4766
The “MR Bra”: Development of a support device for supine breast imaging with commercially available flexible body coils1Nuffield Department of Women's and Reproductive Health, University of Oxford, Oxford, United Kingdom, 2Perspectum Ltd., Oxford, United Kingdom, 3Engineering Science, University of Oxford, Oxford, United Kingdom
Synopsis
Keywords: Breast, Breast, Supine, support
Motivation: Many women find conventional prone breast imaging uncomfortable. We developed a support device (the ‘MR Bra’) to enable supine breast imaging using existing flex coils, without breast compression.
Goal(s): We aimed to evaluate the comfort of the MR bra and asses its SNR performance and structure visualisation capability.
Approach: Two prototypes were developed. Healthy participants were scanned prone with the breast coil and supine using the flex coil and MR bra. The application of negative pressure was assessed with additional imaging.
Results: The MR bra produced reduced, but acceptable, SNR values and improved patient comfort whilst enabling good visualisation of breast tissue structure.
Impact: The MR bra enables comfortable supine breast imaging using readily-available flexible body coils whilst maintaining acceptable SNR values. Negative pressure to elongate the breast structure promises improved tissue visualisation. Further prototype development and evaluation of lesion identification is now underway.
Introduction
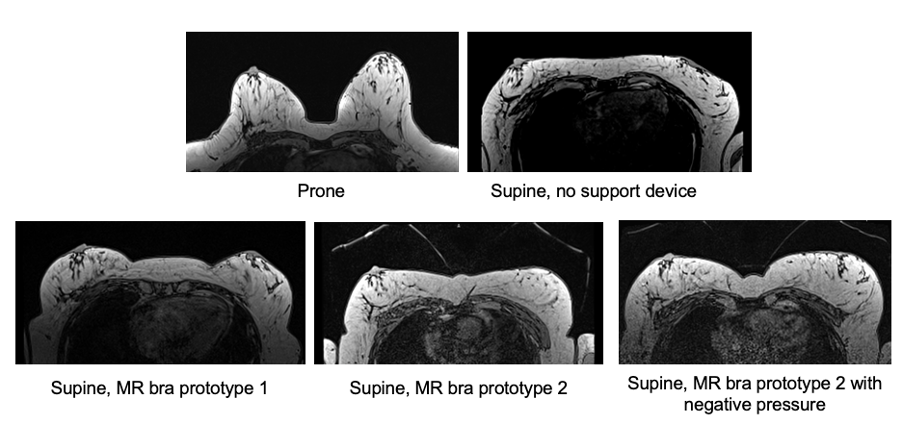
Conventional breast MRI is performed in the prone position with patients’ breasts hanging into a breast-specific RF coil (Figure 1). Breast tissue is elongated from the chest wall, enabling the breast structure to be clearly viewed1. However, the prone position is uncomfortable for many women and inaccessible for those with severe mobility issues2. Moreover, breast-specific coils are only available at a fraction of clinical sites.Supine breast imaging may improve patient comfort and could enable improved image registration to other modalities3, but concerns remain about visualisation of fine structure as the breast is compressed under the weight of the RF coil. Recent development of novel coils for supine breast imaging show excellent results4,5 but clinical implementation necessitates sites to purchase a new coil which are currently limited to 3T.
We developed a support device (the “MR Bra”) for supine breast imaging, designed for use with readily available flexible body (‘flex’) coils. This study assesses the SNR of supine imaging with the MR Bra, reports patient feedback, and provides a preliminary assessment of employing negative pressure on SNR and fine structure visualisation.
Methods
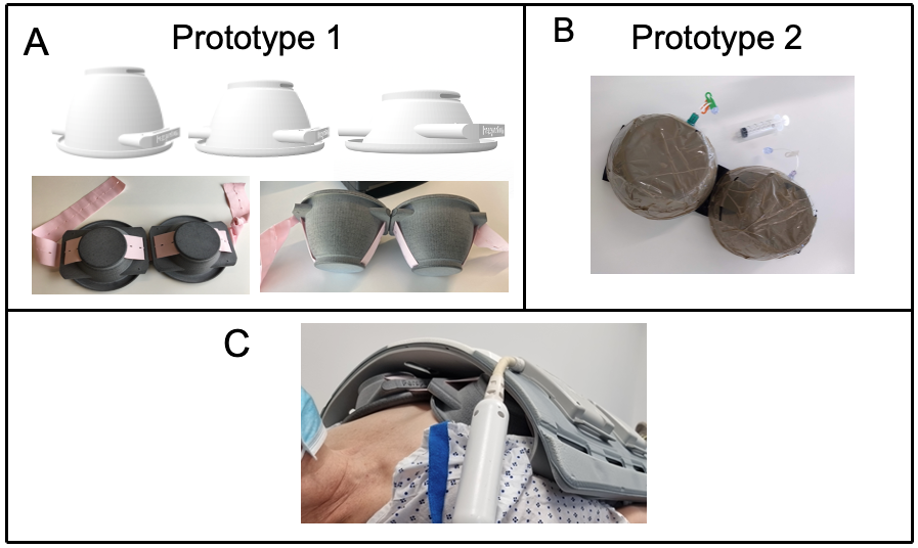
Two prototype support devices were developed (Figure 2). The first prototype consisted of cups designed by a qualified engineer using Autodesk Inventor6 then 3D-printed using hard plastic. Cups were fastened together using an elasticated fabric band, which was changed between scans. Three sizes were developed to account for different breast volumes. A second prototype employed commercially-available plastic structures as cups and incorporated a mechanism for applying negative pressure to pull the breasts away from the chest wall and elongate the breast tissue.Eighteen healthy women (mean age 39 years, range 31-71 years) gave informed consent and were imaged on a Siemens Magnetom Aera 1.5T scanner. Participants were first imaged prone using an 18-channel breast coil (Siemens Healthineers). Participants were then imaged supine with a 6-channel flexible body coil whilst wearing the MR Bra. A 3D axial T1-weighted Dixon scan was performed with the following parameters TE1/TE2/TR = 2.39ms/4.77ms/6.49ms, flip angle 10°, in-plane resolution 1.39x1.39mm2, slice thickness 1.5mm.
SNR was measured using a standard technique7 at a central slice of the T1-weighted images. Participants completed a questionnaire to feedback on the comparative comfort of each scan.
One healthy participant, who previously received a lumpectomy, underwent additional imaging with the flex coil in the supine position (Figure 3). The participant was firstly imaged without a support device and then was imaged with the second prototype MR Bra before and after the application of negative pressure. Two radiologists qualitatively reviewed images of this participant in all five orientations.
Results
Although the mean SNR across 18 participants was significantly lower supine with the MR Bra compared to traditional prone imaging (Wilcoxon signed rank test, p = 2.9e-4), the MR Bra produced good SNR values (Figure 4) which are comparable to those obtained in the prone position in other 1.5T studies3.Supine images of one participant without a support device demonstrated compression of the breast from the weight of the coil, but produced higher SNR than use of the MR bra.
Application of negative pressure to the MR Bra did not affect measurement of SNR (Figure 5). Two radiologists provided positive feedback on visualisation of fine structure with the MR Bra and were able to identify the participant’s lumpectomy scar more easily when a support device was used. The radiologists indicated a preference for the elongated breast shape induced by application of negative pressure.
Several participants identified areas of discomfort during prone scanning. Participant tolerance of supine scanning with the MR bra was generally good, with participants describing the position as 'comfortable' and 'more private'. Of the participants who provided feedback on the comparative comfort of the scans, 82% preferred supine imaging with the MR bra compared to prone imaging.
Discussion
This encouraging patient feedback suggests the MR bra may provide a well-tolerated alternative to conventional prone breast imaging. Review by radiologists suggest that application of negative pressure may provide preferable visualisation of fine structure which is more comparable to traditional prone imaging. Density estimation has previously been shown to have good agreement prone and supine using the MR bra8 – acquisition of acceptable SNR values provides further support for use of this device. Future work should consider the impact of the MR bra upon lesion identification and assess comfort across an older and more diverse population.Conclusion
The MR bra enables comfortable breast imaging with acceptable SNR at 1.5T, and provides a low-cost, easily-implementable solution for supine imaging which may be particularly beneficial for mobility-impaired patients.Acknowledgements
The present work was supported by Perspectum Ltd. and the Royal Commission for the Exhibition of 1851.References
1. Mann R. M., Cho N., Moy L. Breast MRI: atate of the art. Radiology. 2019;292(3):520-526.
2. Agaronnik N.D., El-Jawahri A., Iezzoni L. I. Implications of physics access barriers for breast cancer diagnosis and treatment in women with mobility disability. Journal of Disability Policy Studies. 2021;33(1):46-54.
3. Fausto A., Fanizzi A., Volterrani L., et al. Feasibility, image quality and clinical evaluation of contrast-enhanced breast MRI performed in a supine position compared to the standard prone position. Cancers. 2020;12(9):2364.
4. Nohava L., Obermann M., Frass-Kriegl R. et al. BraCoil – preliminary performance evaluation of a wearable breast coil array for 3T MR mammography. Proc. Intl. Soc. Mag. Reson. Med. 2022;30:2253.
5. Vincent J., Follante C. K., Bayram E. et al. Ultra-flexible, high-resolution, 60-channel RF coil for supine breast imaging. Proc. Intl. Soc. Mag. Reson. Med. 2021;29:1591.
6. Autodesk. Autodesk Inventor: Mechanical design software for ambitious ideas. https://www.autodesk.co.uk/products/inventor/overview, retrieved 8 November 2023.
7. Welvaert M. and Rosseel Y. On the definition of signal-to-noise ratio and contrast-to-noise ratio for fMRI data. PLoS One. 2013;8(11):77089
8. Herlihy A., Tiedeman G., Gordon I. et al. Prone and supine quantitative MRI measurement of breast density: preliminary results from ongoing IMOGEN study. Breast Cancer Research. 2023;25:73.
Figures