognitive decline, gait disturbance, and urinary incontinence2, 3. NPH can be treated with ventriculoperitoneal shunt surgery4 with sustained improvement in about 80% of cases5, 6. However, due to the invasive nature of surgery, improving the predictability of outcomes is imperative. Different morphologic phenotypes of NPH have been demonstrated to be associated with unique mechanical signatures measured by magnetic resonance elastography (MRE). In this study, we tested the hypothesis that MRE-based mechanical signatures can be used to predict surgical outcomes. Two feature spaces were considered to determine if a more-detailed, phenotype-specific set of features could improve this prediction.METHODS
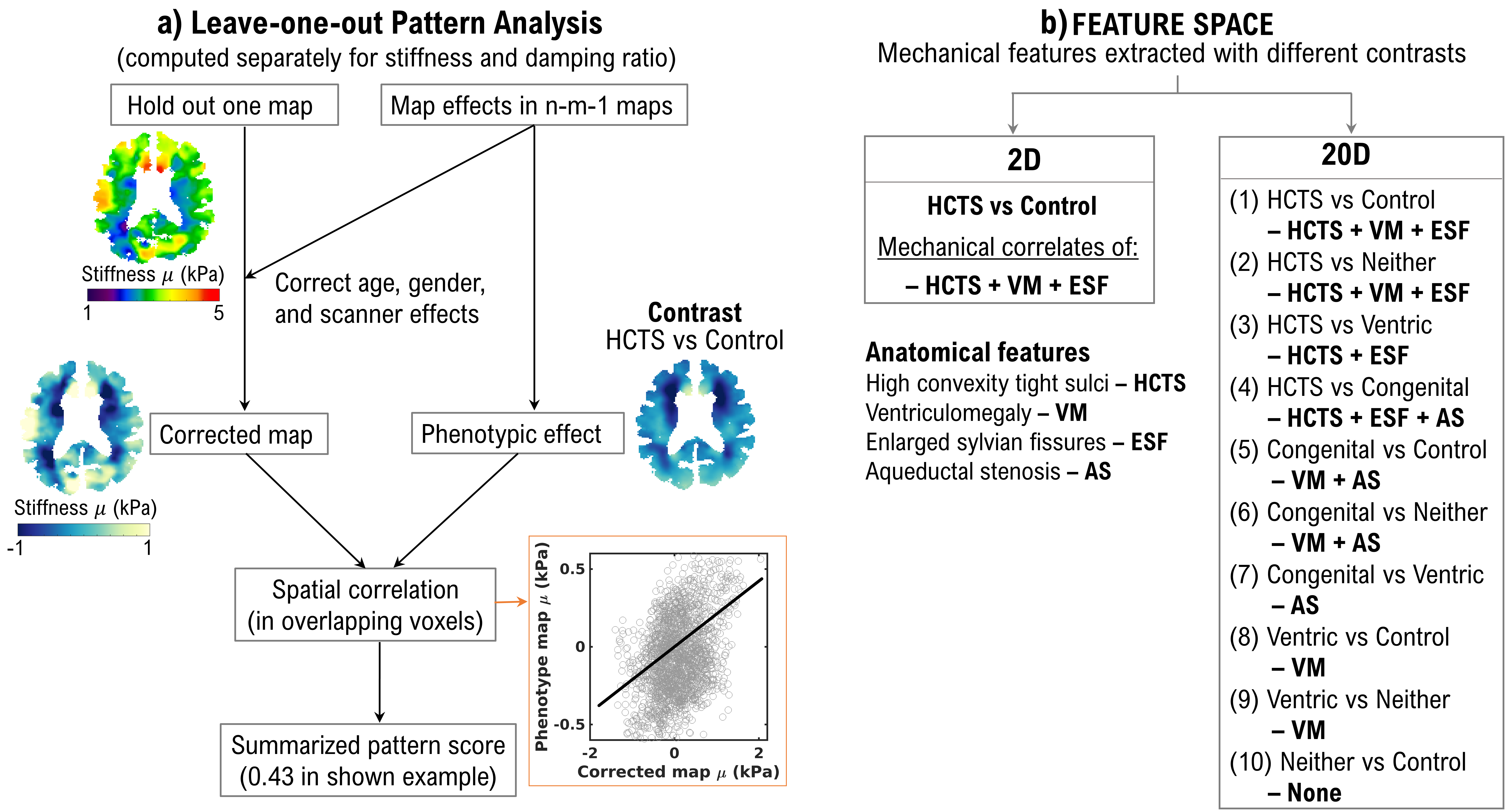
MRE and structural imaging were performed in 128 suspected NPH patients and 44 control participants. A neuroradiologist classified patients with suspected NPH into four subgroups based on their morphologic features assessed on structural imaging: (1) high convexity tight sulci (HCTS7), (2) congenital hydrocephalus (Congenital), (3) ventriculomegaly alone (Ventric), and (4) neither ventriculomegaly nor HCTS (Neither). Sixty-eight participants who had normal opening CSF pressure (< 25 cm water) during lumbar puncture and gait improvement with the spinal tap test underwent treatment with ventriculoperitoneal shunt placement. Of these patients, 54 were shunt responders8 and 14 were non-responders, based on patient report, gait exam/analysis, and/or mental status exam. Stiffness and damping ratio maps were computed from MRE displacement data using neural network inversion9. After mechanical property estimation, maps were warped into template space for analyses10. Mechanical signatures associated with each phenotype were summarized using pattern analysis11 method described in Figure 1(a). By contrasting one group versus another, we computed pattern scores that reflect the viscoelastic alterations associated with the unshared anatomical features between the two groups. With 5 groups, there were 10 contrasts. The summarized pattern scores were used as features to train support vector machine (SVM) classification models and predict surgical outcomes for two feature spaces: a limited 2-dimensional (2D) feature space that included the most common features found in NPH, and an expanded 20-dimensional (20D) feature space that included features from all four morphologic subgroups as shown in Figure 1(b). We compared the two SVM models using permutation tests for following performance metrics: area under the receiver operating curve (AUROC), accuracy, diagnostic odds ratio (DOR), positive predictive value (PPV), and negative predictive value (NPV).RESULTS
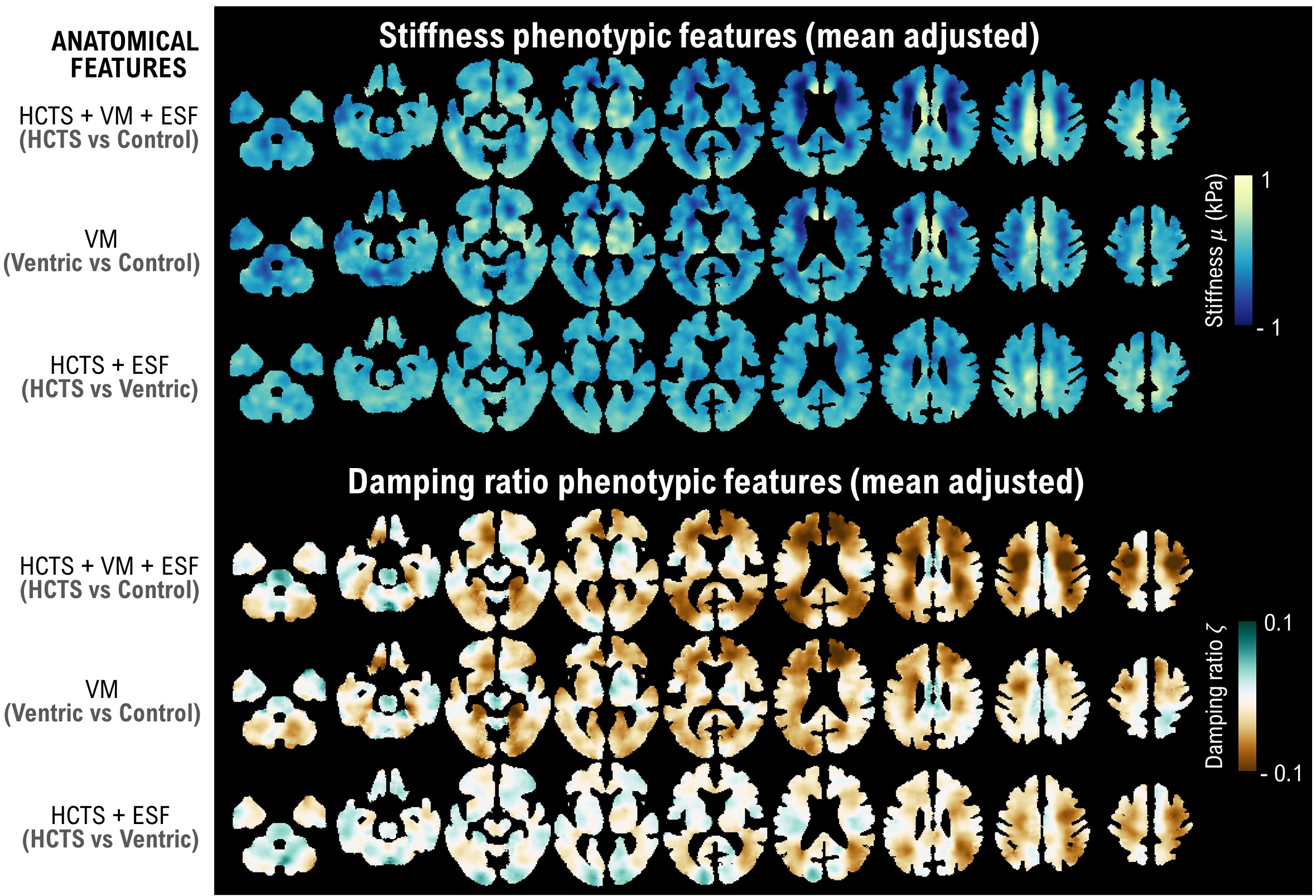
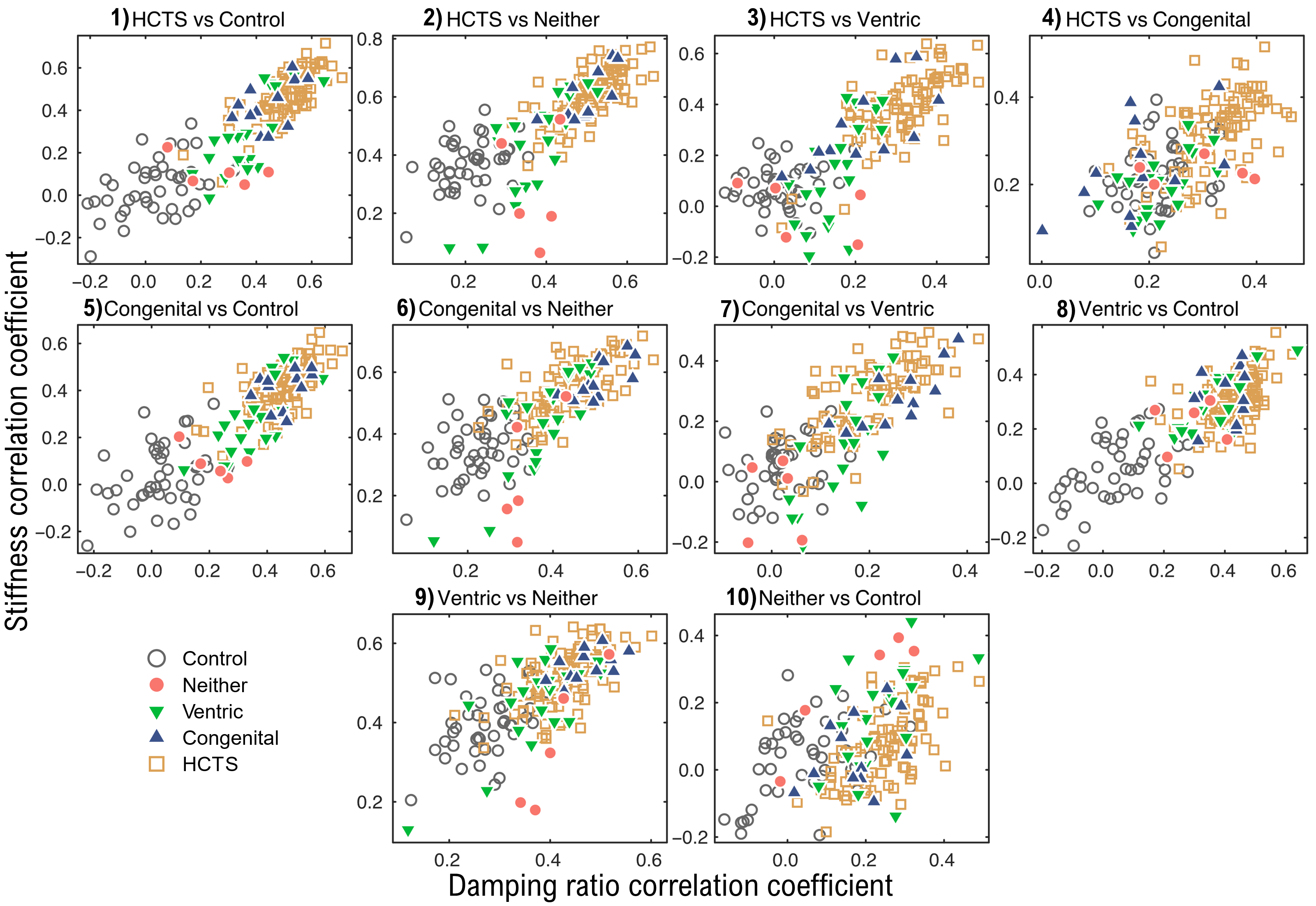
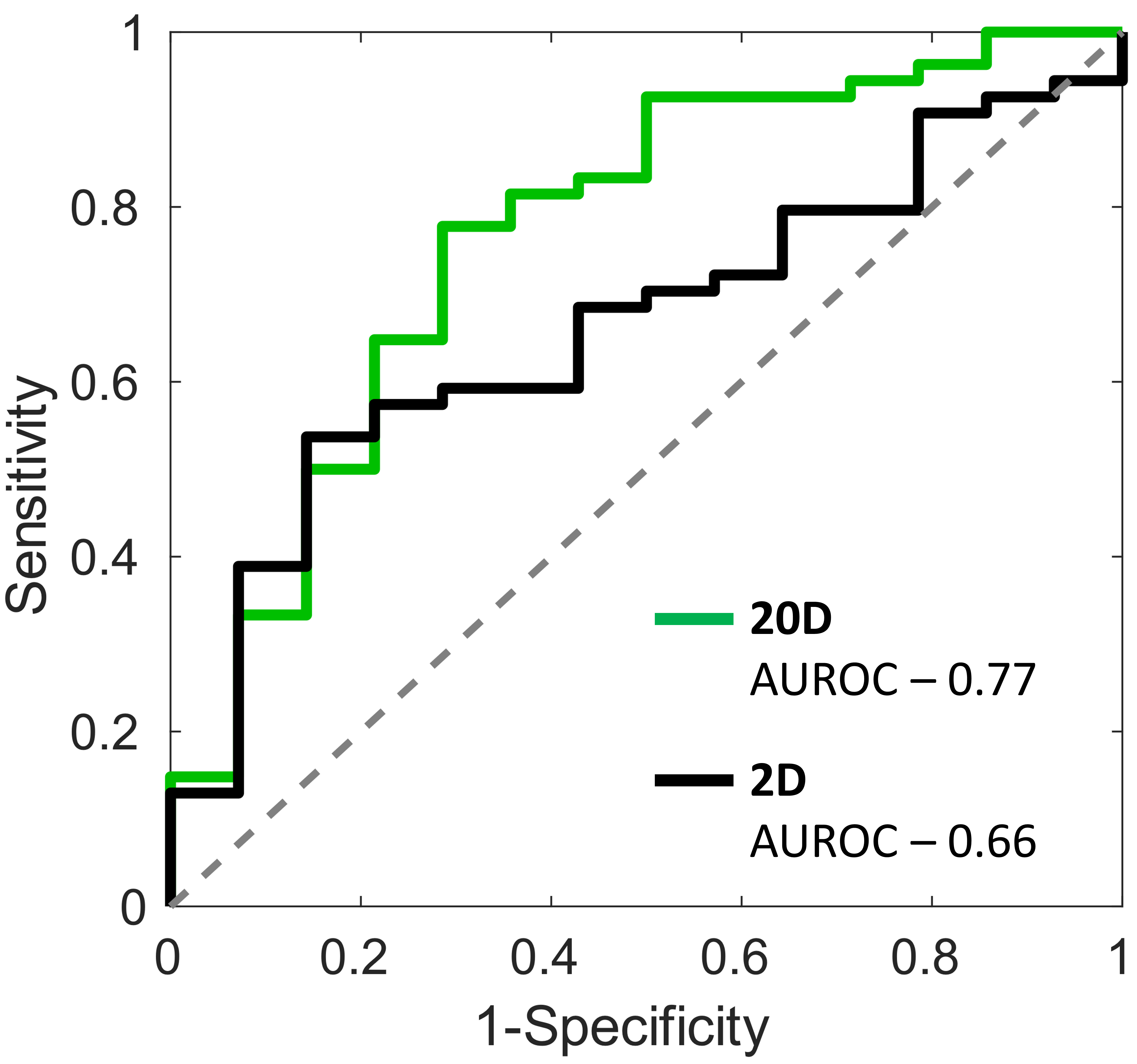
The most discriminative mechanical signatures are presented in Figure 2. In Figure 3, scatter plots of damping ratio and stiffness pattern scores are shown for the 10 contrasts. In HCTS versus Control (Figure 3.1), HCTS and control cases formed distinct clusters. This contrast reflects the mechanical correlates of enlarged ventricles, enlarged sylvian fissures, and tightening of sulci at the vertex of the brain (Figure 2). In Figure 3.2, HCTS vs Neither contrast showed further separation of cases between the two groups. In the HCTS versus Ventric contrast (Figure 3.3), features reflect the tightening of sulci at the vertex and enlarged sylvian fissures, since the two groups have ventriculomegaly in common. In Figure 3.4, pattern analysis could not distinguish between HCTS and congenital cases due to similar mechanical patterns. The remaining six contrasts in Figures 3.5 - 3.10 showed a variable degree of group separation. Figure 4 presents receiver operating characteristic curves for the SVM models trained with the limited (2D) and the expanded feature space (20D). The AUROC was 0.77 for the 20D feature space (greater than chance with P<0.01, permutation test) in comparison to 0.66 using the 2D feature space (P<0.05). Accuracy of the 20D space was 72% compared to 66% for the 2D space, DOR was 6.50 compared to 1.06, PPV was 0.91 compared to 0.80, and NPV was 0.40 compared to 0.21. The differences in the DOR and the PPV between 20D and 2D spaces were statistically significant with P<0.05 and the difference in accuracy approached the level of significance with P=0.06 based on permutation tests.DISCUSSION
Predicting the outcome of shunt surgery is a challenging task. Spinal tap tests are commonly used for prediction with high positive predictive values but low negative predictive values12. In this study, we presented a machine learning approach based on MRE for prognostic of surgery outcomes. Future work including a larger number of patients in each NPH subgroup and with clinical follow-up after shunt placement may improve pattern score estimation and the classifier training.CONCLUSION
Predicting shunt efficacy in NPH is clinically important. In this study, we demonstrated that a more detailed summary of the MRE result contains clinically useful information for predicting surgical outcomes in NPH and merits further investigation.Acknowledgements
This research was supported by the National Institute of Health grant U01 EB024450, R37 EB001981, and R01 AG076636. We also thank Dr. Bradley D. Bolster and Dr. Stephan Kannengiesser of Siemens Healthcare for providing the MRE pulse sequence on that platform.References
[1] J. Graff-Radford et al., "Cerebrospinal fluid dynamics disorders," Relationship to Alzheimer biomarkers and cognition, vol. 93, no. 24, pp. e2237-e2246, 2019, doi: 10.1212/wnl.0000000000008616
[2] S. Hakim, "Some observations on csf pressure: hydrocephalic syndrome in adults with “normal” csf pressure," Bogota: Javeriana University School of Medicine, 1954.
[3] S. Hakim and R. D. Adams, "The special clinical problem of symptomatic hydrocephalus with normal cerebrospinal fluid pressure: Observations on cerebrospinal fluid hydrodynamics," Journal of the Neurological Sciences, vol. 2, no. 4, pp. 307-327, 1965/07/01/ 1965, doi: 10.1016/0022-510X(65)90016-X.
[4] M. B. Wallenstein and G. M. McKhann, 2nd, "Salomón Hakim and the discovery of normal-pressure hydrocephalus," (in eng), Neurosurgery, vol. 67, no. 1, pp. 155-9; discussion 159, Jul 2010, doi: 10.1227/01.neu.0000370058.12120.0e.
[5] A. K. Toma, M. C. Papadopoulos, S. Stapleton, N. D. Kitchen, and L. D. Watkins, "Systematic review of the outcome of shunt surgery in idiopathic normal-pressure hydrocephalus," (in eng), Acta Neurochir (Wien), vol. 155, no. 10, pp. 1977-80, Oct 2013, doi: 10.1007/s00701-013-1835-5.
[6] E. M. Wu et al., "Ventriculoperitoneal Shunt Outcomes of Normal Pressure Hydrocephalus: A Case Series of 116 Patients," (in eng), Cureus, vol. 11, no. 3, p. e4170, Mar 4 2019, doi: 10.7759/cureus.4170.
[7] H. Kitagaki, E. Mori, K. Ishii, S. Yamaji, N. Hirono, and T. Imamura, "CSF spaces in idiopathic normal pressure hydrocephalus: morphology and volumetry," (in eng), AJNR Am J Neuroradiol, vol. 19, no. 7, pp. 1277-84, Aug 1998.
[8] A. Mládek et al., "Prediction of Shunt Responsiveness in Suspected Patients With Normal Pressure Hydrocephalus Using the Lumbar Infusion Test: A Machine Learning Approach," (in eng), Neurosurgery, vol. 90, no. 4, pp. 407-418, Apr 1 2022, doi: 10.1227/neu.0000000000001838.
[9] J. M. Scott et al., "Impact of material homogeneity assumption on cortical stiffness estimates by MR elastography," (in eng), Magn Reson Med, vol. 88, no. 2, pp. 916-929, Aug 2022, doi: 10.1002/mrm.29226.
[10] J. Ashburner and K. J. Friston, "Unified segmentation," (in eng), Neuroimage, vol. 26, no. 3, pp. 839-51, Jul 1 2005, doi: 10.1016/j.neuroimage.2005.02.018.
[11] M. C. Murphy et al., "Identification of Normal Pressure Hydrocephalus by Disease-Specific Patterns of Brain Stiffness and Damping Ratio," (in eng), Invest Radiol, vol. 55, no. 4, pp. 200-208, Apr 2020, doi: 10.1097/rli.0000000000000630.
[12] M. Mihalj, K. Dolić, K. Kolić, and V. Ledenko, "CSF tap test - Obsolete or appropriate test for predicting shunt responsiveness? A systemic review," (in eng), J Neurol Sci, vol. 362, pp. 78-84, Mar 15 2016, doi: 10.1016/j.jns.2016.01.028.
Figures