4772
An evaluation of hemodynamic parameters before and after Ross procedure for Unicuspid Aortic Valve (UAV) using 4D flow MRI1Radiology, Northwestern University Feinberg School of Medicine, CHICAGO, IL, United States, 2Cardiac Surgery, Northwestern University Feinberg School of Medicine, CHICAGO, IL, United States
Synopsis
Keywords: Flow, Cardiovascular, Aorta, Aortic Valve, Unicuspid Aortic Valve, Bicuspid Aortic Valve, 4D Flow, 4D Flow MRI
Motivation: Unicuspid Aortic Valve (UAV) is an important subset of Bicuspid Aortic Valve. We identified a need to include wall shear stress in a larger pre- and post-operative cohort of UAV patients.
Goal(s): Our goal was to evaluate the effects of the Ross procedure for UAV patients, specifically evaluating hemodynamic parameters, peak systolic velocity and wall shear stress (WSS), in the ascending aorta (AAo).
Approach: We retrospectively examined these hemodynamic parameters in thirteen patients before and after UAV replacement.
Results: We found that both peak systolic velocity and WSS in the AAo decreased significantly post-operatively, indicating successful restoration of aortic 3D blood flow dynamics.
Impact: Unicuspid Aortic Valve (UAV) is a rare yet important subset of Bicuspid Aortic Valve (BAV). Here, we analyze the hemodynamics of a larger pre- and post-operative UAV cohort with the inclusion of wall shear stress (WSS).
INTRODUCTION
Unicuspid Aortic Valve (UAV) is a congenital malformation that is a rare yet important morphological subset of Bicuspid Aortic Valve (BAV)1. Patients typically present in the third to fifth decade of life with aortic stenosis or regurgitation and represent approximately 5% of patients requiring surgery for aortic stenosis2,3. Non-invasive four-dimensional (4D) flow magnetic resonance imaging (MRI) has proven useful in studying complex hemodynamic patterns in patients with aortic valve disease, including the ascending aorta (AAo). While 4D flow data exists comparing the wall shear stress (WSS) and peak systolic velocity in BAV, this patient cohort dedicated to UAV pre- and post-operative hemodynamic parameters is novel due to its size and examination of WSS. Our goal was to describe and evaluate post-interventional hemodynamic changes in the AAo of UAV patients.METHODS
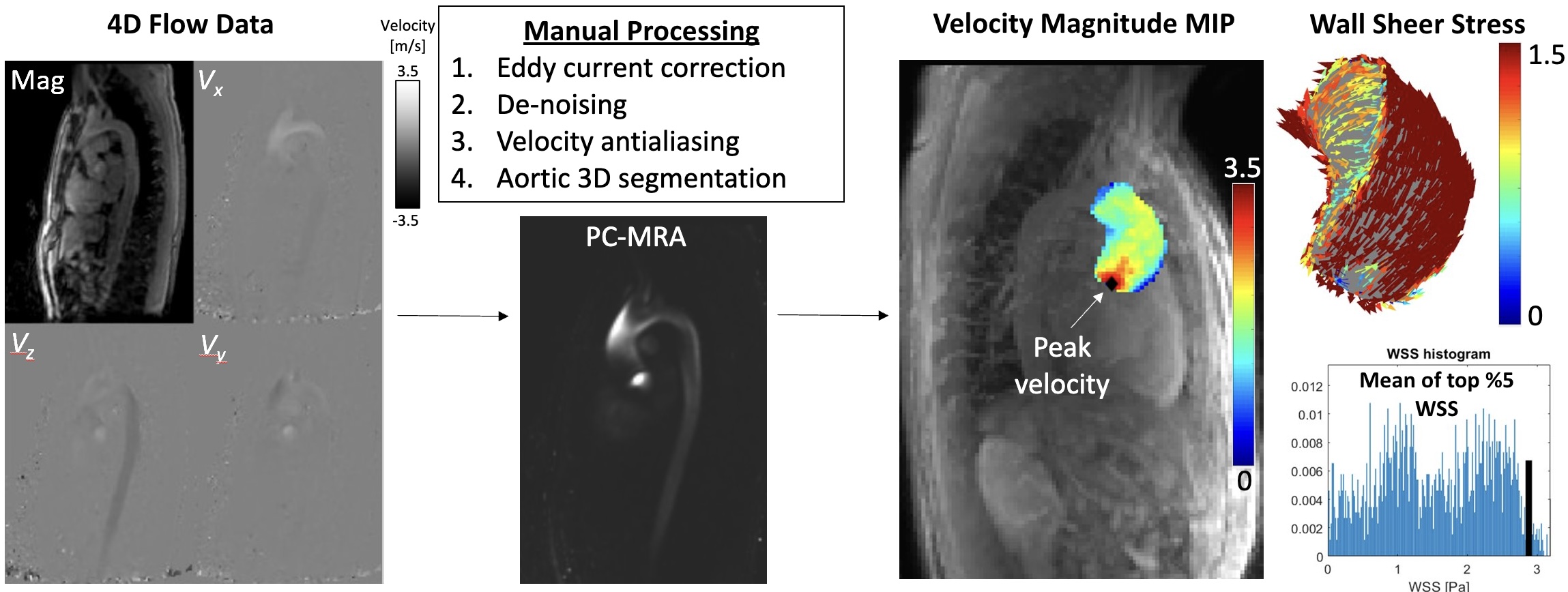
Patients with a UAV who underwent pulmonary autograft replacement of their UAV between February 2020 and August 2023 were identified (25 patients). Of those patients, 13 had pre- and post-operative 4D flow MRI exams between July 2018 and August 2023. All MRIs were performed using 1.5 or 3.0T systems (Siemens, Germany) and included either a sagittal-oblique, retrospectively ECG and respiratory-gated aortic 4D flow acquisition, or a coronal, retrospectively ECG-gated and free-breathing whole heart 4D flow acquisition. The imaging parameters for the scans were as follows (mean±SD): spatial resolution (mm3) = 2.6±0.2 x 2.6±0.2 x 3.0±0.2, echo time (TE) = 2.15±0.12 msec, repetition time (TR) = 9.51±0.61 msec, temporal resolution = 31.3±5.1 msec, and velocity encoding (VENC) = 312±116 cm/sec. Data were manually processed by a trainee with two years of experience to correct for eddy currents, velocity noise, and aliasing, and to generate a 3D segmentation of the thoracic aorta (Figure 1). The ascending aorta (AAo) was then defined by placing a plane proximal to the brachiocephalic trunk, after which the AAo systolic peak velocity and AAo WSS were calculated. The systolic peak velocity in the AAo was determined using a voxel-wise approach as the maximum velocity (98th percentile) within the AAo segmentation at peak systole. The systolic peak WSS was calculated as the average of the top 5% of magnitude WSS values mapped on the AAo surface at peak systole. Statistical analysis assessed normality using the Shapiro-Wilk test. Paired t-tests were utilized to determine if there was a difference in peak velocity and WSS in the AAo before and after UAV replacement.RESULTS
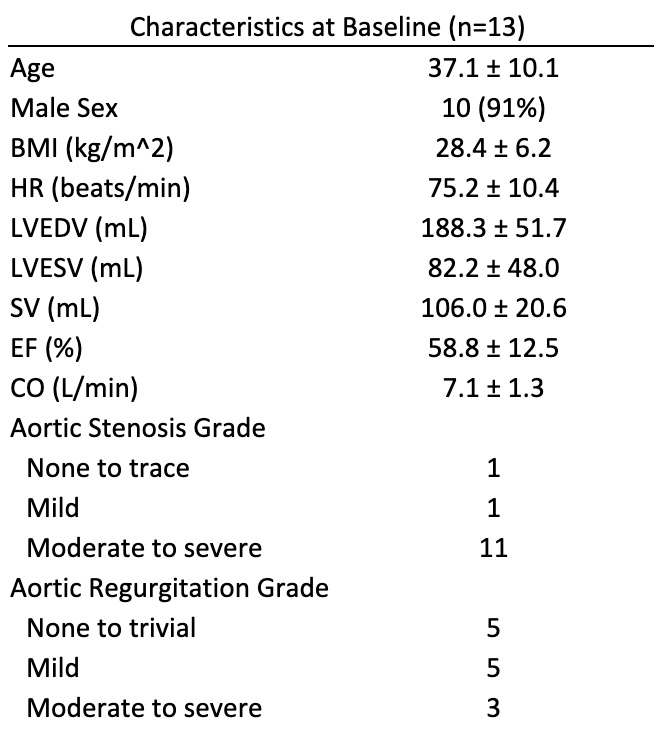
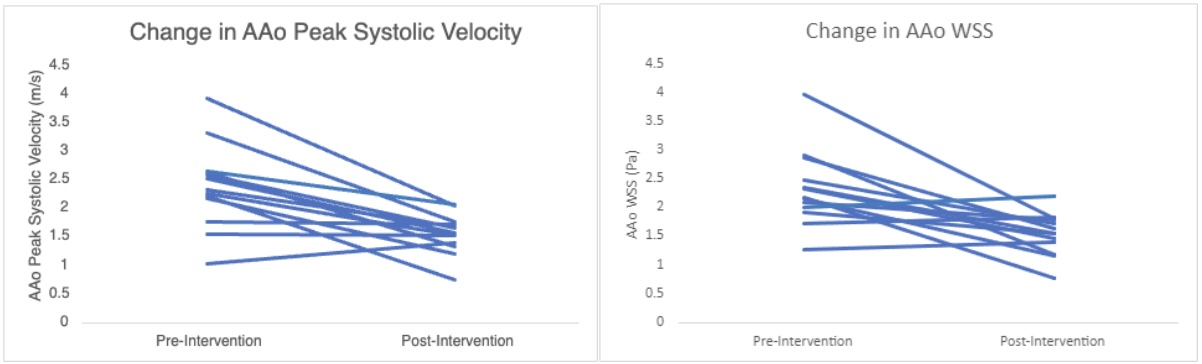
Thirteen patients (age: 37.1±10.1 years, 11 males) who underwent UAV replacement with n=26 MRIs (2/patient, before and after surgery) acquired between 2018 to 2023 were included. Patients’ characteristics at baseline are shown in Table 1. Twelve of 13 patients demonstrated a reduction in their AAo peak systolic velocity and 10 of 13 demonstrated a reduction in AAo WSS (Figure 2). In the two patients who had decreased post-intervention peak systolic velocity and increased WSS, their pre-operative MRIs occurred an average of 29 days before their surgery. However, in the one patient who experienced increases in both hemodynamic variables had their pre-intervention MRI 83 days before their surgery. In this patient, their true pre-interventional AAo peak systolic velocity may have been higher than reported. In the entire cohort, mean systolic peak velocity before and after UAV replacement were 2.40±0.74 m/s and 1.57±0.35 m/s, respectively (p < 0.01), and mean AAo WSS before and after UAV replacement were 2.34±0.66 Pa and 1.56±0.36 Pa, respectively (p < 0.01).DISCUSSION
The positive effects of aortic valve replacement on AAo hemodynamics have been previously described in patients with BAV, functional UAV (fUAV), and small cohorts of UAV patients3,4,5,6. Results from this study show a significant decrease in both peak systolic velocity and WSS in the AAo of UAV patients after undergoing valve replacement surgery. Individually, most patients experienced expected reduction in their AAo peak systolic velocity and WSS (12/13 and 10/13, respectively). Overall, these results reveal value in assessing UAV patients with 4D flow MRI to assess hemodynamics, including peak systolic velocity and WSS. Further research should be conducted to confirm these findings and future direction of investigation may include evaluation of the stability of post-operative hemodynamics further into the post-operative period.CONCLUSION
Peak systolic velocity and wall shear stress are significantly reduced in unicuspid aortic valve patients after undergoing pulmonary autograft replacement. These results indicate the value of assessing unicuspid aortic valve patients with 4D flow MRI to quantify peak systolic velocity and wall shear stress. By using 4D flow MRI quantifications, the potential degree of success for the surgical intervention may be assessed, and those patients requiring more comprehensive follow-up may be identified.Acknowledgements
No acknowledgement found.References
- Zhu Y, Roselli EE, Idrees JJ, Wojnarski CM, Griffin B, Kalahasti V, Pettersson G, Svensson LG. Outcomes After Operations for Unicuspid Aortic Valve With or Without Ascending Repair in Adults. Ann Thorac Surg. 2016 Feb;101(2):613-9. doi: 10.1016/j.athoracsur.2015.07.058.
- Singh S, Ghayal P, Mathur A, Mysliwiec M, Lovoulos C, Solanki P, Klapholz M, Maher J. Unicuspid unicommissural aortic valve: an extremely rare congenital anomaly. Tex Heart Inst J. 2015 Jun 1;42(3):273-6. doi: 10.14503/THIJ-13-3634.
- Drullinsky D, Mehta CK, Scott MB, et al. Four-Dimensional Magnetic Resonance After Ross Procedure for Unicuspid Aortic Valve. Circ Cardiovasc Imaging. 2021;14(4):e011500. doi:10.1161/CIRCIMAGING.120.011500
- Lenz A, Petersen J, Riedel C, Weinrich JM, Kooijman H, Schoennagel BP, Adam G, von Kodolitsch Y, Reichenspurner H, Girdauskas E, Bannas P. 4D flow cardiovascular magnetic resonance for monitoring of aortic valve repair in bicuspid aortic valve disease. J Cardiovasc Magn Reson. 2020 Apr 30;22(1):29. doi: 10.1186/s12968-020-00608-0.
- Entezari, P., Schnell, S., Mahadevia, R., Malaisrie, C., McCarthy, P., Mendelson, M., Collins, J., Carr, J.C., Markl, M. and Barker, A.J. (2014), From unicuspid to quadricuspid: Influence of aortic valve morphology on aortic three-dimensional hemodynamics. J. Magn. Reson. Imaging, 40: 1342-1346. https://doi.org/10.1002/jmri.24498
- Ma, L. E., Vali, A., Blanken, C., Barker, A. J., Malaisrie, C., McCarthy, P., Collins, J. D., Carr, J. C., Schnell, S., & Markl, M. (2018). Altered aortic 3-dimensional hemodynamics in patients with functionally unicuspid aortic valves. Circulation: Cardiovascular Imaging, 11(8). https://doi.org/10.1161/circimaging.118.007915
Figures