4769
Age and sex-matched intracardiac force analysis for repaired tetralogy of fallot patients using 4D flow MRI1University of Calgary, Calgary, AB, Canada, 2Radiology, University of Calgary, Calgary, AB, Canada
Synopsis
Keywords: Flow, Cardiovascular, flow
Motivation: Cardiac force analysis shows promise for non-invasive treatment and diagnosis for patients with heart disease.
Goal(s): Assessing intracardiac forces as a metric of diagnostics in repaired tetralogy of fallot patients which require lifelong monitoring.
Approach: Intracardiac forces were analyzed using segment in twenty rTOF patients and 20 control patients. These were compared in age and sex-matched groups.
Results: Age and sex-matched analysis showed significant differences in intracardiac forces for control and patient groups. Results also indicated that men and women may be affected differently by rTOF, as there were significant differences between the gender groups with rTOF.
Impact: Evaluation of intracardiac forces shows promise as a biomarker for heart disease in rTOF females and males; also demonstrates potential for other diseases, although more investigations must be conducted. This can be used in clinical settings, for non-invasive diagnoses.
Introduction
Tetralogy of Fallot (TOF) is the most prevalent congenital heart disease, affecting 9/1000 live births1. Individuals born with TOF generally receive surgical repair (rTOF) in early life and go on to live long lives2. The 4D flow MRI is a recent development in health sciences that can be utilized to quantify and visualize hemodynamics and has shown to be promising in the diagnostics of early diseases in a non-invasive way3. Ventricular intracardiac pressures have been quantified in rTOF patients and controls, although there is little scientific research that included sex and age-matched analysis in rTOF patients compared to controls. This research aims to quantify the differences in hemodynamic forces in the left ventricle in patients with rTOF and healthy controls with respect to age and sex. We hypothesize that hemodynamic forces in the heart will increase with age in both rTOF patients and controls.Method
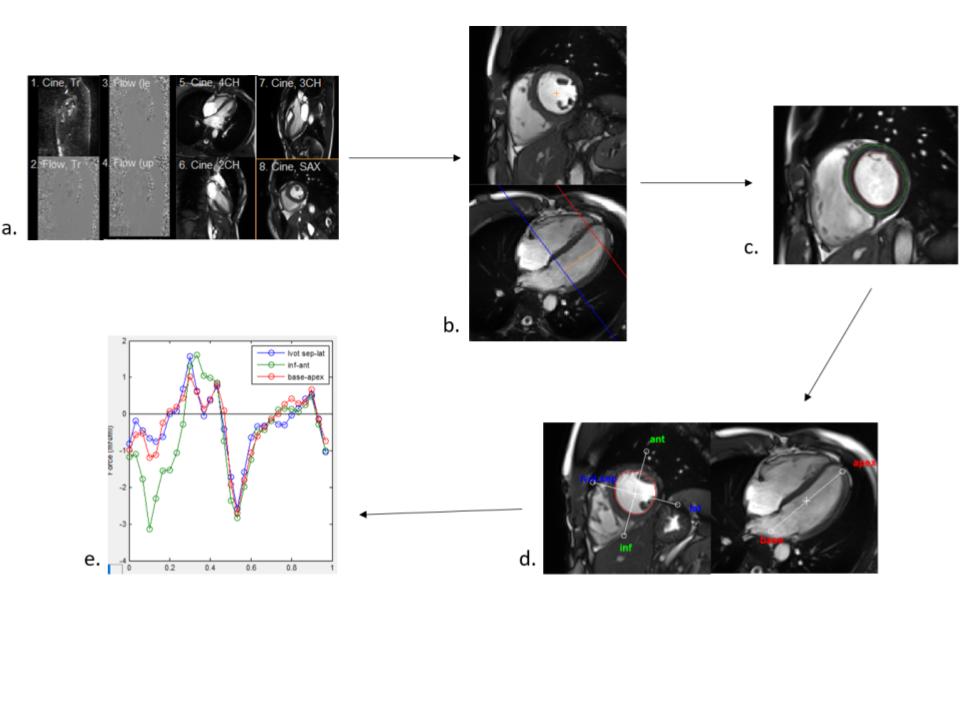
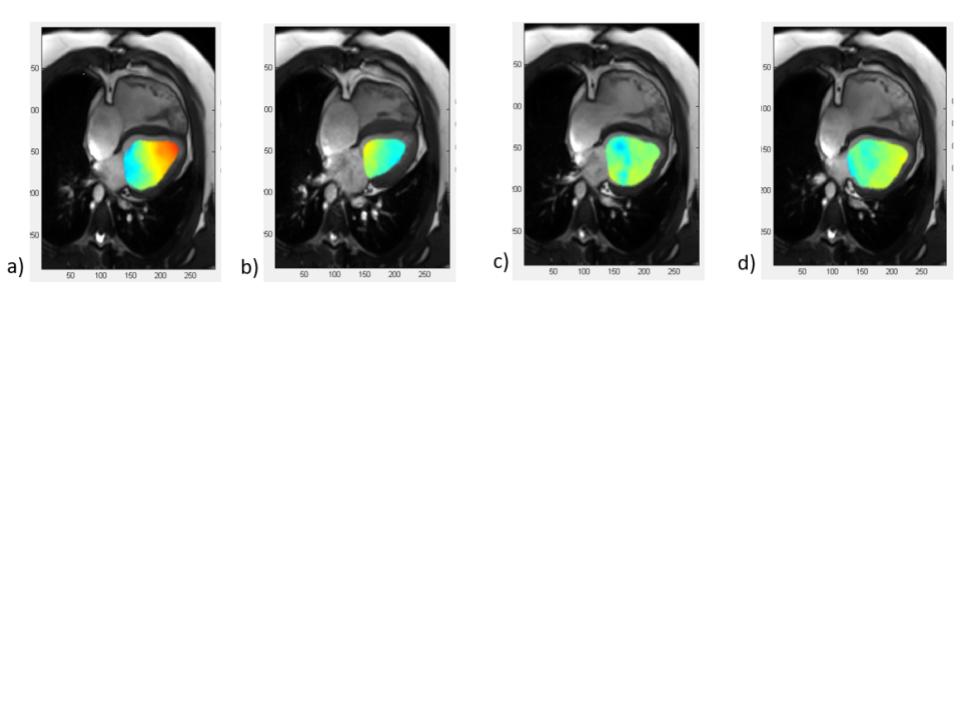
This study included 20 patients with rTOF and 20 control patients. All subjects provided written consent to participate in the study. All subjects underwent a standardized cardiac imaging protocol, including time-resolved balanced steady-state free precession cine imaging in 4-chamber, 3-chamber, 2-chamber, and short-axis views of the left ventricle. Moreover, 4D Flow MRI was performed using retrospective ECG gating and a respiratory navigator for the comprehensive hemodynamic assessment of the whole heart. 4D flow acquisition parameters included: velocity encoding: 150-250 cm/s, flip angle = 15 degrees, spatial resolution: 2.0-3.5 x 2.0-3.5 x 2.5-3.5 mm3. Segment4 was used to calculate the hemodynamic forces in the left ventricle using the LV cine images for segmentation of the 4D Flow MRI data (see Figure 1). The average systolic force, peak systolic force, peak diastolic force and average overall force (see Figure 2) can be analyzed for all cases in the left (and right) ventricle(s), allowing for the determination of the variation of forces in healthy volunteers and patients with rTOF.Results
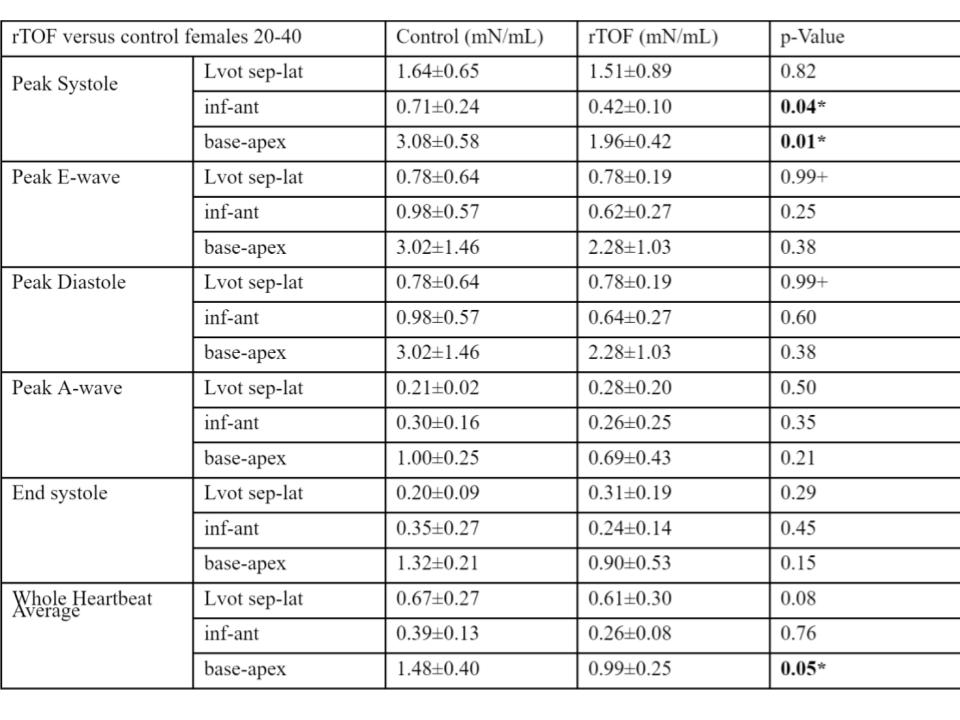
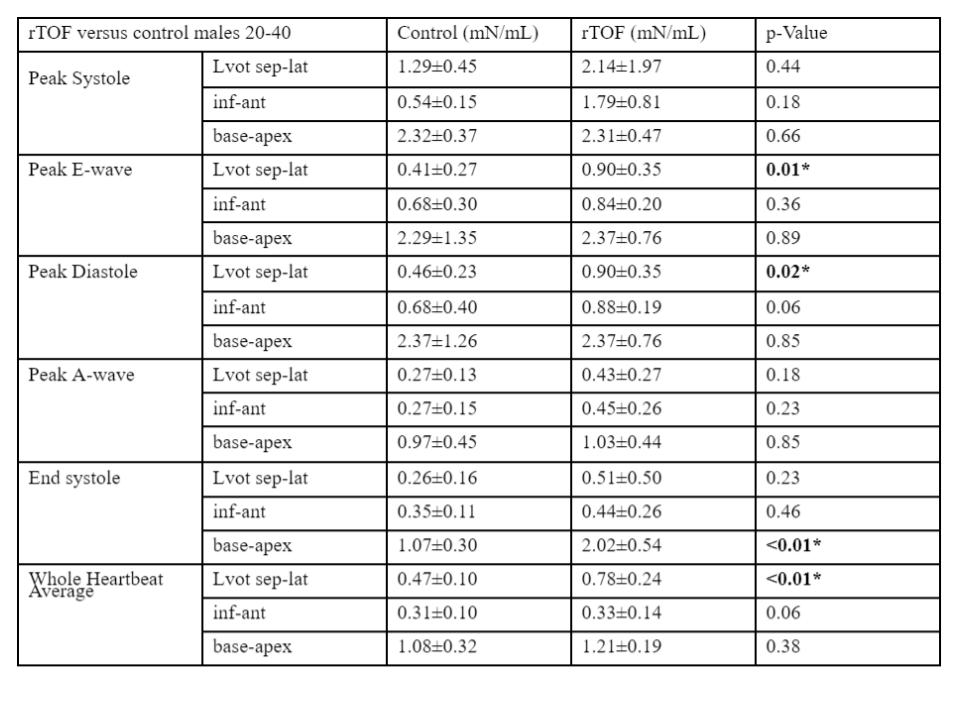
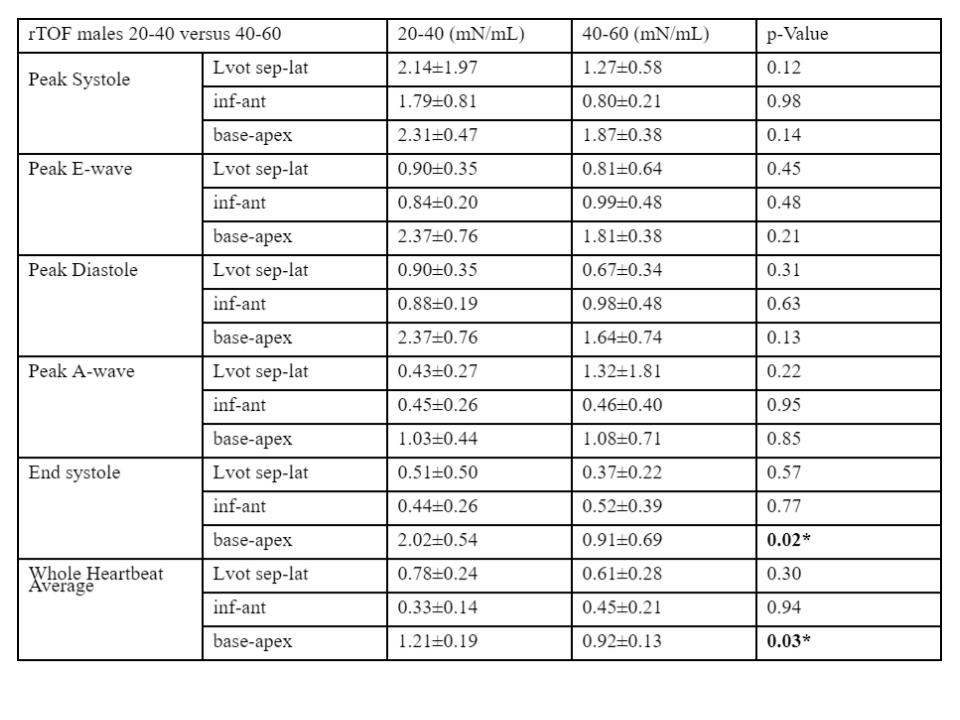
rTOF affected patients and healthy controls have significantly different basal-apical forces during systole and inferior-anterior and septal-lateral forces during diastole. Females aged 20-40 with rTOF have significantly differing inferior-anterior (0.42 mN/mL versus 0.71 mN/mL, p=0.82) and basal-apical forces (1.96 mN/ML versus 3.08 mN/mL,p=0.01) during systole when compared with controls. Males aged 20-40 with rTOF when compared with controls have significantly differing septal-lateral forces (0.90 mN/mL versus 0.46 mN/mL,p=0.01) during peak diastole, septal-lateral (0.90mN/mL versus 0.41mN/mL, p=0.02) during peak E-wave, and septal lateral for the full heartbeat (0.78mN/mL versus 0.47mN/mL, p=<0.01). Females and males aged 40-60 have no significantly differing forces compared to controls. Comparison of rTOF females 20-40 and 40-60 yielded no significantly differing forces were found, however, control females 20-40 versus 40-60 had differing peak systole forces (2.37mN/mL versus 2.11mN/mL, p=0.02) in the basal-apical axis, and end systole (1.07mN/mL versus 0.72mN/mL, p=0.02) in the basal-apical axis. rTOF males had differing forces in end systole in the basal-apical axis (2.02mN/mL versus 0.91mN/mL, p=0.02) and for the full heartbeat in the basal-apical axis (1.21mN/mL versus 0.92mN/mL, p=0.03).Discussion
This experiment included only 4 cases for the diseased and 4 cases for the healthy groups for the female and male groups aged 40-60. The lower number of cases may have resulted in insufficient data for statistical testing to yield an accurate result. Repetition of the experiment with a higher number of cases may yield more accurate results.Conclusion
Evaluation of intracardiac forces shows promise as a biomarker for heart disease in young females and males. The differing forces also suggest hemodynamic forces do not return to the same condition as a completely healthy heart after post-surgical repair. There were significant differences found in young patients, but none in older patients suggesting the heart may eventually normalize as a patient ages. Additionally, the aspects that differed in females aged 20-40 were different than those that differed in males aged 20-40, suggesting intracardiac forces in females and males are affected differently by rTOF.Acknowledgements
No acknowledgement found.References
References
1. Marshall, T., Ryan, J., & Hung, S. (2023, January 29). Tetralogy of Fallot: Video, Anatomy & Definition. Osmosis. Retrieved October 1, 2023, from https://www.osmosis.org/learn/tetralogy-of-fallotMayo Clinic Staff. (2021, August 17).
2. Tetralogy of Fallot - Diagnosis and treatment. Mayo Clinic. Retrieved October 1, 2023, from https://www.mayoclinic.org/diseases-conditions/tetralogy-of-fallot/diagnosis-treatment/drc-20353482
3. Sjoberg, P., Toger, J., hedstrom, E., Arvidsson, P., Heiberg, E., Arheden, H., Gustafsson, R., Nozohoor, S., & Carlsson, M. (2019, June 24). Altered biventricular hemodynamic forces in patients with repaired tetralogy of Fallot and right ventricular volume overload because of pulmonary regurgitation. American Physiological Society. Retrieved October 1, 2023, from https://journals.physiology.org/doi/full/10.1152/ajpheart.00330.2018?rfr_dat=cr_pub++0pubmed&url_ver=Z39.88-2003&rfr_id=ori%3Arid%3Acrossref.org
4. Heiberg, J., Sjoren, M., Ugander, M., Carlsson, M., Engblom, H., & Arheden, H. (2010). Design and Validation of Segment - A Freely Available Software for Cardiovascular Image Analysis. BMC Medical Imaging.
Figures