4765
The diagnostic potential of magnetic resonance fluoroscopy in patients with achalasia1Tianjin Medical University General Hospital, Tianjin, China, 2Siemens Healthineers, Beijing, China
Synopsis
Keywords: Digestive, Safety, magnetic resonance fluoroscopy;achalasia
Motivation: A non-invasive imaging method, such as MR fluoroscopy, was used for treating achalasia patients.
Goal(s): To determine whether MR fluoroscopy can diagnose patients with achalasia.
Approach: We included 39 achalasia patients and 39 healthy volunteers. MR fluoroscopy was performed to observe the structure of the gastroesophageal junction.
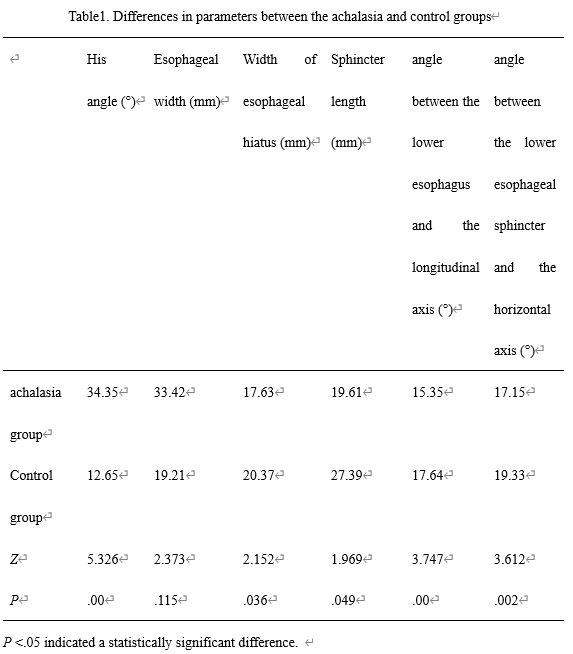
Results: We measured his angle, the esophageal width, the width of esophageal hiatus, the sphincter length, the angle between the lower esophagus and the longitudinal axis, and the angle between the lower esophageal sphincter and horizontal axis. The parameters of the patient group were statistically and significantly different from those of control group.
Impact: MR fluoroscopy can be effectively used in the clinical diagnosis of cardiac achalasia. The MR imaging method is a non-radiological tool and is used to evaluate anatomical structures.
Introduction
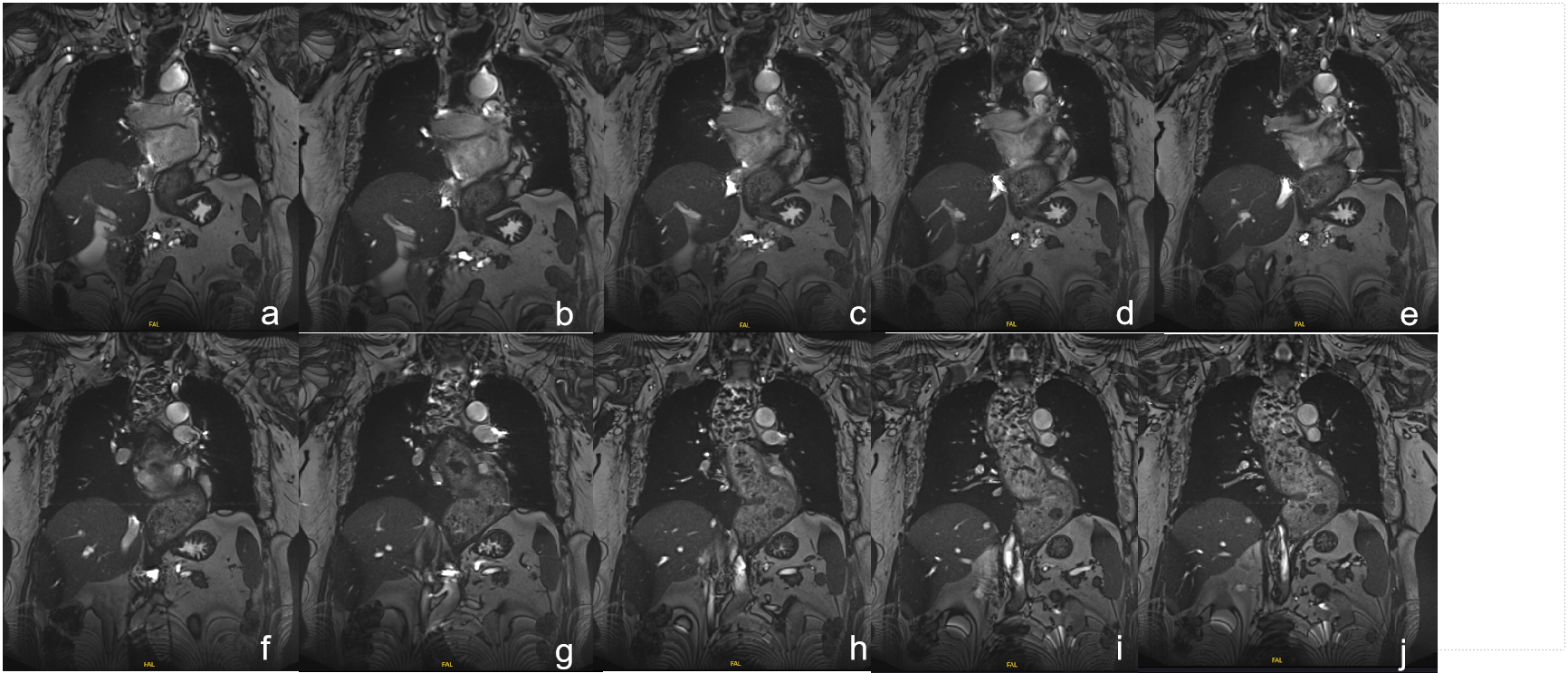
Since achalasia is a neurodegenerative motility disorder of the esophagus. Such a condition causes deranged esophageal peristalsis in patients. Consequently, the lower esophageal sphincter exhibits a loss of function [1]. Currently, a limited number of imaging modalities are used to investigate the esophagus. They are either irradiating the esophagus or restricting the analysis to the esophageal lumen. Magnetic resonance imaging (MRI) is a non-invasive and non-radiating imaging technique [2]. It provides a high degree of soft tissue contrast. The fast MRI sequence is a novel method that enables the morphological and functional assessment of the esophageal body and esophagogastric junction [3]. In this study, our aim is to determine the structure and function of esophagus in patients with achalasia. We explored the feasibility of using a non-invasive imaging method that evaluates patients with achalasia.Methods
In this study, we enrolled 39 achalasia patients(The age of the patients ranged from 28 to 70 years, with an average of 43.09 [Standard deviation (SD) ± 11.26] years), who were clinically diagnosed at our hospital,and the control group consisted of 39 healthy volunteers. All subjects gave written informed consent. To observe the structure of gastroesophageal junction, we performed magnetic resonance fluoroscopy on the participants of this study. The technique was performed on a 3T system (MAGNETOM Skyra, Siemens Healthcare, Erlangen, Germany). The anatomical parameters were estimated through consensus reading. Thereafter, we performed true fast imaging with steady-state precession (TrueFISP): TR = 741 ms; TE = 2 ms; flip angle = 45°; 3 slices; slice thickness = 2.5 mm; distance factor = -30%; FOV = 430 × 430 mm2; measurements = 10; and time resolution = 500 milliseconds. The imaging findings of patients were compared with those of healthy volunteers through SPSS 19.0. The imaging quality was graded by two radiologists (with 15 and 21 years of experience, respectively) according the four-point scale. The inter-reader agreement of the measurements between the 2 readers was assessed using ICC analysis.Results
All the participants were observed by performing MRI TrueFISP. The interobserver agreement was excellent for the following parameters: His angle, the width of the esophagus, the transverse diameter of the esophageal hiatus, the length of the lower esophageal sphincter, the angle between the lower esophagus and the longitudinal axis, and the angle between the lower esophageal sphincter and the horizontal axis. The His angle of the achalasia group was greater than that of the control group, and the difference was statistically significant (Z = 5.326, P <.05). The width of the esophageal and esophageal hiatus of the achalasia group was greater than that of the control group (Z = 2.373, 2.152, P <.05). The esophageal sphincter length of the achalasia group was shorter than that of the control group (Z = 1.969, P <.05). In the experimental group, the angle between the lower esophagus and the longitudinal axis, and the angle between the lower esophageal sphincter and the horizontal axis were different from those of the control group (Z = 3.747, 3.612, P <.05). This difference was found to be statistically significant. (Table 1)Discussion
In this study, we evaluated whether MR fluoroscopy produced reproducible results in the diagnosis of achalasia. The structure and the function of the esophagus undergo transformation in patients with achalasia. The changes seem to be an adaptive response, which is aimed at alleviating unpleasant symptoms. The level of interobserver agreement is high for the various functional parameters. Therefore, the visualization of Esophageal morphology and Angle in patients with achardia by MR fluoroscopy has considerable potential for clinical application in achardia.Conclusion
The imaging parameters may help in the detection of achalasia. The structure and the function were visualized by performing MR fluoroscopy. This novel method has considerable clinical applications in the treatment of achalasia.Acknowledgements
I would like to express my gratitude to all those who helped me during the writing of this thesis.References
[1] O'Neill OM, Johnston BT, Coleman HG. Achalasia: A review of clinical diagnosis, epidemiology, treatment and outcomes. World J Gastroenterol. 2013,21;19(35):5806-5812. Doi: 10.3748/wjg.v19.i35.5806.
[2] Leandri C, Soyer P, Oudjit A, et al. Contribution of magnetic resonance imaging to the management of esophageal diseases: A systematic review. Eur J Radiol. 2019, 120:108684. Doi: 10.1016/j.ejrad.2019.108684.
[3] Lee SL, Yadav P, Starekova J, et al. Diagnostic Performance of MRI for Esophageal Carcinoma: A Systematic Review and Meta-Analysis. Radiology. 2021,299(3):583-594. Doi: 10.1148/radiol.2021202857.
Figures