4786
Broadband Motion Detection with Wavelet MRE: Validation Study in Phantom and in vivo1Radiology, Mayo Clinic, Rochester, MN, United States
Synopsis
Keywords: Elastography, Elastography, Transient MRE, Wavelet, Brain trauma, broadband motion
Motivation: To test wavelet magnetic resonance elastography (MRE), a promising new technique, on its efficiency in detecting broadband tissue motion.
Goal(s): Evaluate the efficiency and reproducibility of broadband motion detection using wavelet MRE.
Approach: Transient motion in phantoms was reconstructed using both the inverse wavelet transform and standard deconvolution using MRE with various MEG lengths. The estimated displacements were compared. The reproducibility of brain transient motion measurements was assessed in vivo.
Results: Wavelet MRE demonstrated high efficiency and reproducibility for broadband motion detection. These findings suggest that wavelet MRE is a promising technique in brain trauma study.
Impact: Wavelet magnetic resonance elastography is developed to detect broadband motion more accurately and efficiently and could be particularly useful in detecting transient motion during brain impact. This study aims to validate its efficacy and assess its repeatability.
Introduction
Wavelet MRE was developed as a more efficient approach for detecting broadband motion1 using Haar wavelet-based motion-encoding gradients2-7. Previous studies have shown that wavelet MRE results were consistent with those of standard MRE8. Furthermore, a volunteer study highlighted its potential application in studying repetitive head impacts9. In this study, we evaluated its efficiency in broadband motion detection and its reproducibility in measuring transient brain motion.Methods
Phantom StudyMRE images were acquired with a phantom in a 3T clinical scanner (Signa Premier, GE) with motion-encoding gradient (MEG) frequencies from 20-200Hz. Transient motion was generated with one 100-Hz cycle using a surface driver (Fig.1a). 80 phase offsets were acquired for each MEG with a 2.5-ms trigger delay between offsets, resulting in a 200-ms sampling duration. Displacement was estimated with: (1) the inverse Haar transform from selected phase offsets across multiple MEGs (Fig.1b)1; and (2) deconvolution with the applied MEG10.
Displacement values were convolved with each MEG profile to reproduce the MRE phase difference information that should be generated by the corresponding MEG. Within a specified ROI, the reproduced phase differences from all voxels were combined and cross-correlated with the acquired phase difference. Ideally, the reproduced phase difference should match the acquired phase difference for each MEG. If a motion frequency range detected by a given MEG is not captured in the displacement measurement, there will be a mismatch. The number of ‘good matches’ was used as a metric for motion detection accuracy. High efficiency was defined as more or the same ‘good match’ with less phase offsets (i.e., shorter scan time).
Volunteer Study
A healthy volunteer was scanned twice (one month apart) in a 3T clinical scanner (MAGNETOM Prisma, Siemens) using wavelet MRE1. One cycle of 90-Hz motion was applied from the back of the head. Bipolar MEGs of 50, 100, and 200Hz formed a Haar series. Sagittal images were acquired at 3x3x3mm3. The motion sampling duration was 100ms. Displacement vectors within the brain were fitted to a rigid-body model11. Maximal principal strain (MPS) was estimated using the 2D strain tensors.
Results
Phantom StudyDisplacements were calculated from the phase images (Fig.1c) using both methods (Fig.2a&b). Taking one voxel as an example (Fig.2c), Figure 2d-2g show its displacement and the reproduced phase difference for a 100-Hz MEG. The inverse Haar calculated displacement exhibits a higher correlation (r2: 0.94 vs. 0.81), indicating a better match for this voxel. When the whole ROI was combined (Fig.3a), the inverse Haar consistently achieved higher r2 (Fig.3b). We set a threshold of r2>0.9 as a ‘good match’. Using 31 phase offsets, the inverse Haar outperformed most deconvolutions, and notably outperforming the deconvolution with 40 phase offsets. Furthermore, inverse Haar with 39 phase offsets outperformed all deconvolutions.
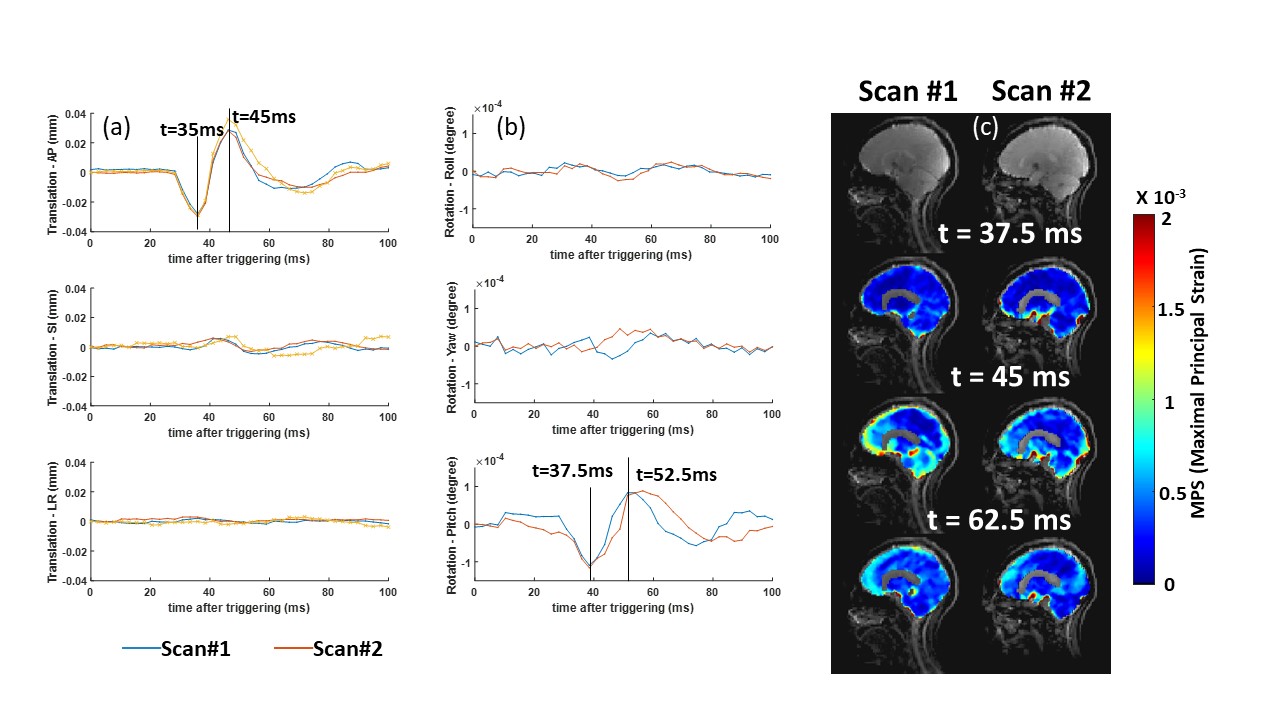
Volunteer study
scans exhibit consistent motion patterns (Fig.4 &5). Specifically, in the AP translation and the pitch rotational direction, distinct peaks are evident between 35-45ms for translation and slightly later at 37.5-52.5ms for rotation. This indicates that the initial impact predominantly induces translational motion, followed by rotational movements. Other axes show modest fluctuations towards the baseline. MPS maps highlighted the regions with the most postimpact deformation, showing the most pronounced deformation peaking at 4ms, notably near the cortical surface and cerebellum. This aligns with MPS findings from neck extension studies using MR tagging12. The consistency between the two scans demonstrates the repeatability of this technique, suggesting that the observed brain movements and deformations are consistent responses to transient impacts, rather than random events.
Discussion
For the 20-Hz MRE, r2 was notably low, likely due to the low amplitude at the low end of the motion spectrum, leading to low SNR in the phase images. Given that wavelet MRE combines multiple MEG lengths to cover a wide frequency spectrum, it is expected that inverse Haar transform would outperform deconvolution with fewer phase offsets (which translates to reduced scan times). For the volunteer study, future research will investigate individual variability across volunteers to provide a more comprehensive understanding of biomechanical responses of the brain to impacts. Since the current acquisition is 2D, there is a potential area for future advancements with the development of a 3D version of the technique.Conclusion
Wavelet MRE is more efficient than standard MRE in detecting broadband motion. The in vivo repeatability data further demonstrates its reliability. This method holds promise for studying brain biomechanics in the context of brain trauma.Acknowledgements
This work is supported by NIH grants (R01 EB001981 and R01 NS113760). We also would like to acknowledge Dr. Bradley D. Bolster and Dr. Stephan Kannengiesser at Siemens Healthcare for their software.References
1. Le, Y., et al. Joint Annual Meeting ISMRM-ESMRMB; London, England, UK.
2. McCracken, P. J., et al. Magn Reson Med. 2005;53(3):628-39. Epub 2005/02/22.
3. Souchon, R., et al. Magn Reson Med. 2008;60(4):871-81. Epub 2008/09/26.
4. Hofstetter, L. W., et al. Magn Reson Med. 2019;81(5):3153-67. Epub 2019/01/22.
5. Hofstetter, L. W., et al. Phys Med Biol. 2020. Epub 2020/12/23.
6. Smith, D. R., et al. J Biomech Eng-T Asme. 2020;142(7).
7. Shahryari, M., et al. Magnetic Resonance in Medicine. 2021;85(4):1962-73.
8. Le, Y., et al. Proc Intl Soc Mag Reson Med; Toronto.
9. Le, Y., et al. Proc Intl Soc Mag Reson Med 31 (2023); Toronto.
10. McCracken, P. J. Transient-based Magnetic Resonance Elastography of the Brain: Biomedical Engineering--Mayo Clinic College of Medicine; 2005.
11. Yin, Z., et al. Magn Reson Med. 2018;80(6):2573-85. Epub 20180517.
12. Knutsen, A. K., et al. Brain Multiphys. 2020;1. Epub 20200903.
Figures