4767
Dual-Venc 5D flow MRI for Increased Velocity Dynamic Range: An in vivo Validation Study1Northwestern University, Chicago, IL, United States, 2University of Lausanne (CHUV), Lasuanne, Switzerland
Synopsis
Keywords: Flow, Cardiovascular, Hemodynamics
Motivation: Single-venc 5D flow is useful for measuring the impact of respiration on hemodynamics, however, its single velocity encoding sensitivity (venc) limit its utility in congenital heart disease patients where both venous and arterial measurements are clinically necessary.
Goal(s): We aimed to validate respiratory-resolved dual-venc 5D flow measurements in vivo.
Approach: Nine healthy volunteers underwent CMR studies including dual-venc 5D flow, single-venc 5D flow, and 4D flow. Net flow and peak flow were compared.
Results: We found good agreement of net flow and peak flow with both 4D flow and single-venc 5D flow MRI, with an 85% increase in velocity-to-noise ratio.
Impact: Dual-venc 5D flow increases velocity-to-noise ratio by 85% compared to single-venc 5D flow with good agreement in respiratory-resolved flow measurements. The method may improve simultaneous measurement of venous and arterial flows, which is often necessary in congenital heart disease patients.
Introduction
Respiration is an important driver of hemodynamics in congenital heart disease patients, such as those post-Fontan repair1,2 or with cardiac shunting.2 5D flow MRI3 is a free-running, self-gated, highly accelerated acquisition that measures 3D blood flow velocities over the cardiac and respiratory cycles. However, congenital heart disease patients often require venous and arterial measurements in the same study (e.g., aortopulmonary collateral quantification) which is difficult to achieve with a single velocity encoding sensitivity (venc). We previously reported the development a dual-venc 5D flow MRI method for increased velocity dynamic range and velocity-to-noise ratio (VNR), which was validated in vitro using a pulsatile flow phantom.4 The goal of this study was to build on these findings and evaluate the performance of the technique in a cohort of healthy volunteers.Methods
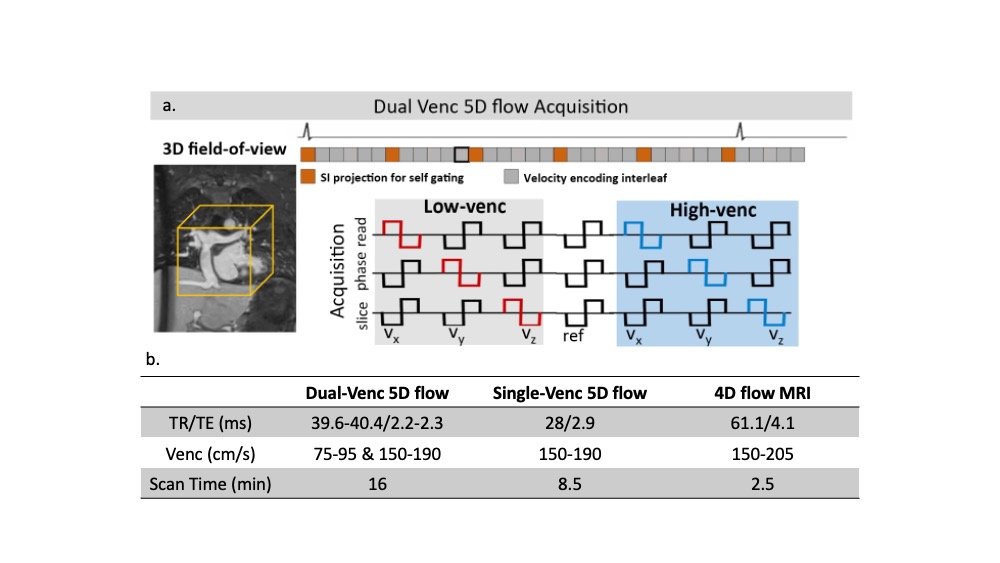
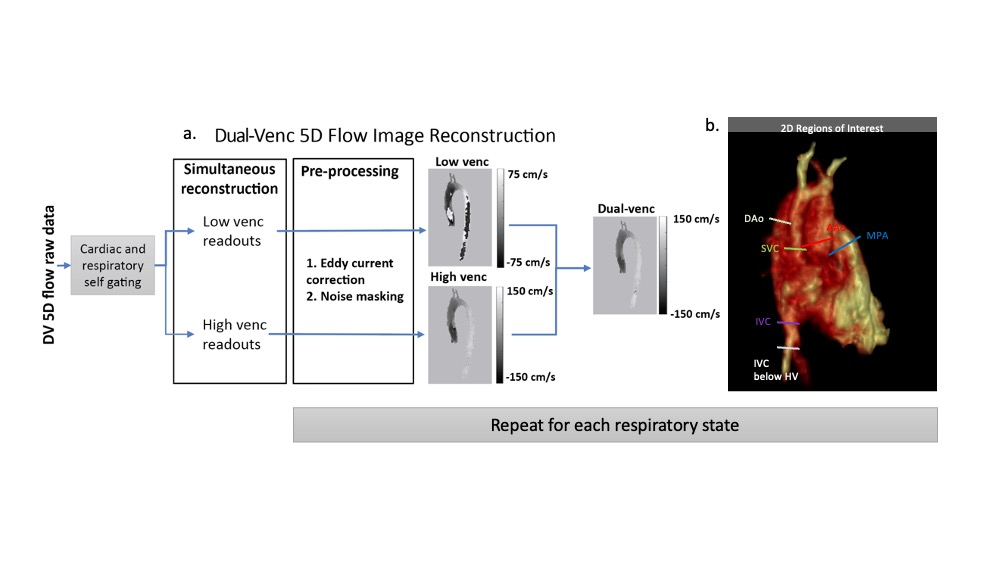
Nine healthy volunteers (35±12 yrs, M/F: 8/1) were prospectively recruited for a cardiac MR study, including conventional 4D flow MRI, single-venc 5D flow MRI, and dual-venc 5D flow MRI (Fig1b).4 Dual-venc (DV) 5D flow MRI employed a 7-point velocity encoding scheme to measure both low venc (LV) and high venc (HV) velocity data (Fig1a). A difference image (HV-LV) was used to identify and correct velocity aliasing in the LV data as previously described5 (Fig2a). Both single-venc (SV) and DV 5D flow are radially acquired, free-running sequences with interleaved superior-inferior (SI) readouts. Cardiac and respiratory signals were extracted from the SI readouts for retrospective gating (40ms cardiac resolution, 4 respiratory states) and images were reconstructed using compressed sensing. For each subject and all flow imaging techniques (4D, SV 5D, DV 5D), net flow and peak flow were measured 6 vessels using time-resolved 2D regions of interest (Fig2b). End-expiration measurements from SV and DV 5D flow were compared with conventional 4D flow MRI. Bland Altman analysis and respiratory resolved net flow curves normalized to end-expiration were used to compare SV 5D flow and DV 5D flow. Lastly, VNR (Eq1) in the entire aorta was calculated for SV and DV 5D flow images (liver segmented as static tissue).$$ VNR = {mean(velocity_{3D segmentation})}/{mean(velocity_{static tissue})} (Eq1) $$
Results
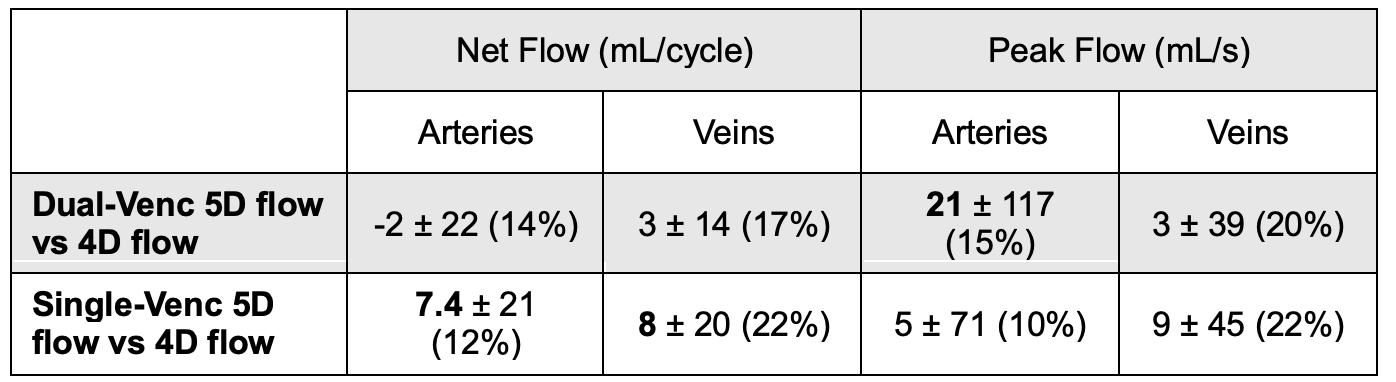
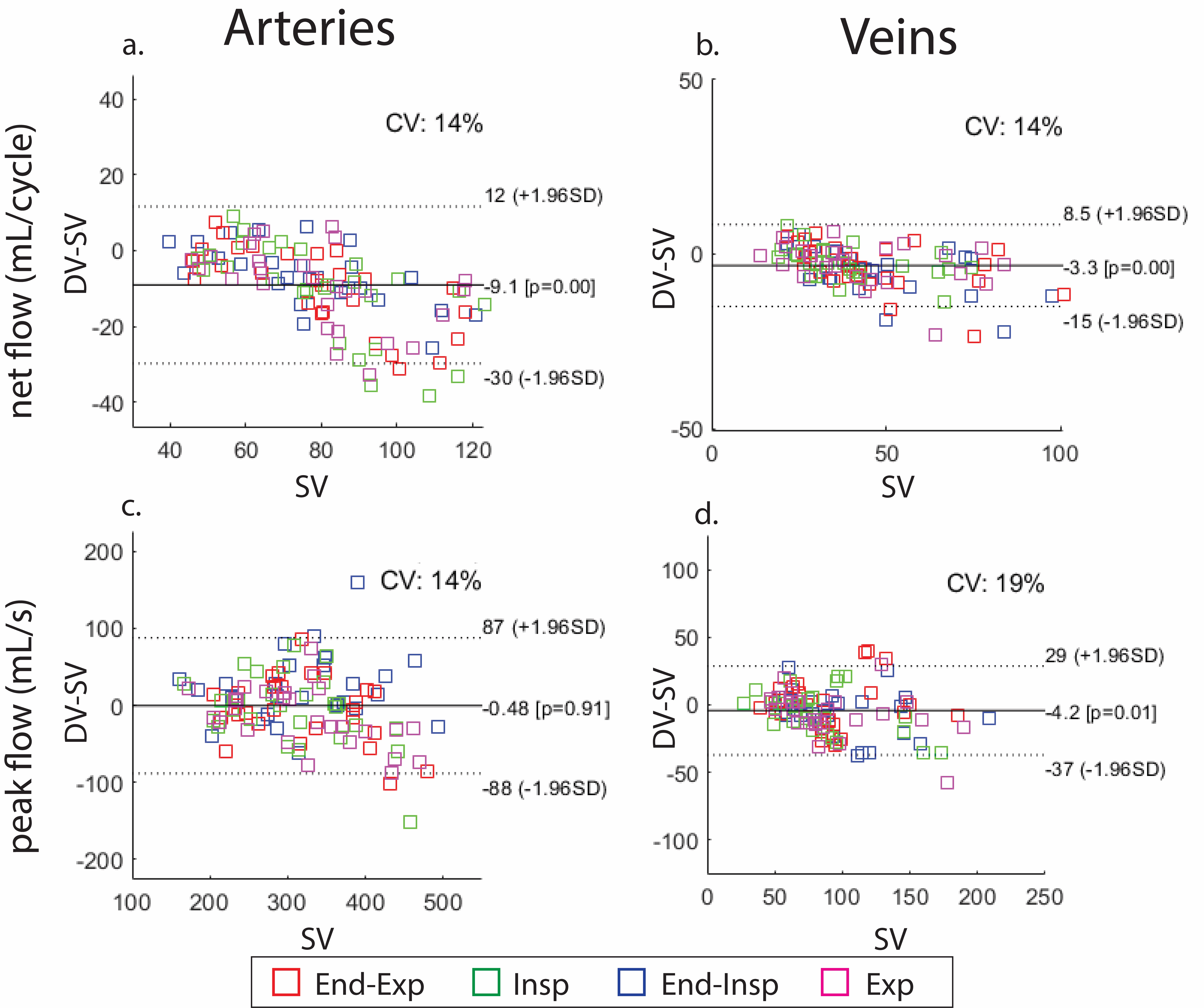
We found good agreement between 4D flow MRI and end-expiration of dual-venc 5D flow MRI (Table 1). There was no significant bias in measured net flow in the arteries (CV=14%) or veins (CV=17%). The limits of agreement were comparable or better to the agreement between single-venc 5D flow and 4D flow. Dual-venc 5D flow overestimated arterial peak flows by 33 mL/s (p=0.03, CV=15%) but had no significant bias in venous (CV=20%) peak flows. The limits of agreement were comparable to the agreement between single-venc 5D flow and 4D flow.There was good agreement in net flow and peak flow measured by single-venc 5D flow and dual-venc 5D flow. Dual-venc 5D flow underestimated net flow in both arteries (9.1 mL/cycle, p<0.01, 12% of mean net flow, Fig3a) and veins (3.3 mL/cycle, p<0.01, 8% of mean net flow, Fig3b). Dual-venc 5D flow had no significant bias in arterial peak flows (Fig3c), but venous peak flows were slightly underestimated (-4.2 mL/s, p=0.01, 4% of mean peak flow, Fig3d). Additionally, there was an 85±48% increase in VNR in dual-venc 5D flow images.
Lastly, we found excellent agreement of respiratory-resolved net flow curves without significant differences in any vessel (Fig4).
Discussion
We found good agreement between dual-venc 5D flow and 4D flow with similar levels of agreement as single-venc 5D flow compared to 4D flow. Overestimation of the peak flow in the arterial measurements may be due to imperfect respiratory state matching between the methods or differences in heart rate during each acquisition and represent a physiological difference.We demonstrated good agreement between single-venc and dual-venc 5D flow. Dual-venc 5D flow tended to underestimate net flow compared to single-venc 5D flow. This may reflect improved noise properties, such as a reduced noise floor, or differences in eddy current correction. Dual-venc 5D flow also underestimated peak flow in the arteries. This may be due to improved noise correction, but it may also be due to increased motion noise due to a longer scan time. Despite these differences, we found excellent agreement in the respiratory-resolved flow curves. Thus, dual-venc 5D flow successfully measured respiratory driven flow changes with increased VNR compared to single-venc 5D flow.
Future work is necessary to evaluate the method in patients. Additionally, motion correction should be implemented given the long scan time inherent to dual-venc 5D flow.
Conclusions
We demonstrate good agreement of dual-venc 5D flow with both 4D flow and single-venc 5D flow with an 85% increase in VNR in 9 healthy volunteers.Acknowledgements
No acknowledgement found.References
1. Wei, Z., Whitehead, K. K., Khiabani, R. H., Tree, M., Tang, E., Paridon, S. M., ... & Yoganathan, A. P. (2016). Respiratory effects on Fontan circulation during rest and exercise using real-time cardiac magnetic resonance imaging. The Annals of thoracic surgery, 101(5), 1818-1825.2. Weiss, E., Rigsby, C., Robinson, J., Baraboo, J., Ma, L., Falcao, M., Roy, C., Stuber, M., & Markl, M (2023). Respiratory Resolved flow in Congenital Heart Disease: A 5D flow MRI Study. Society of Cardiovascular Magnetic Resonance Annual Sessions.3. Ma, L. E., Yerly, J., Piccini, D., Di Sopra, L., Roy, C. W., Carr, J. C., ... & Markl, M. (2020). 5D flow MRI: a fully self-gated, free-running framework for cardiac and respiratory motion–resolved 3D hemodynamics. Radiology: Cardiothoracic Imaging, 2(6).4. Weiss, E., Baraboo, J., Ma, L., Falcao, M., Roy, C., Stuber, M., & Markl, M (2023). Dual Venc 5D flow MRI with Increased Velocity Dynamic Range: An in-vitro and in-vivo Validation and Feasibility Study. ISMRM Annual Meeting.5. Schnell, S., Ansari, S. A., Wu, C., Garcia, J., Murphy, I. G., Rahman, O. A., ... & Markl, M. (2017). Accelerated dual‐venc 4D flow MRI for neurovascular applications. Journal of Magnetic Resonance Imaging, 46(1), 102-114.Figures