4782
Preliminary 4D-Flow cardiac MRI assessment of ascending aorta in patients with sigmoid hypertrophic cardiomyopathy1Radiology, Mayo Clinic, Rochester, MN, United States
Synopsis
Keywords: Flow, Quantitative Imaging
Motivation: To establish accurate measures in predicting prognosis in patients with sigmoid HCM from their 4D-flow-derived hemodynamics.
Goal(s): We explored the association between aortic stiffness and sigmoid HCM through measuring peak wall shear stress in the three ascending aorta segments: proximal, mid, and descending.
Approach: We recruited 40 subjects and divided them into control and affected groups and then compared ascending aorta 4D flow hemodynamics.
Results: Maximum diameters and peak flow velocity of ascending aorta were higher in the affected group.
Impact: Assessing aortic hemodynamics with 4D Flow CMR in patients with hypertrophic cardiomyopathy will help us understand the relationship between aortic stiffness and left ventricular hypertrophy, which is associated with outcomes in hypertrophic cardiomyopathy patients.
Introduction
Higher aortic stiffness has been reported in adults and children with hypertrophic cardiomyopathy (HCM). The risk of death in patients with HCM is related to the degree of left ventricular hypertrophy. The relationship between aortic stiffening and the degree of left ventricular hypertrophy in patients with HCM remains incompletely understood but is believed to contribute to increased left ventricular hypertrophy. In addition, increased aortic stiffness may influence exercise capacity and disease progression.(1) In this study, we measured aortic wall shear stress in patients with sigmoid subtype of HCM and healthy control participants using 4D flow cardiovascular magnetic resonance (CMR).Methods(2)
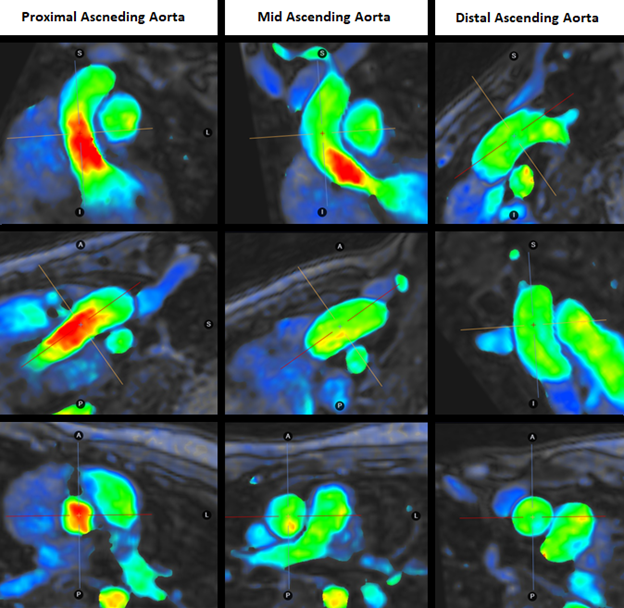
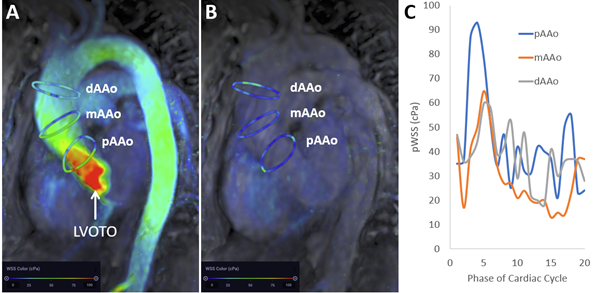
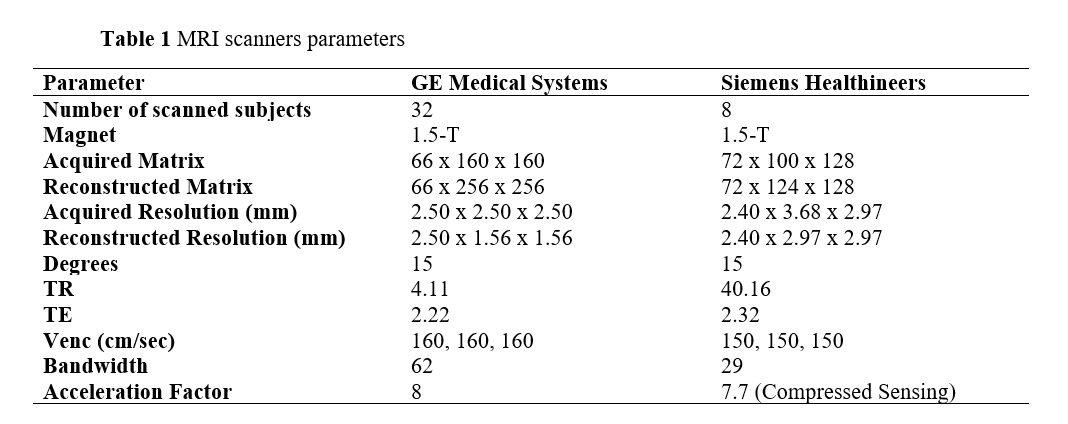
This retrospective, IRB-approved study included CMR data from 20 patients with sigmoid hypertrophic cardiomyopathy (HCM) and 20 healthy control subjects. The need for individual informed consent was waived. Patients with sigmoid HCM were scanned as part of their clinical routine, with 4D Flow CMR acquired for quantification of mitral regurgitation and left ventricular outflow tract velocities. Healthy volunteers were identified from prospective studies that included 4D Flow CMR and whole heart CINE imaging. CMR was performed on two clinical 1.5T MRI scanners (MR450w, GE Healthcare and Area, Siemens). Whole heart CINE balanced steady-state free precession (bSSFP) imaging was performed according to SCMR guidelines with short-axis images covering the entire left ventricle. Short-axis CINE bSSFP was used for quantification of left ventricle size and ejection fraction. 4D Flow CMR parameters are summarized in Table 1. Correction, including eddy current correction and anti-aliasing, were applied for image optimization. 4D flow CMR analysis was conducted using commercially available software (Arterys, version 31.0.2). Hemodynamic parameters measured in each subject included peak wall shear stress (pWSS), peak flow velocity, and maximum vessel diameter across 3 segments of the ascending aorta: proximal (pAAO), mid (mAAO), and distal (dAAO). Statistical analysis was executed using IBM SPSS Statistics software (version 28.0) with p-value of less than 0.05 denoting statistical significance. Continuous variables were expressed as mean and median with interquartile range (IQR) for age, left ventricular ejection fraction (LVEF), along with maximum diameter, peak flow velocity, and pWSS for each aortic segment. These variables were then compared using the Mann-Whitney U test, given their non-equal distribution.Results
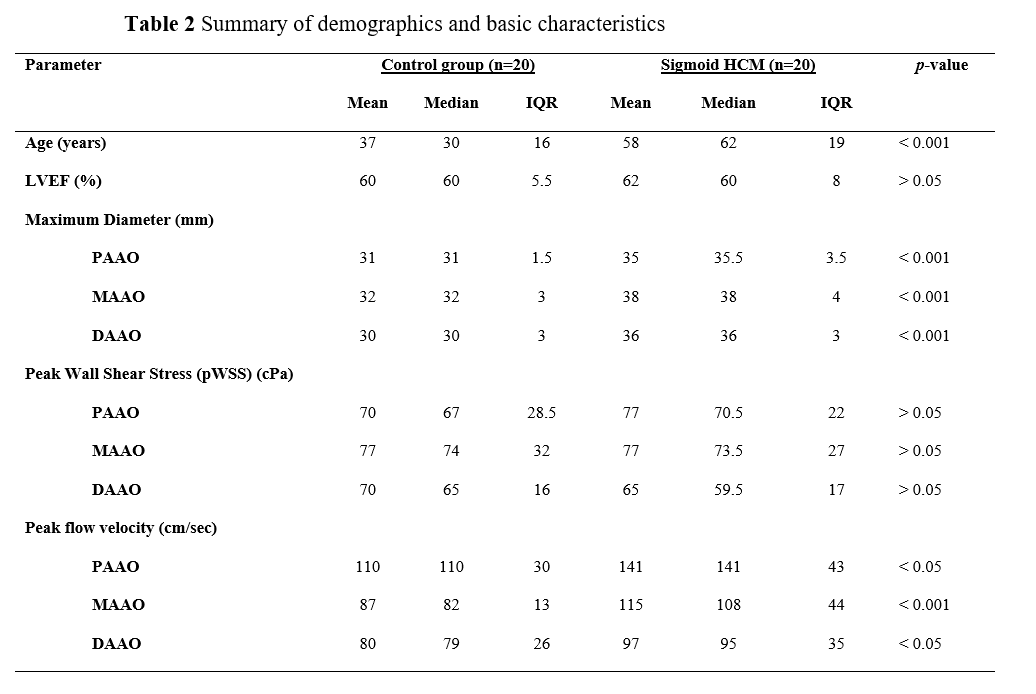
The median age was 29.5 years (IQR = 28-44) for the control group and 62 (IQR = 50-68) for the sigmoid HCM group. Eight female subjects were present in each group. Median LVEF was 60% for both control (IQR = 57-62) and the sigmoid HCM group (IQR = 58-66). Results are summarized in Table 2. Significant differences (p < 0.05) were present for age, peak flow velocity, and maximum diameter across the 3 segments of ascending aorta: pAAO, mAAO, and dAAO. Both groups had similar mean and median of pWSS. However, peak flow velocity and maximum vessel diameter were larger in subjects with sigmoid hypertrophic cardiomyopathy.Discussion
In this study we measured aorta diameter, peak velocity, and peak wall shear stress in patients with sigmoid subtype of HCM and healthy controls using 4D flow CMR. Peak flow velocity and maximum vessel diameter of the ascending aorta in patients with sigmoid subtype of HCM were significantly greater than in healthy control subjects. There was no significant difference in pWSS between groups, which could be related to differences in the age between the groups.(3) Further studies will be conducted to assess changes in aorta hemodynamics using 4D Flow CMR in other subtypes of HCM and to explore the relationships between aortic hemodynamics and left ventricular hypertrophy and clinical complications in patients with HCM.Conclusion
Patients with sigmoid HCM have an increased diameter of the ascending aorta and higher peak flow velocity yet maintain a normal peak wall shear stress. These hemodynamic parameters may serve as precise markers for assessing disease outcome and progression in patients with HCM.Acknowledgements
No acknowledgement found.References
1. Austin BA, Popovic ZB, Kwon DH, et al. Aortic stiffness independently predicts exercise capacity in hypertrophic cardiomyopathy: a multimodality imaging study. Heart 2010;96(16):1303-1310.
2. Bissell MM, Raimondi F, Ait Ali L, et al. 4D Flow cardiovascular magnetic resonance consensus statement: 2023 update. Journal of Cardiovascular Magnetic Resonance 2023;25(1).
3. Callaghan FM, Grieve SM. Normal patterns of thoracic aortic wall shear stress measured using four-dimensional flow MRI in a large population. Am J Physiol Heart Circ Physiol 2018;315(5):H1174-H1181.
Figures