4779
Accelerated Phase Contrast MRI with Use of K-Space Restoration and Resolution Enhancement Generative Adversarial Neural Network1Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, MA, United States
Synopsis
Keywords: Flow, Cardiovascular
Motivation: Phase-contrast (PC) MRI evaluates blood flow in cardiovascular disease. However, the prolonged scan times limit its efficiency.
Goal(s): We sought to develop a highly accelerated PC technique based on omitting high-frequency k-space regions along the phase encoding direction.
Approach: A deep learning k-space restoration and enhancement strategy for training (KREST) was developed to improve resolution while maintaining phase information. KREST was trained and tested with PC images from 1600 patients.
Results: In a prospective study of 16 patients, KREST reduced breath-hold time relative to parallel imaging (19 vs 6 s).
Impact: Our k-space restoration and enhancement strategy enables resolution-enhancement while providing k-space data consistency. Deep learning accelerated phase-contrast imaging showed similarly accurate quantification of peak mean velocity to a standardized parallel imaging method.
Introduction
Phase-contrast (PC) MRI is widely used for assessing blood flow in cardiovascular disease. However, most PC sequences require acquisition of velocity compensated and velocity encoded images for each cardiac frame, which results in prolonged scan times and longer breath-holds or reduced spatiotemporal resolution. Resolution-enhancement using a generative adversarial network (GAN) is a promising technique for accelerated imaging based on omitting high-frequency k-space regions along the phase encoding (PE) direction [1]. However, current DL resolution-enhancement models are based on magnitude images only. Enhancement of phase images is challenging since DL models can yield outputs with arbitrary pixel values, resulting in inaccurate measures of blood flow. We propose a deep learning (DL) approach using a k-space restoration and enhancement strategy for training (KREST) to improve resolution while maintaining phase information.Methods
We implemented our KREST methodology for GAN-based resolution enhancement. “High-resolution” ground-truth images are created from fully sampled k-spaces, while the input images come from low-resolution k-spaces that retain only 25-75% of phase-encoding (PE) lines (Fig. 1A). The inputs are channel-concatenated real and imaginary components of low-resolution images, and the outputs are intermediate “edge images” used to generate the outer k-space regions. We ensure data consistency by merging the original center and synthesized outer regions (Fig. 1B). The generator included ten residual blocks of 32 filters (Fig. 2A). The discriminator included six discriminator blocks (Fig. 2B). The network, trained on both velocity compensated and encoded images using image and k-space losses (Fig. 2C), enhances resolution in a single image. Therefore, during inference, PC images are enhanced separately to obtain a resolution-enhanced phase difference image (Fig. 2D).The study included retrospective and prospective components: retrospective data collected from 1600 patients (56 ± 16 years) were used for training and testing (4:1 ratio). Subsequently, we prospectively recruited 16 patients (57 ± 19 years). All patients were undergoing clinical cardiac MRI at 3T.
Retrospective data for training and testing were collected using breath-hold ECG-segmented PC in aortic, pulmonary, mitral, and tricuspid valve views. Imaging parameters included: GRAPPA rate 2, TE/TR = 2.7/4.7 ms, FA = 20 degrees, slice thickness = 6.0 to 7.0 mm, temporal resolution = 33 ms, asymmetric echo = 33%, spatial resolution = 1.9 × 1.9 mm2, and matrix size = 147 ± 6 (144 – 216) × 192. Thus, the ground-truth reference was not “fully sampled” due to asymmetric echo and PE already truncated at ~75%.
We prospectively collected two separate breath-hold ECG-segmented PC scans in aortic view. Imaging parameters included: GRAPPA rate 2, TE/TR = 2.7/4.3 ms, FA = 20 degrees, slice thickness = 8 mm, temporal resolution = 43 ms, resolution 1.9 × 1.9 mm2, matrix = 192 × 192, PE truncation = 80% and 25%, and breath-hold durations = 19 and 6 s. Combined acceleration rates were 2.2-fold and 5.3-fold.
Reconstruction consisted of vendor-provided GRAPPA to create images from 2.2-fold and 5.3-fold undersampled k-space. The 5.3-fold reconstructed images were blurry due to the PE truncation. Thus, our proposed KREST method was applied to enhance the spatial resolution.
Using aortic view scans from 368 patients from the retrospective testing cohort, we generated low-resolution images by keeping 5 to 60% of PE lines. KREST-enhanced images were generated by applying KREST to low-resolution images. KREST-enhanced and ground-truth high-resolution images were compared using peak mean velocity (PMV) and vessel wall sharpness [2]. In the prospective study, sharpness and PMV were assessed in 2.2-fold, 5.5-fold, and 5.3-fold KREST-enhanced images.
Statistics included linear regression, Pearson r, and paired t-test. P-value < 0.05 was significant.
Results
Resolution-enhanced images were successfully generated using KREST (Fig. 3). In the restored k-space, KREST synthesized only up to ~75% of PE lines and had some difficulty in outer k-space regions along readout direction (Fig. 4). This is caused by the asymmetric echo and PE truncation already present in the training data. For retrospective test data with 28% of collected PE lines or more, image sharpness was similar in high-resolution and KREST-enhanced images (2.8, 2.8 ± 0.3; P=0.2), and errors in PMV were < 0.1 cm/s (Fig. 5A). Sharpness and PMV accuracy rapidly deteriorated below 28%. In prospective breath-hold ECG-segmented PC, 5.3-fold KREST-enhanced images showed increased sharpness (2.3 ± 0.2) compared to 5.3-fold (1.1 ± 0.2) but was lower (P < 0.001) than 2.2-fold images (3.1 ± 0.3) (Fig. 5C). There was a strong correlation (r = 0.99) and agreement (slope = 1.00) between 5.3-fold KREST-enhanced and 2.2-fold measures of PMV.Conclusion
We developed and evaluated a DL-based resolution enhancement strategy (KREST) that preserves k-space and phase information, enabling highly accelerated PC imaging.Acknowledgements
This study was supported in part by the American Heart Association Career Development Award and National Institutes of Health.References
[1] Yoon, Siyeop, et al. "Accelerated Cardiac MRI Cine with Use of Resolution Enhancement Generative Adversarial Inline Neural Network." Radiology 307.5 (2023): e222878.
[2] Ahmad, Rizwan, Yu Ding, and Orlando P. Simonetti. "Edge sharpness assessment by parametric modeling: application to magnetic resonance imaging." Concepts in Magnetic Resonance Part A 44.3 (2015): 138-149.
Figures
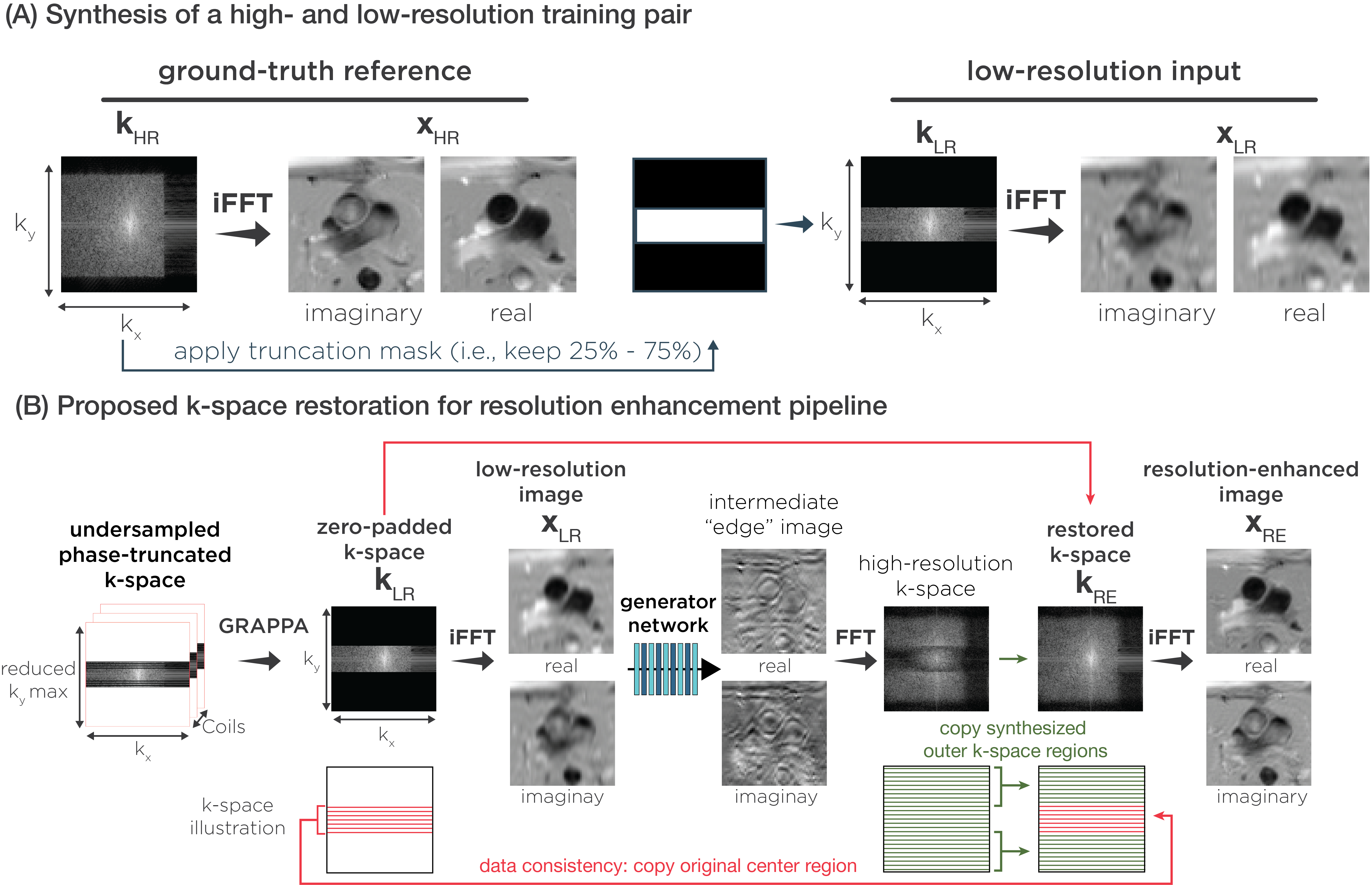
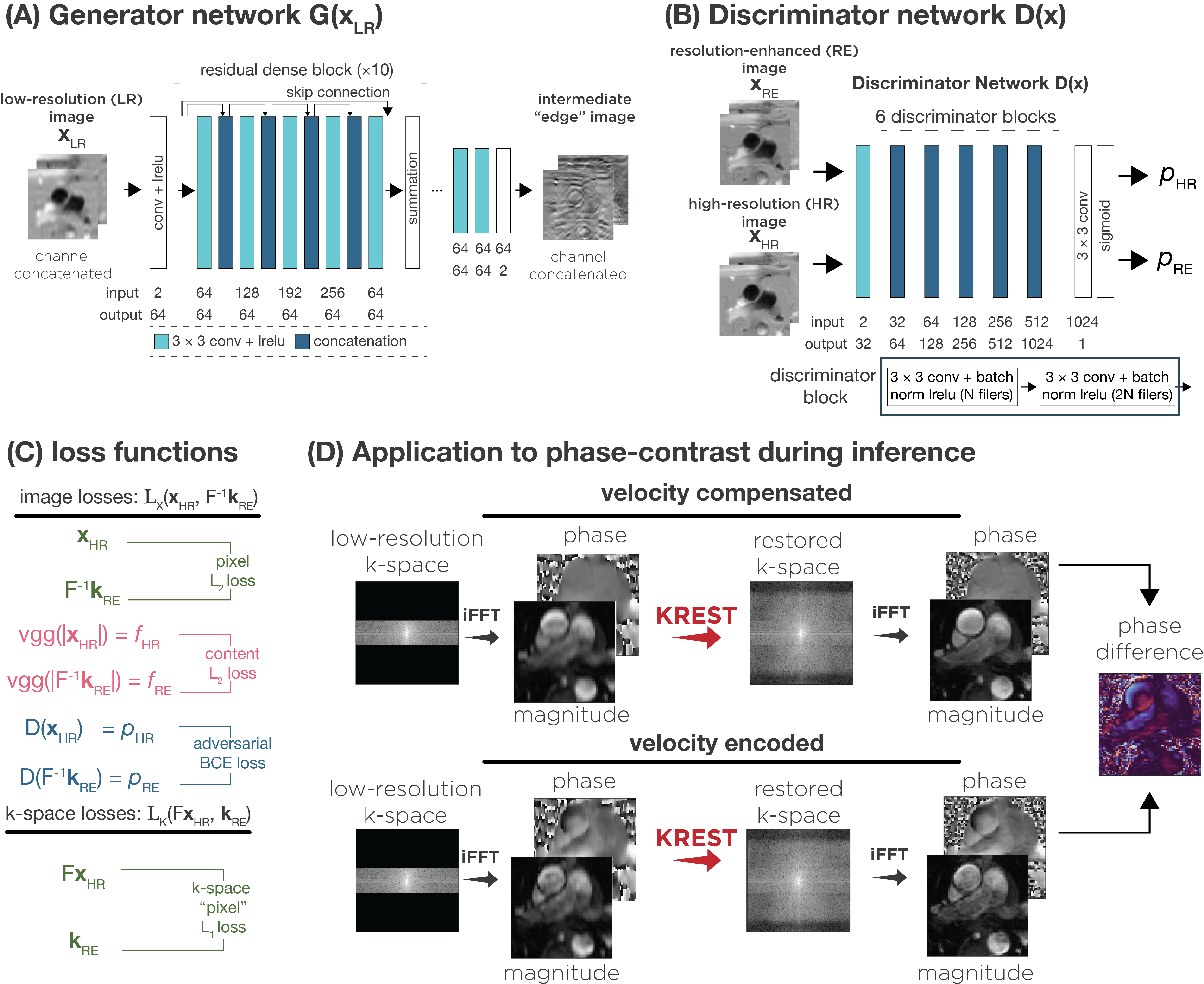
Figure 2. (A) Generator with 10 residual blocks of 32 filters. (B) Discriminator network with 6 discriminator blocks. (C) The final output is the resolution-enhanced k-space kRE. Image and k-space losses are Lx(xHR, F-1kRE), Lk(FxHR, kRE). (D) KREST is based on a single image and is not specific to PC data. Thus, a single network was trained using both velocity compensated and encoded images. During inference, the images are enhanced separately to obtain a resolution-enhanced phase difference image. Magnitude and phase are shown here, but network uses concatenate real and imaginary.
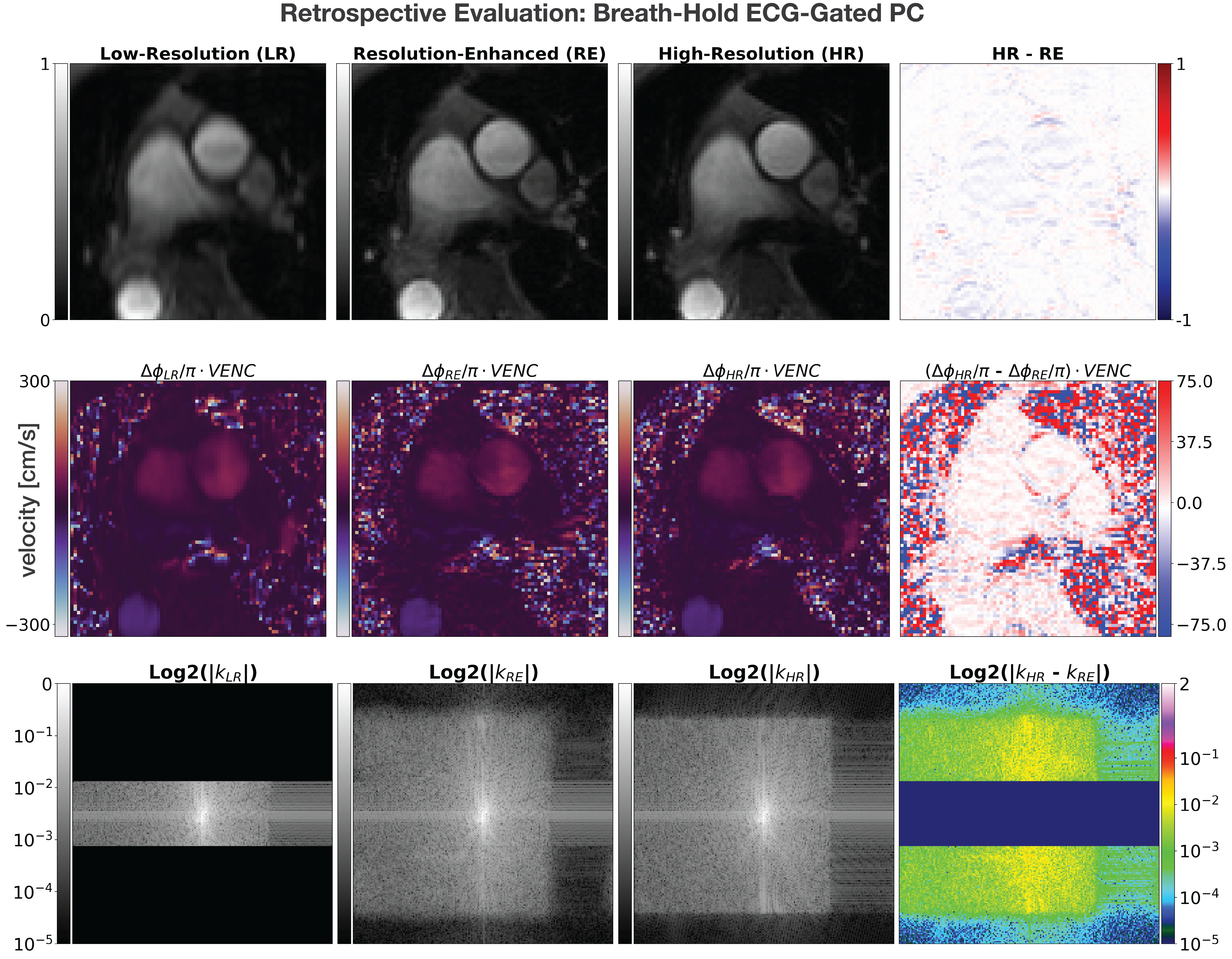
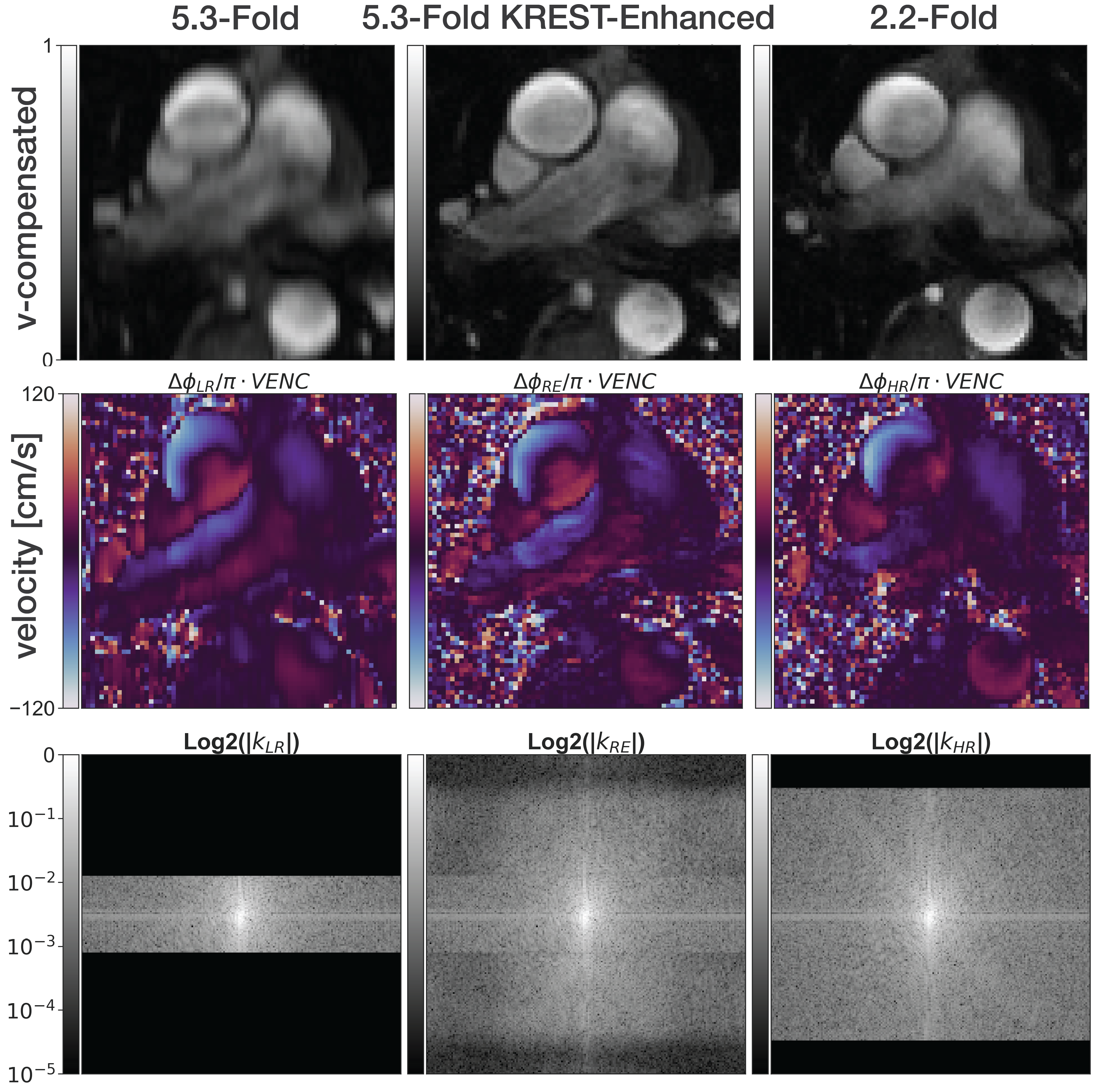
Figure 4. Prospective breath-hold electrocardiogram-gated phase-contrast scan with a 192 × 192 matrix and 1.9 × 1.9 mm2 resolution. Phase-encoding (PE) truncation at 25% (first column) and 80% (third column) resulted in 48 and 154 PE lines. With GRAPPA rate = 2 and ACS lines = 24, total collected lines were 89 and 36, equivalent to 2.2-fold and 5.3-fold acceleration rates. KREST was applied to blurry 5.3-fold images to obtain 5.3-fold KREST-enhanced (2nd column). 1st row: magnitude of velocity-compensated image. 2nd row: aortic blood velocity. 3rd row: k-spaces. Errors in last column.
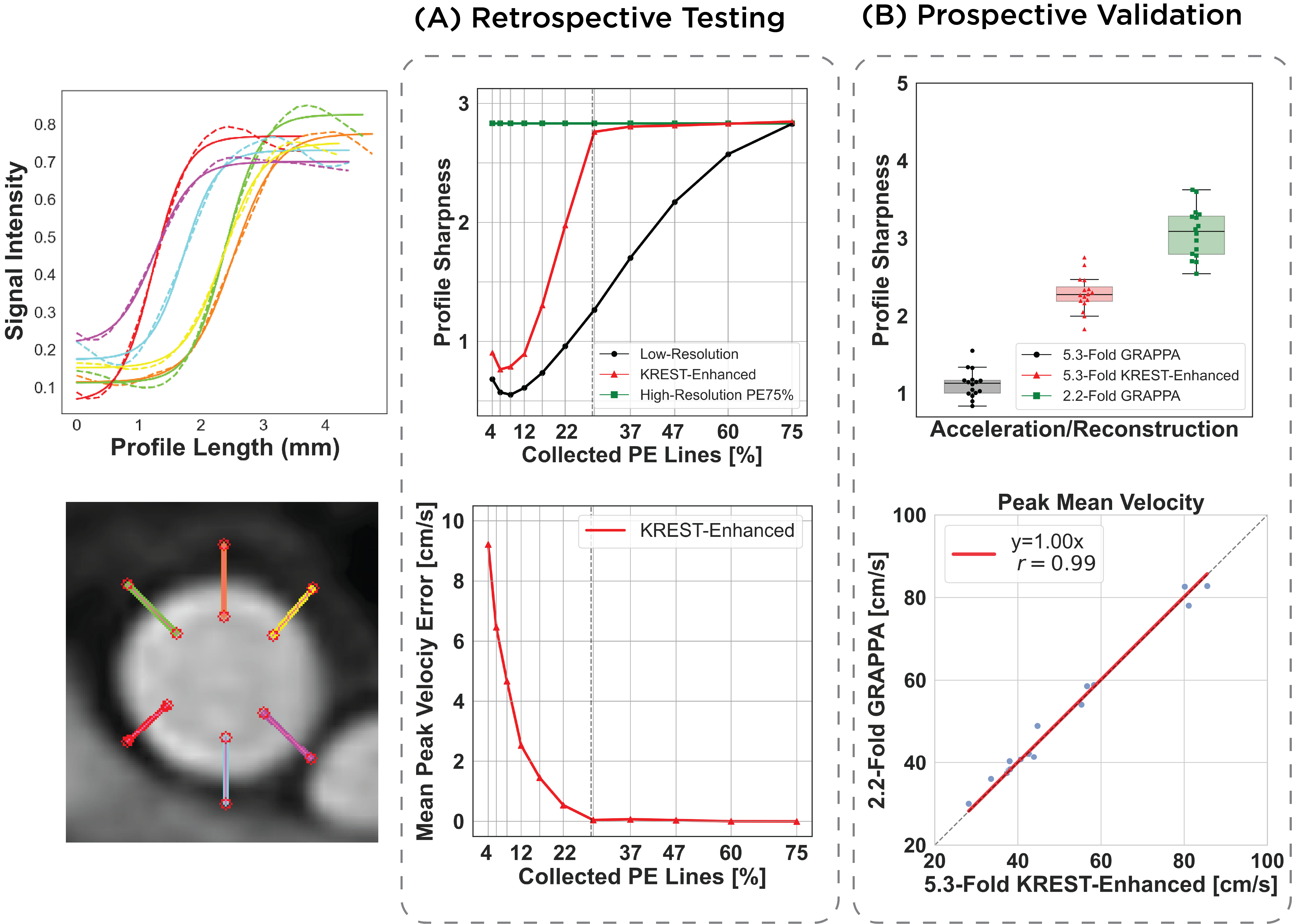
Figure 5. First, the aortic wall vessel was segmented in each cardiac frame. Mean velocity per frame was the average within the segmented region. Profiles were drawn across the wall vessel in the cardiac frame where peak mean velocity (PMV) occurs. Sharpness is the slope of a fitted sigmoid. (A) Sharpness and PMV error as a function of collected phase-encoding (PE) lines in the retrospective test suggest a PE truncation of ~30% is the maximum allowed. (B) 5.3-fold KREST-enhancement improves sharpness and provides accurate PMV measures of in breath-hold ECG PC.