4764
Renal MRI Assessment of the Effects of High-Water Intake on Total Kidney Volume Growth in ADPKD1Radiology, Weill Cornell Medicine, New York, NY, United States, 2Medicine, Weill Cornell Medicine, New York, NY, United States, 3The Rogosin Institute, New York, NY, United States, 4School of Electrical and Computer Engineering, Cornell University and Cornell Tech, New York, NY, United States, 5Radiology, Columbia College of Physicians and Surgeons, New York, NY, United States
Synopsis
Keywords: Kidney, Kidney, ADPKD, CKD
Motivation: By measuring height-adjusted total kidney volume (ht-TKV), renal MRI monitors autosomal dominant polycystic kidney disease (ADPKD) progression and evaluates therapeutic interventions’ efficacy for slowing cyst growth.
Goal(s): Since arginine vasopressin (AVP) stimulates cyst growth, reducing vasopressin with high-water intake (HWI) may slow ADPKD progression.
Approach: We test this hypothesis using a case-crossover study with 7 ADPKD subjects, measuring ht-TKV changes on MRI during usual and high-water intake.
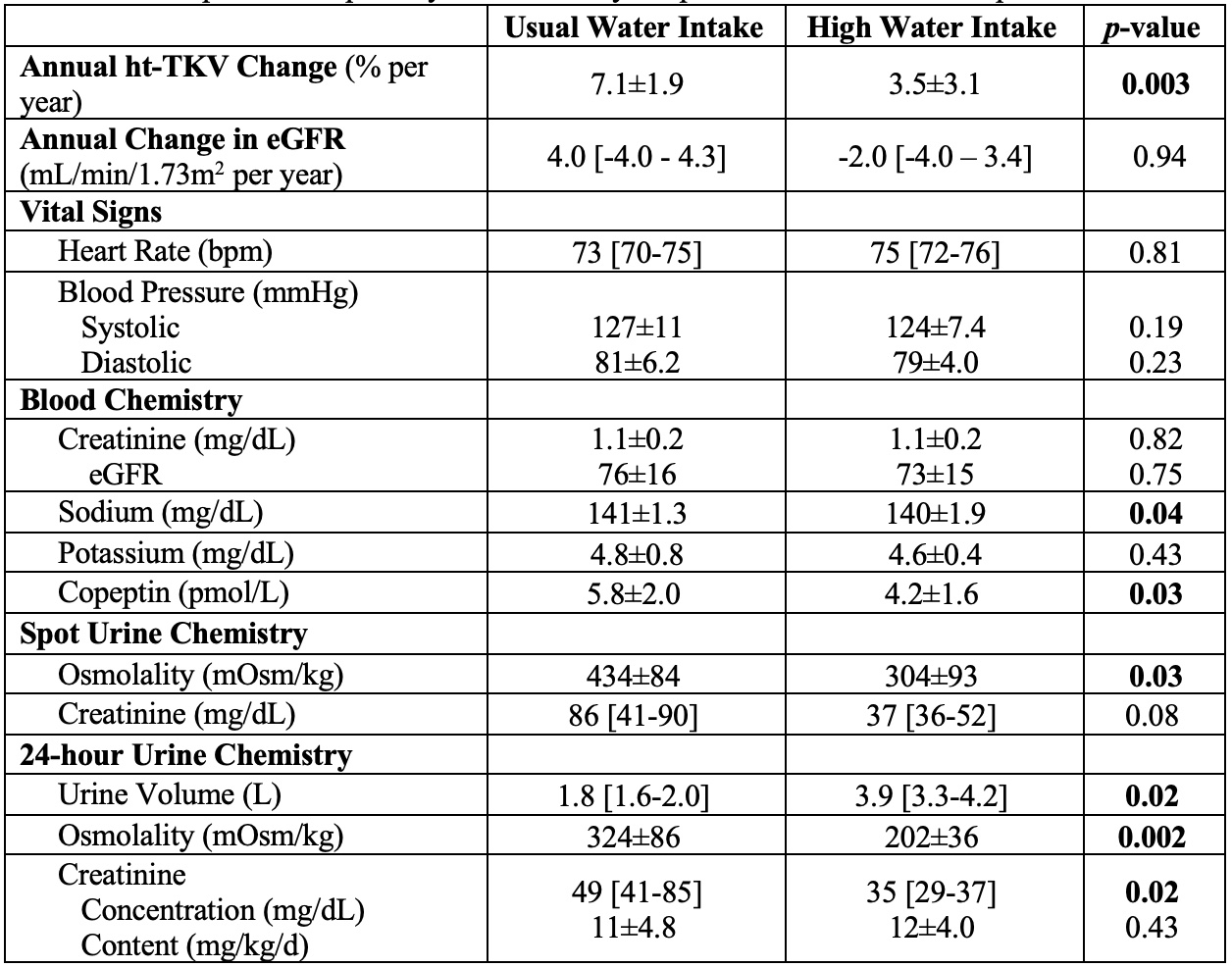
Results: High-water intake decreased 24-hour urine osmolality (359 vs 202mOsm/kg, p=0.002) and rate of increase in annualized ht-TKV growth rate (7.1% vs 3.5%, p=0.003), suggesting that high-water intake can slow ADPKD progression.
Impact: Decreasing the rate of ht-TKV increase, measured by renal MRI during high water intake, suggests this as a potential treatment to slow progression of ADPKD, forestalling end-stage kidney failure requiring dialysis or transplantation.
Introduction
ADPKD is characterized by proliferation of renal tubular epithelium and secretion of fluid into kidney cysts, which are stimulated by arginine vasopressin (AVP) via the type 2 vasopressin receptor.1 In ADPKD patients, increased AVP release compensates for impaired renal concentrating ability, elevating cAMP levels.2 Tolvaptan, a V2R antagonist, is an FDA-approved treatment for ADPKD to slow cyst growth and progression of chronic kidney disease.3 However, tolvaptan use is limited by high cost, aquaretic side effects and hepatotoxicity.4 Suppressing vasopressin by high water intake has been proposed as an alternative to tolvaptan. A randomized control trial of high-water intake showed no benefit in ADPKD patients, but the findings may have been confounded by inadequate compliance to HWI and ht-TKV measurement reproducibility on MRI.5 The current study obtained ht-TKV measurements at 5 timepoints using MRI pulse sequence(s) with minimal acquisition error to reliably determine the effect of high water intake on cyst growth and assess ADPKD progression.Methods
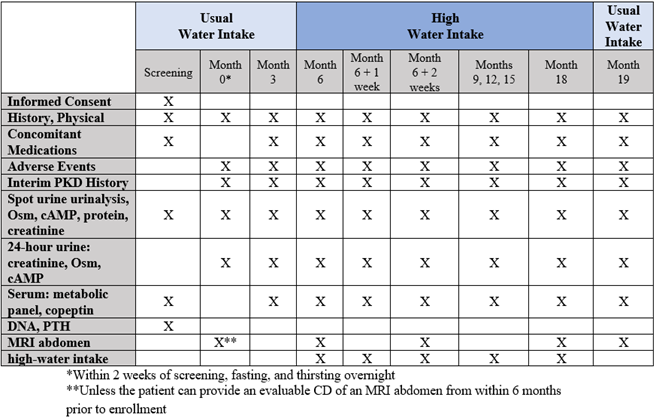
In this time-series case-crossover trial, 7 ADPKD subjects had ad libitum, usual water intake (UWI) for 6 months, followed by HWI for 12 months. Each subject had individualized prescribed water intake amount designed to maintain urine osmolality below serum osmolality (285 mOsm/kg).6 An initial volumetric MRI established the UWI baseline ht-TKV, using sequences that had no acquisition errors. Subsequent MRI scans were acquired at specific intervals: 6-month, 6-month + 2-week, 18-month and 19-month timepoints, for further volumetric analyses. To assess subject compliance to water intake protocol, a “smart” water bottle was given to each subject at their 6-month visit. During each scheduled visit, adverse events were recorded, and 24-hour urine samples were collected to determine if these markers were associated with the ht-TKV pattern measured on MRI (Fig. 1) utilizing 5 pulse sequences (axial 3D T1 SPGR, axial and coronal T2 single-shot fast spin echo, axial and coronal steady-state free precession) obtained during breath-holding.7 Kidneys were segmented using a semi-automated 3D deep learning-assisted technique, including an outlier analysis to eliminate sequences corrupted by motion and other artifacts.8 Copeptin is secreted in an equimolar amount to vasopressin and is more easily measured as a AVP level marker.7Results
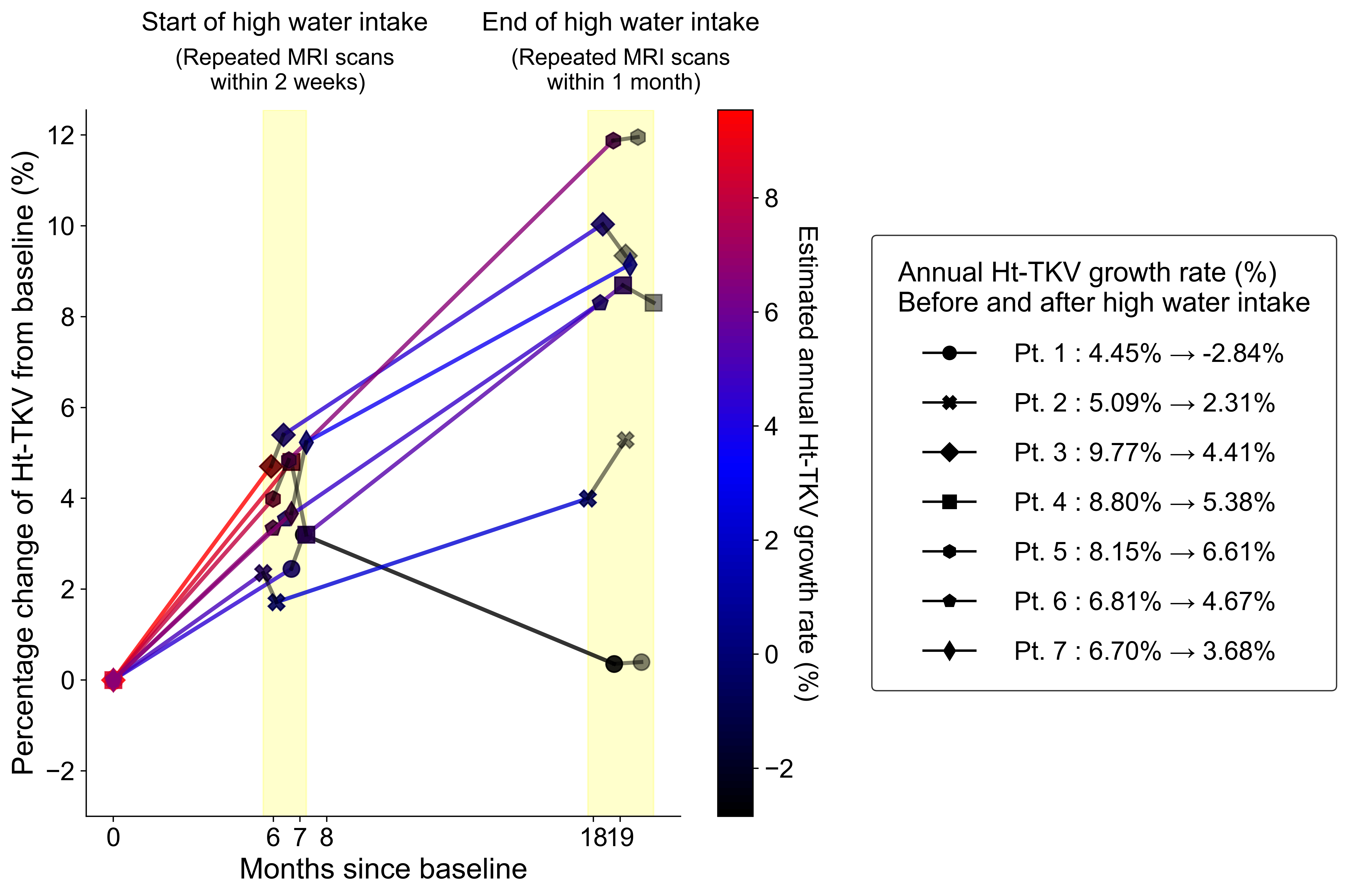
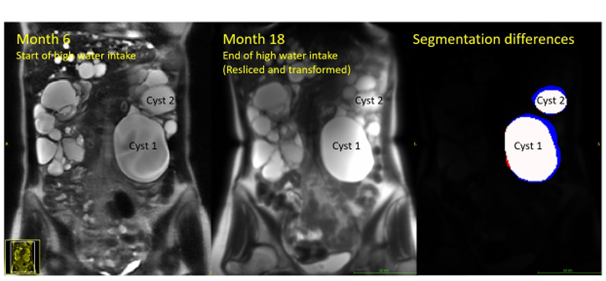
All subjects completed the 5 MRI scans tracking ht-TKV on UWI and HWI schedules, and all reached the target 24-hour urine osmolality (<285 mOsm/kg) on HWI, with a net 2.1L increase in 24-hour urine volume from their baseline level (p=0.02), confirming their compliance with the protocol. Serum copeptin levels decreased by 28% (ad libitum 5.8 to high-water intake 4.2pmol/L, p=0.03), indicating a decrease in AVP level.The annualized ht-TKV growth rate measured by renal MRI decreased by 50%, from 7.1% on UWI to 3.5% during HWI (p=0.003) (Fig. 2). Results were similar when analyzing individual MRI pulse sequences for the volumetric analysis, as compared to averaging all available sequences (Fig. 3). The maximum reduction was observed in a patient at high risk for rapid progression of ADPKD (Mayo Class 1D), whose annualized ht-TKV decreased from 4.4% during UWI to 2.8% on high water intake. Further analysis of the images showed that individual cysts became smaller in this patient, consistent with the conclusion that ht-TKV decreased during usual water intake (Fig. 4). During the transition periods after changes in water intake (Month 6+2 weeks and Month 19), there were changes in ht-TKV.
There were no significant adverse events during HWI. One subject required hospitalization due to a ruptured cyst hemorrhage during UWI.
Discussion
This crossover study with 7 ADPKD patients at moderate to high risk of disease progression showed that HWI significantly reduced the annualized rate of ht-TKV growth by ~50%. Plasma copeptin levels decreased during HWI, indicating reduced vasopressin levels.9 Unlike previous studies, our HWI trial determined the efficacy of the regimen on cyst growth in ADPKD using MRI methodologies and image processing algorithms that analyze all available pulse sequences and include an outlier analysis to obtain ht-TKV values with low variability, ensuring precise and reliable results.The study findings demonstrate the feasibility of using renal MRI to assess the efficacy of a high-water intake regimen on reducing cyst growth in ADPKD patients. Strengths of this study include the cross-over design, precise and reproducible MRI protocols for assessing TKV, and high compliance with the water intake prescriptions. Limitations of this study include the small sample size, lack of randomization of the order of water intake prescriptions, and relative short duration of the study.
Conclusion
Renal MRI tracks kidney volumes in ADPKD demonstrating slower disease progression during high water intake diet, which suppresses vasopressin release from the posterior pituitary gland.Acknowledgements
No acknowledgement found.References
1. Chebib FT, Torres VE. Autosomal Dominant Polycystic Kidney Disease: Core Curriculum 2016. Am J Kidney Dis. May 2016;67(5):792-810. doi:10.1053/j.ajkd.2015.07.0372. Zhou X, Torres VE. Emerging therapies for autosomal dominant polycystic kidney disease with a focus on cAMP signaling. Front Mol Biosci. 2022;9:981963. doi:10.3389/fmolb.2022.981963
3. Torres VE, Chapman AB, Devuyst O, et al. Tolvaptan in Patients with Autosomal Dominant Polycystic Kidney Disease. New England Journal of Medicine. 2012;367(25):2407-2418. doi:10.1056/nejmoa1205511
4. Müller RU, Messchendorp AL, Birn H, et al. An update on the use of tolvaptan for autosomal dominant polycystic kidney disease: consensus statement on behalf of the ERA Working Group on Inherited Kidney Disorders, the European Rare Kidney Disease Reference Network and Polycystic Kidney Disease International. Nephrol Dial Transplant. Apr 25 2022;37(5):825-839. doi:10.1093/ndt/gfab312
5. Rangan GK, Wong ATY, Munt A, et al. Prescribed Water Intake in Autosomal Dominant Polycystic Kidney Disease. NEJM Evidence. 2022;1(1):EVIDoa2100021. doi:doi:10.1056/EVIDoa2100021
6. Grantham JJ. Therapy for Polycystic Kidney Disease? It's Water, Stupid! Journal of the American Society of Nephrology. 2008;19(1):1-7. doi:10.1681/asn.2007101100
7. Christ-Crain M. Vasopressin and Copeptin in health and disease. Reviews in Endocrine and Metabolic Disorders. 2019/09/01 2019;20(3):283-294. doi:10.1007/s11154-019-09509-9
8. He X, Hu Z, Dev H, et al. Test Retest Reproducibility of Organ Volume Measurements in ADPKD Using 3D Multimodality Deep Learning. Acad Radiol. 2023/10/03/ 2023;doi:https://doi.org/10.1016/j.acra.2023.09.009
Figures