4768
Determining the Reproducibility and Reliability of 2D- and 4D flow MRI Mitral Valve Regurgitation Quantification Methods1Cardiology, Inselspital, University Hospital Bern, Bern, Switzerland, 2Graduate School for Cellular and Biomedical Sciences (GCB), University of Bern, Bern, Switzerland, 3Translation Imaging Center (TIC), Swiss Institute for Translational and Entrepreneurial Medicine, Bern, Switzerland, 4Inselspital, University Hospital Bern, Bern, Switzerland, 5Department of Diagnostic, Interventional and Pediatric Radiology (DIPR), Inselspital, University Hospital Bern, Bern, Switzerland
Synopsis
Keywords: Flow, Cardiovascular, Data Analysis, Challenges, Flow, Heart, Valves, Velocity & Flow, Validation, 4D-flow, 2D-flow
Motivation: Mitral valve regurgitation (MVR) quantification is crucial for diagnosis and treatment of patients with mitral valve disease. While different MRI based MVR quantification methods exist, their correlation with one another and their reproducibility and reliability remains unknown.
Goal(s): To determine the reproducibility and reliability of four different 2D- and 4D flow MVR volume quantification methods based on CMR.
Approach: The intermethod, inter- and intra-reader agreements between four different methods, 4D-flowAIM, 2D-PCstandard, 2D-PCMV, Volumetric, were compared for patients with severe secondary MVR.
Results: Among all techniques, 2D-PCstandard and Volumetric methods were the most reliable ones (ICC>0.99, P-value<0.001).
Impact: 2D-PCstandard and Volumetric methods quantify the MVR volume most consistently and further research with diverse MVR types and larger cohorts is needed to establish reliable conclusions for 2D-PCMV and 4D-flowAIM methods.
INTRODUCTION
Mitral valve regurgitation (MVR) is one of the common reasons for either open-heart surgery or novel minimal invasive transcatheter edge-to-edge (TEER) mitral valve repair1. While echocardiography remains the primary diagnostic tool for assessing MVR severity, cardiac MRI (CMR) is gaining recognition for its importance and ability to accurately quantify the MVR severity2. This study aims to compare different established two-dimensional (2D)- and four-dimensional (4D)-flow MVR quantification methods and determine their reproducibility by assessing intermethod, inter- and intra-reader agreements.METHODS
Patients with severe secondary MVR and reduced ejection fraction (EF < 50%) planned for TEER underwent MRI before intervention. Scans were performed at 1.5T (MAGNETOM Sola, Siemens Healthcare, Erlangen, Germany). A total of 6 patients (age: 73±15 years, all male, LVSV: 89±17, LV EF 29±20) were included. All patients were recruited prospectively and gave their written consent. Acquisition parameters, as well as patients’ demographics, are summarized in Table 1.Figure 1 summarizes all four different MVR volume quantification methods based on MRI3: (1) 2D phase-contrast standard method (2D-PCstandard), indirectly measuring MVR volume by subtracting aortic stroke volume (SVAAo) assessed by 2D-PC from left ventricular SV (LVSV) assessed by cine short-axis CMR images, (2) the 2D-PC mitral valve method (2D-PCMV), quantifying MVR volume by subtracting the stroke volume (SV) derived from forward flow through the mitral valve (MVSV) from SVAAo, (3) the Volumetric method, which calculates the disparity between LVSV and right ventricular SV (RVSV) from cine CMR images, and (4) the 4D flow intraventricular annular inflow (4D-flowAIM), calculating regurgitation volume by subtracting the SVAAo from the stroke volume (SV) derived from MVSV. Measurements were performed offline using the CVI42 software (Circle Cardiovascular Imaging, Calgary, Canada) by two readers, YS and MB, twice.
Inter- and intra-reader agreement analyses were conducted using Python, measuring interclass correlations (ICC) and Pearson correlation (r) coefficients. MVR severities for each measurement were classified into three groups: mild (MVRvolume < 30 ml), moderate (MVRvolume = 30-59), and severe (MVRvolume > 60 ml)4.
RESULTS
MVR volumes measured by both readers demonstrated stark differences between quantification methods. MVR volumes were 31±8 ml (2D-PCstandard), 53±26 ml (2D-PCMV), 18±14 ml (Volumetric), and 26±16 ml (4D-flowAIM) (Figure 2).2D-PCstandard had poor correlation with both 2D-PCMV (r=0.233, P=0.656) and Volumetric method (r=-0.056, P=0.916) methods. 2D-PCMV had a moderate correlation with the Volumetric method (r=-0.642, P=0.169). 4D-flowAIM had moderate correlation with 2D-PCstandard (r=-0.617, P=0.192), and Volumetric method (r=-0.405, P=0.425) but poor correlation with 2D-PCMV (r=0.202, P=0.701) (Table 2).
The inter- and intra-reader agreements show the least bias for 2D-PCstandard and Volumetric methods (Figure 3). When comparing all methods, 2D-PCstandard and Volumetric methods had excellent inter- and intra-reader reliability (ICC >=0.9). However, 4D-flowAIM and 2D-PCMV had poor inter- and intra-reader reliability (ICC < 0.5). With 2D-PCstandard and Volumetric, the MVR severity is consistent between readers and measurements but varies for 4D-flowAIM and 2D-PCMV measurements.
DISCUSSION
We statistically compared the intermethod, inter-, and intra-reader agreements between the four different MVR quantification methods for patients with severe secondary MVR. Despite the inconsistency between methods, 2D-PCstandard and Volumetric measurements didn’t affect the MVR severity classification across readers and inter-readers quantifications. Whereas 4D-flowAIM lacks this consistency, it’s the only single acquisition method capturing intra-cardiac flow information for the same cardiac cycle.Besides the moderate agreement between the 2D-PCstandard and 4D-flowAIM methods, all other methods correlated poorly with each other. The well-established 2D-PCstandard and Volumetric methods demonstrated eloquent reliability and reproducibility across intra- and inter-reader measurements, unlike 2D-PCMV and 4D-flowAIM methods, which might be due to the mitral valve’s saddle shape and through-plane motion3. Besides, MVR volume quantification with the 4D-flowAIM method is dependent on the positioning of the reconstructed plane and adequately contouring the valve plays a crucial role in both 2D-PCMV and 4D-flowAIM quantifications3–5.
The limited size of our patient cohort is the primary limitation of this study, and since only patients with severe secondary MVR were included, the findings may not be generalizable to patients with lower-grade or primary MVR. Additionally, there is no consensus on the appropriate valve contouring and placement of the reconstructed plane in 4D-flow imaging.
CONCLUSION
We compared various MVR volume quantification methods using CMR. The 2D-PCstandard and Volumetric methods yielded consistent results, contrasting with the 2D-PCMV and 4D-flowAIM methods. However, future studies are required to include diverse MVR types, larger cohorts, and an established consensus on measurement approaches with the 2D-PCMV and 4D-flowAIM methods.Acknowledgements
This study was a part of the PRE-MITRA project funded by the Swiss National Science Foundation (SNF) (grant number: 197754).References
- Iung, B. et al. A prospective survey of patients with valvular heart disease in Europe: The Euro Heart Survey on Valvular Heart Disease. Eur. Heart J. 24, 1231–1243 (2003).
- Le Goffic, C. et al. Quantitative evaluation of mitral regurgitation secondary to mitral valve prolapse by magnetic resonance imaging and echocardiography. Am. J. Cardiol. 116, 1405–1410 (2015).
- Safarkhanlo, Y. et al. Mitral valve regurgitation assessed by intraventricular CMR 4D-flow: a systematic review on the technological aspects and potential clinical applications. Int. J. Cardiovasc. Imaging 1–15 (2023).
- Garg, P. et al. Assessment of mitral valve regurgitation by cardiovascular magnetic resonance imaging. Nat. Rev. Cardiol. 17, 298–312 (2020).
- Fidock, B. et al. Standard and emerging CMR methods for mitral regurgitation quantification. Int. J. Cardiol. 331, 316–321 (2021).
Figures
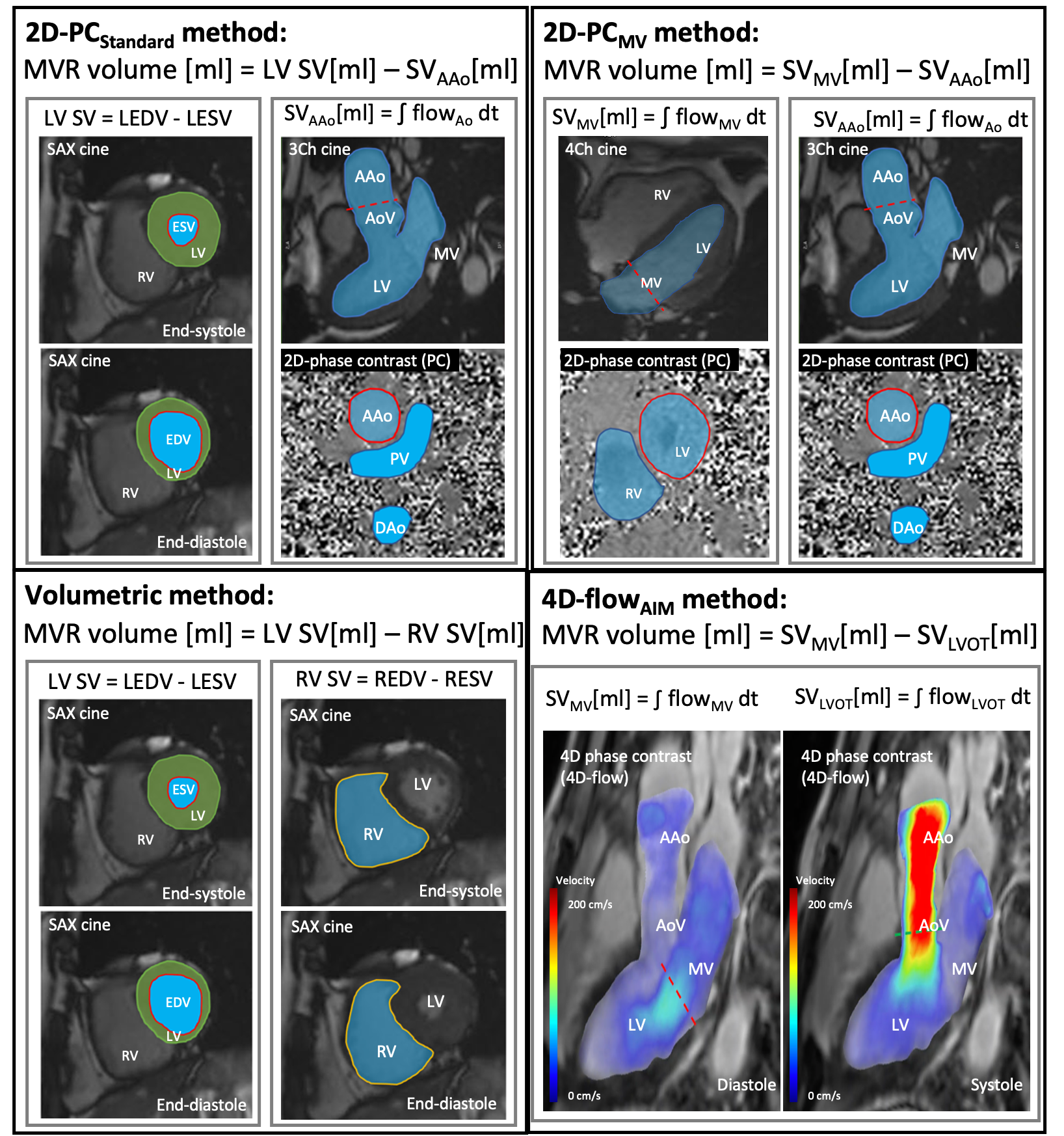
Figure 1: Illustration of MVR quantification methods.
2D-PCstandard; 2D-PCMV; Volumetric; 4D-flowAIM; MVR, Mitral Valve Regurgitation; LVSV, Left Ventricle Stroke Volume; AoPC, Aortic Forward Flow; LEDV, Left Ventricle End Diastolic Volume; LESV, Left Ventricle End Systolic
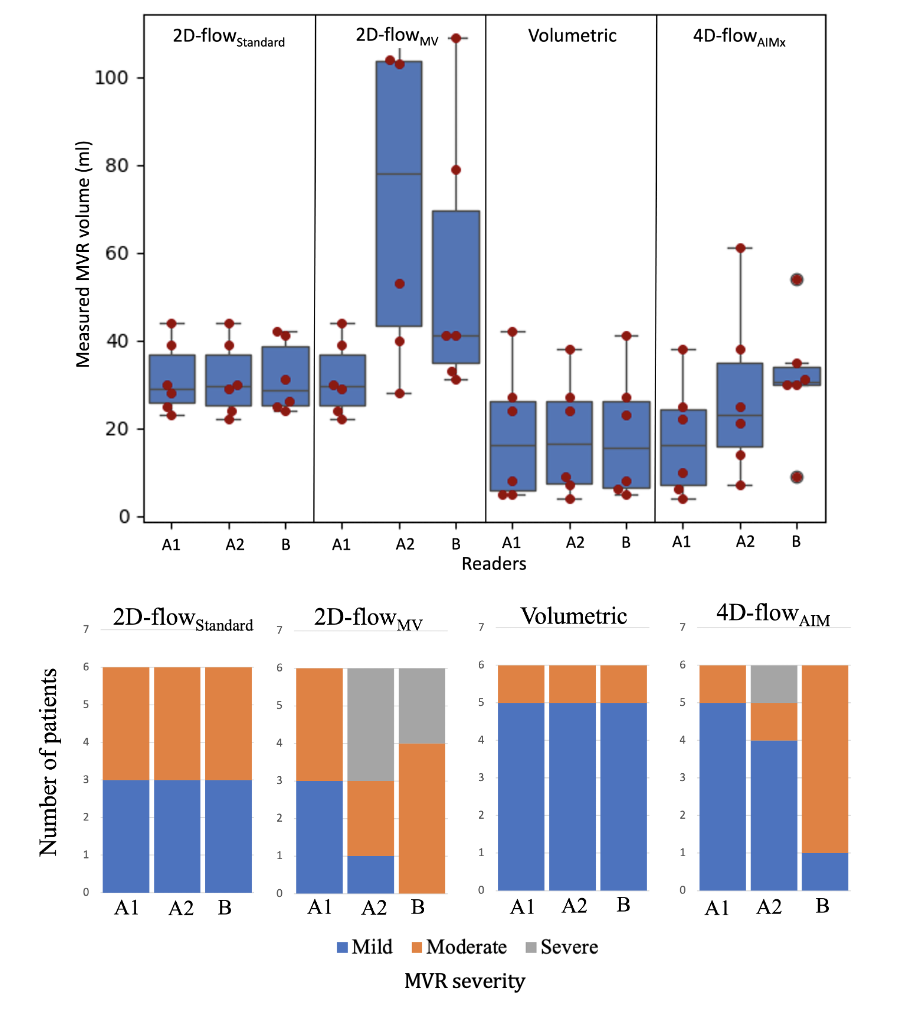
Figure 2: Mitral Valve Regurgitation volumes measured with the four different CMR quantification methods.
Two separate measurements with the same reader A twice, A1 and A2, and two different readers A and B.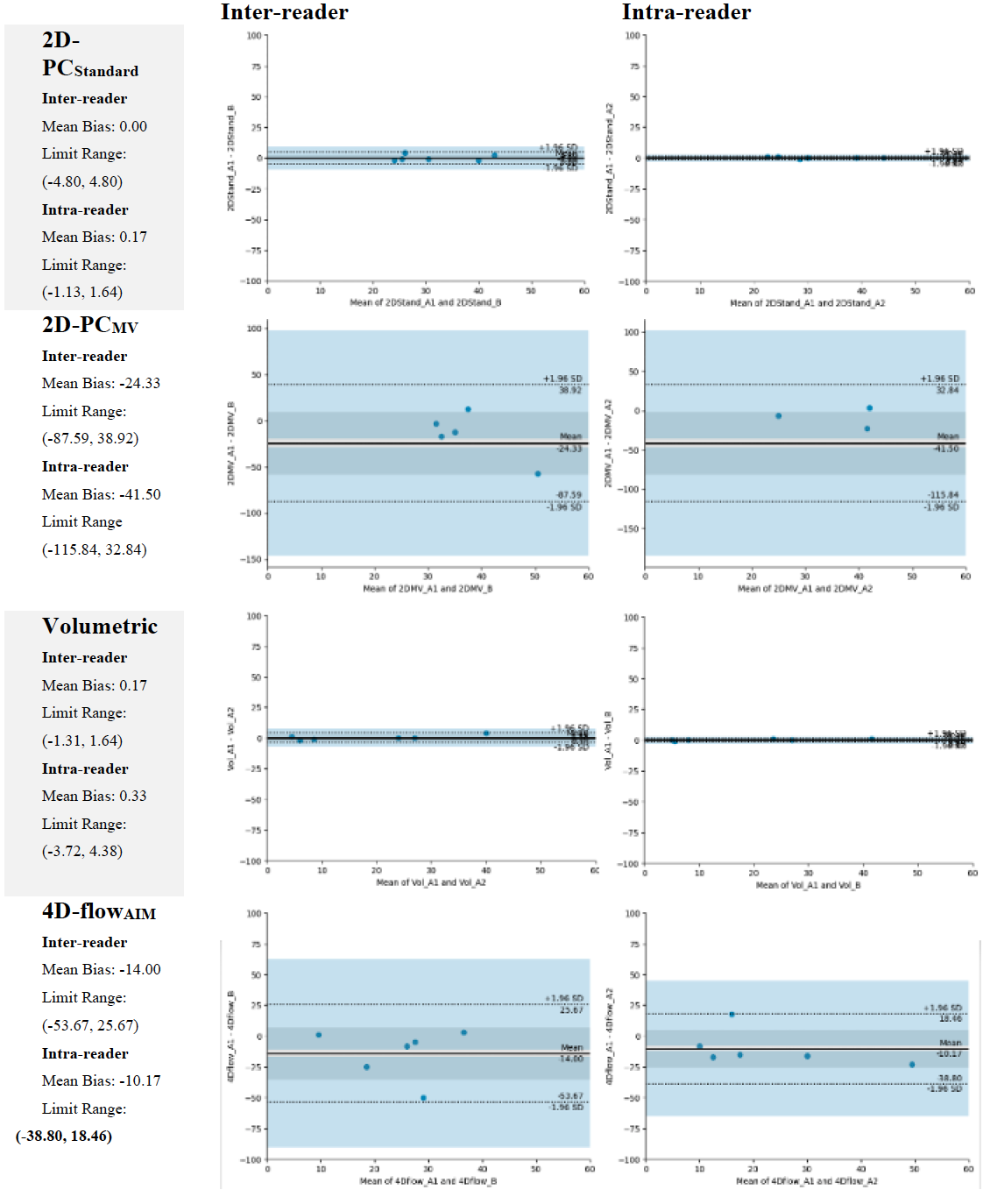
Figure 3: Intra and inter-reader Bland-Altman plots for each MVR quantification method.
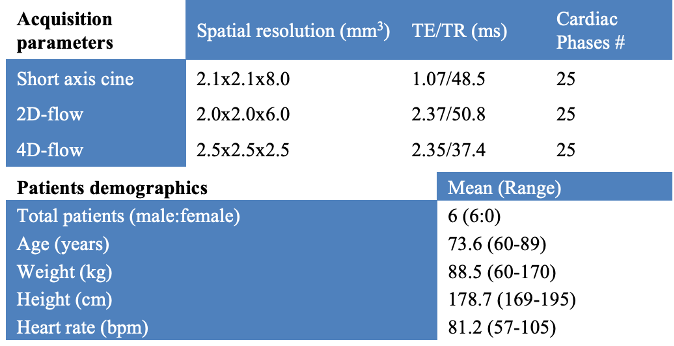
Table 1: Acquisition parameters and patients' population features
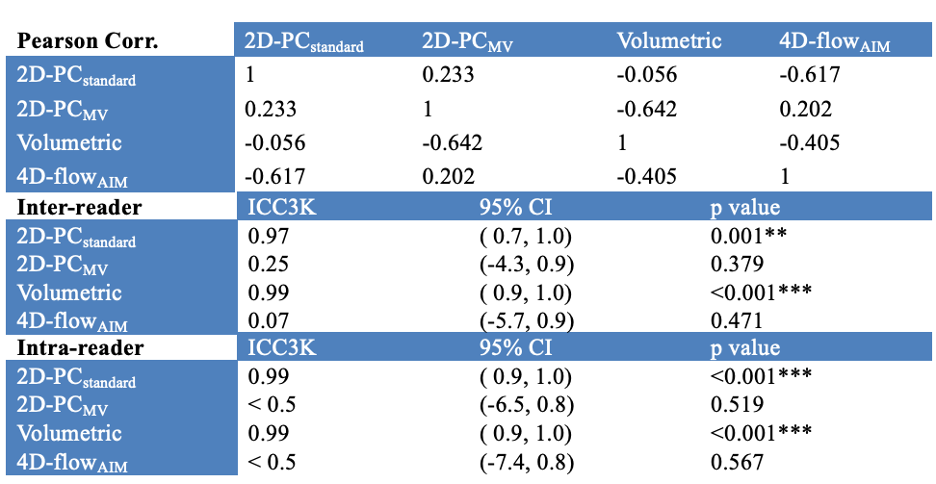
Table 2: Correlation coefficients between different methods and Inter- and Intra-reader consistency for MVR quantification with CMR.
r ≥ 0.9, excellent correlation; r = 0.7–0.89, strong correlation; r = 0.4–0.7, moderate correlation; r = 0.1–0.39, weak correlation. ICC >= 0.9, excellent reliability; ICC = 0.75–0.9, good reliability; ICC = 0.5–0.75, moderate reliability; ICC < 0.5, poor reliability. The stars define the level of significance. * = 0.05, ** = 0.01, *** = 0.001