4780
Dynamic 2D phase-contrast of the tricuspid valvular flow with automated valve-tracking: patient case studies1Yale University School of Medicine, New Haven, CT, United States, 2Université de Paris, Cardiovascular Research Center, INSERM, Paris, France, 3Biomedical Engineering, Yale University, New Haven, CT, United States, 4Yale School of Medicine, New Haven, CT, United States
Synopsis
Keywords: Flow, Valves, regurgitation
Motivation: MRI is not capable of measuring tricuspid regurgitant jets, required for diastolic function evaluation.
Goal(s): Using a dynamic slice plane which tracked the tricuspid valve, we studied patients with suspected tricuspid regurgitation.
Approach: The valve-tracking phase-contrast sequence used deep learning to automatically prescribe a phase-dependent slice plane.
Results: Tricuspid regurgitation was measured and tricuspid regurgitant jets could be visualized in patients.
Impact: A new automated 2D valve-tracking phase-contrast approach permits visualization of tricuspid regurgitant jets. This will enable evaluation of diastolic function by MRI.
Introduction
Tricuspid valvular regurgitation with fast regurgitant jets is often due to elevated right ventricle (RV) pressure, commonly seen in pulmonary hypertension (PH) (1) and patients with diastolic dysfunction, where tricuspid regurgitant velocity is one of 4 criteria used to identify dysfunction (along with LA volume, E/e’ and E/A) (2). Thus, evaluation of tricuspid regurgitant velocity is of great clinical import. Transthoracic echocardiography (3) is used for measuring regurgitant jets. Direct valve flow evaluation by cardiac MRI is not feasible due to valvular displacement during the cardiac cycle; even more so for the highly dynamic (translating and rotating) tricuspid valve (4). Therefore, cardiac MRI is not capable of measuring tricuspid regurgitant jets with standard techniques. 4D Flow methods have had success in tricuspid regurgitant velocity evaluation, using many minutes of scan time, because retrospective valve tracking can be employed (5,6). Prospective valve-tracking methods have also been employed to acquire 2D phase-contrast (PC) with a dynamic slice plane prescription that changes over the cardiac cycle (7,8). Such methods have recently been greatly improved, using automatic tracking in 2- and 4-chamber LV or RV cines to determine phase-dependent slice translation and rotation, for prospective valve-tracking PC (9) (10). This can be accomplished with both modern feature-tracking (11), or even most recently using a deep learning framework (MVnet or TVnet(12 ,13)) for the mitral and tricuspid valves) to generate a dynamic slice prescription. In this study, we utilize the deep learning framework TVnet to determine a dynamic prospective slice-prescription for valve-tracking phase-contrast. We studied five patients with suspected tricuspid regurgitation, to evaluate regurgitation and visualize jets.Methods
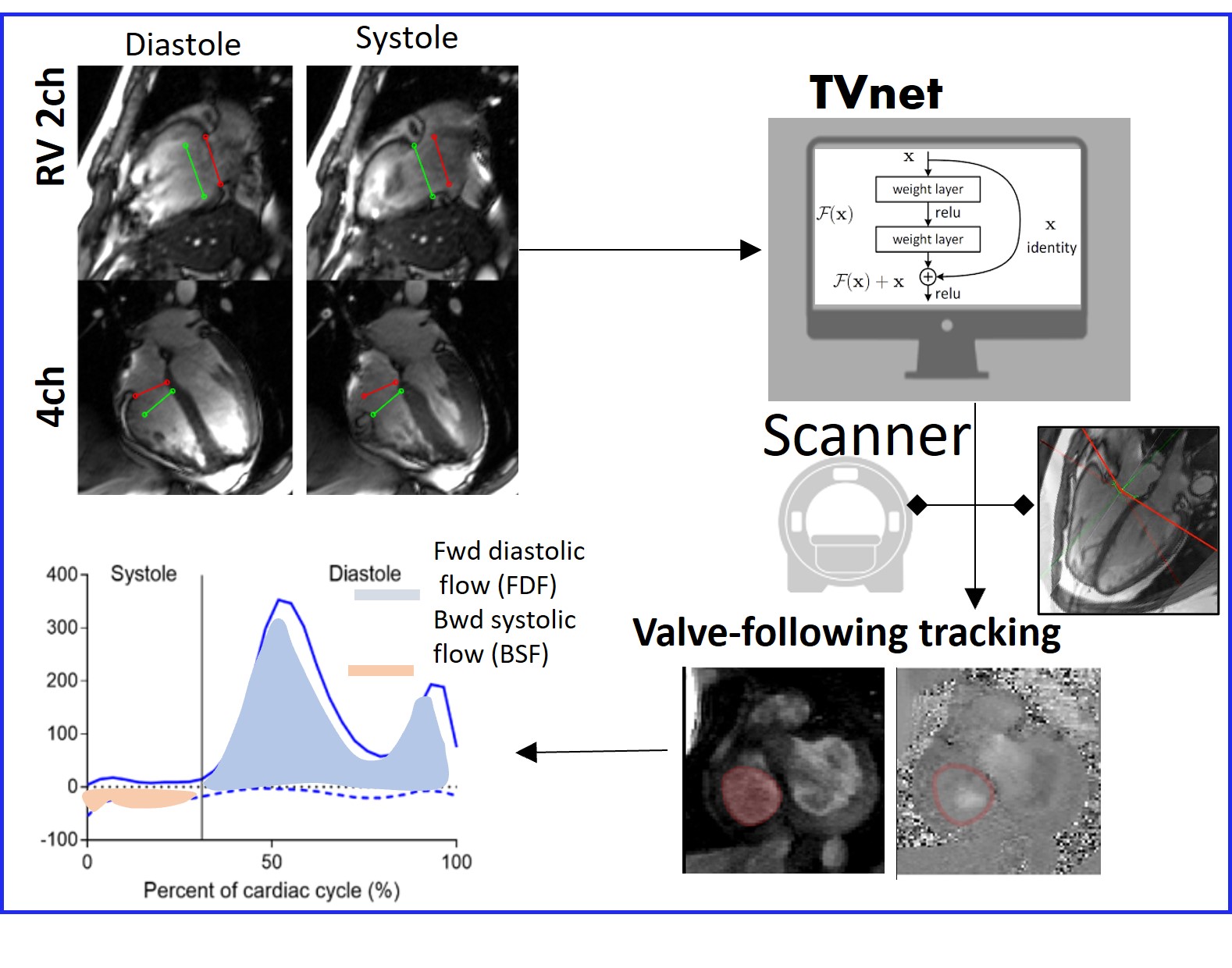
Methods. Figure 1 shows the workflow for valve-tracking PC. First, RV 2- and 4-chamber long-axis cines are acquired and exported to an offline computer for automated tracking of the valve-insertion points, using TVnet. This automated tracking produces the center point of the TV plane and the normal to the TV plane for each time-point in the cardiac cycle. This is automatically input to the customized MRI sequence via a USB device. During the breath-hold, the slice geometry is updated by the sequence at each cardiac phase to match the valve position and orientation. Five patients (42 ±8 years old, 1 F) undergoing a clinically indicated cardiac MR (1.5T Siemens, Erlangen, Germany) were prospectively enrolled. The study was approved by our local IRB and all subjects provided written informed signed consent. Research imaging included a 2D PC acquisition with dynamic slice plane, using automated valve-tracking by TVnet. The 2D-PC scan protocol was: FOV: 380mm, acquisition matrix=256x208, repetition time=5.3ms, echo time=3.4ms, flip angle=15°, voxel size= 1.48x1.48x5-6 mm3, GRAPPA=2, partial Fourier 6/8, through-plane flow-encoding with a VENC of 150cm/s to 400cm/s (higher if high velocity jets were expected); temporal resolution of 42ms. Standard planimetry of the cine stack and aortic PC were used to compare resultant SV values, depending on the patient’s protocol. Flow analysis was performed using Segment software (14), including eddy current compensation, using cardiac phase-dependent ROIs to identify static tissue. The flow velocities were corrected for relative motion of the valve (15). All patients had a recent echocardiography.Results
This method was validated in a study of 9 healthy controls (9) without expected regurgitation, where the forward valvular flow agreed strongly with RVSV (r=0.94, Bland-Altman limits of agreement 0.2 ± 10.4mls) using PC with a dynamic slice plane, and agreement was superior to a static slice plane PC (r=0.84, Bland-Altman limits of agreement -10.6 ± 16.1mls).Figure 2 (Patient A) shows a patient with a short lived jet, where valve-tracking PC with a 330cm/s VENC was obtained. Using the indirect method (RV SV-aortic flow), the patient had 23 mls of regurgitation. By valvular flow, the patient had 26 mls of regurgitant flow. This shows reasonable agreement between the indirect and direct methods (23 vs. 26mls). Echocardiography depicted a short lived jet, with peak velocities of ~150 cm/s, which was not observable by MRI. The tracking results in apparent motion of the chest wall, but the slice plane was usually maintained at the tricuspid valve.
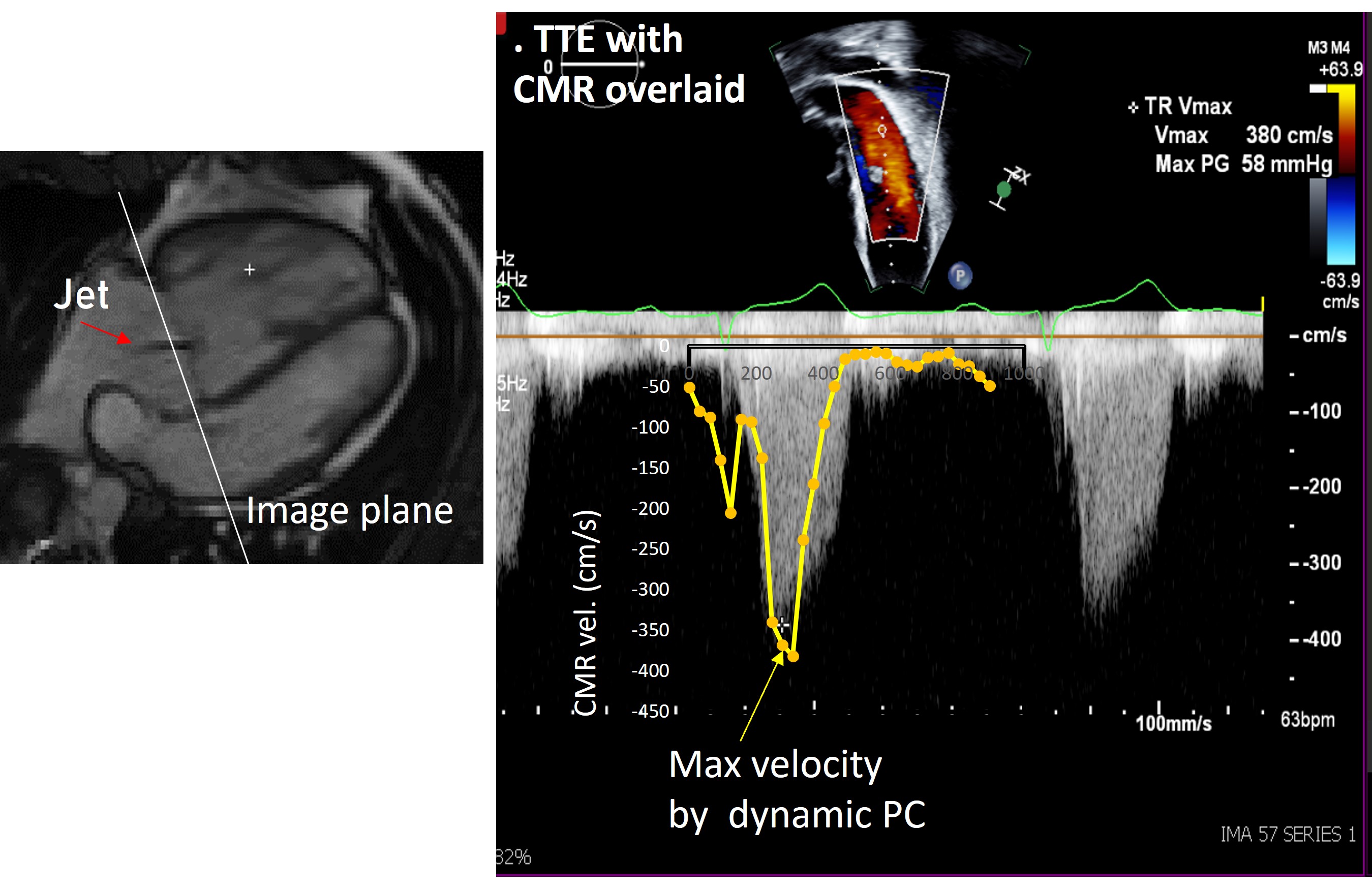
Figure 3 (Patient B) shows a patient with a high velocity jet, evident on the velocity images in systole. The tracking was excellent, with the slice plane just above the valve in all cardiac phases. Comparison to echocardiography shows excellent agreement of dynamic valve-tracking PC, regarding peak jet velocity (Figure 4). However, a dynamic slice plane just below the valve revealed much less regurgitation, indicating that slice plane is critical.
Conclusions
Tricuspid regurgitant jet velocity evaluation is possible with 2D valve-tracking PC.Acknowledgements
No acknowledgement found.References
1. Mutlak D, Aronson D, Lessick J, Reisner SA, Dabbah S, Agmon Y. Functional Tricuspid Regurgitation in Patients With Pulmonary Hypertension Is Pulmonary Artery Pressure the Only Determinant of Regurgitation Severity? Chest 2009;135(1):115-121.
2. Nagueh SF, Smiseth OA, Appleton CP, Byrd BF, Dokainish H, Edvardsen T, Flachskampf FA, Gillebert TC, Klein AL, Lancellotti P, Marino P, Oh JK, Popescu BA, Waggoner AD, Echocardiography AS, Imaging EAC. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur Heart J-Card Img 2016;17(12):1321-1360.
3. Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP, Gentile F, Jneid H, Krieger EV, Mack M, McLeod C, O'Gara PT, Rigolin VH, Sundt TM, Thompson A, Toly C. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2021;143(5):e72-e227.
4. Ton-Nu TT, Levine RA, Handschumacher MD, Dorer DJ, Yosefy C, Fan DL, Hua LQ, Jiang L, Hung J. Geometric determinants of functional tricuspid regurgitation - Insights from 3-dimensional echocardiography. Circulation 2006;114(2):143-149.
5. Feneis JF, Kyubwa E, Atianzar K, Cheng JY, Alley MT, Vasanawala SS, Demaria AN, Hsiao A. 4D Flow MRI Quantification of Mitral and Tricuspid Regurgitation: Reproducibility and Consistency Relative to Conventional MRI. J Magn Reson Imaging 2018;48(4):1147-1158.
6. Driessen MMP, Schings MA, Sieswerda GT, Doevendans PA, Hulzebos EH, Post MC, Snijder RJ, Westenberg JJM, van Dijk APJ, Meijboom FJ, Leiner T. Tricuspid flow and regurgitation in congenital heart disease and pulmonary hypertension: comparison of 4D flow cardiovascular magnetic resonance and echocardiography. J Cardiovasc Magn Reson 2018;20(1):5. 7. Kozerke S, Schwitter J, Pedersen EM, Boesiger P. Aortic and mitral regurgitation: Quantification using moving slice velocity mapping. J Magn Reson Imaging 2001;14(2):106-112.
8. Kozerke S, Scheidegger MB, Pedersen EM, Boesiger P. Heart motion adapted cine phase-contrast flow measurements through the aortic valve. Magn Reson Med 1999;42(5):970-978. 9. Lamy J, Xiang J, Seemann F, Gonzales R, Huber S, Steele J, Heiberg E, Peters D. 2.5D Flow MRI: 2D phase-contrast of the tricuspid valvular flow with automated valve-tracking ISMRM (accepted as oral abstract) 2023
10. Seemann F, Heiberg E, Carlsson M, Gonzales RA, Baldassarre LA, Qiu M, Peters DC. Valvular imaging in the era of feature-tracking: A slice-following cardiac MR sequence to measure mitral flow. J Magn Reson Imaging 2019. 11. Seemann F, Pahlm U, Steding-Ehrenborg K, Ostenfeld E, Erlinge D, Dubois-Rande JL, Jensen SE, Atar D, Arheden H, Carlsson M, Heiberg E. Time-resolved tracking of the atrioventricular plane displacement in Cardiovascular Magnetic Resonance (CMR) images. Bmc Med Imaging 2017;17. 12. Gonzales R, Lamy J, Thomas K, Zhang Q, Shanmuganathan M, Heiberg E, Ferreira V, Piechnik S, Peters DC. TVnet: automated global analysis of tricuspid valve plane motion in CMR long-axis cines with residual neural networks. European Heart Journal-Cardiovascular Imaging, 23(S2), pp36-37 2022.
13. Gonzales R, Lamy J, Seemann F, Arvidsson P, Murray V, Heiberg E, Peters D. TVnet: Automated Time-Resolved Tracking of the Tricuspid Valve Plane in Long-Axis Cine Images with a Dual Stage Deep Learning Pipeline. In International Conference on Medical Image Computing and Computer-Assisted Intervention (MICCAI) (pp 567-576) Springer, Cham 2021.
14. Heiberg E, Sjogren J, Ugander M, Carlsson M, Engblom H, Arheden H. Design and validation of Segment--freely available software for cardiovascular image analysis. Bmc Med Imaging 2010;10:1. 15. Kayser HWM, Stoel BC, vanderWall EE, vanderGeest RJ, deRoos A. MR velocity mapping of tricuspid flow: Correction for through-plane motion. J Magn Reson Imaging 1997;7(4):669-673.
Figures