4761
Repeatability of Standalone versus Image-Acquisition-Integrated 129Xe Spectroscopy1Tanwei College, Tsinghua University, Beijing, China, 2Department of Radiology, Duke University, Durham, NC, United States, 3Department of Radiology & Medical Imaging, Charlottesville, VA, United States
Synopsis
Keywords: Lung, Hyperpolarized MR (Gas)
Motivation: 129Xe spectral parameters of lung airspaces, membrane tissues and red blood cells (RBC), provided by an MRS calibration scan, are important indicators of gas exchange function.
Goal(s): Currently, such spectra are often acquired separately from gas exchange images, but it may be feasible to integrate 129Xe gas-exchange MRI and MRS into one scan, and test its repeatability.
Approach: In this study, we assess the performance of image-acquisition-integrated spectra and compare them with a dedicated spectroscopicacquisition.
Results: In subjects with a range of diseases, image-acquisition-integrated spectra were less repeatable than dedicated ones. However, increasing the number of averaged FIDS to 1second may yield equivalent performance.
Impact: The repeatability of 129Xe spectroscopy integrated with imaging would be improved by collecting and averaging at least 1 second of data.
Introduction
129Xe magnetic resonance spectroscopy provides useful quantitative metrics for assessing gas exchange by characterizing signals originating from the lung air spaces, uptake in membrane tissues (M), and transfer to red blood cells (RBCs)1. The resulting RBC/M ratio and RBC chemical shift are biomarkers of gas exchange efficiency and blood oxygen saturation, respectively (Figure1). RBC/M has emerged as one of the most sensitive and repeatable markers for detecting impaired gas exchange, disease progression, and therapy response2,3,4, and is also vital for 1-point Dixon image decomposition. The RBC shift is indicative of mean capillary blood oxygenation and is reduced in most lung diseases5. Although typical 129Xe protocols involve separate breath-hold doses for calibration/spectroscopy and Dixon-based gas exchange imaging6, there is a growing interest in consolidating these steps into a single breath-hold scan. Recent research demonstrated the feasibility of acquiring ventilation, gas-exchange imaging, and anatomy within a one breath-hold exam7. Although this work obtained RBC/M from a separate calibration scan, it is logical to also add spectroscopy, to achieve a full exam in one breath-hold. However, this must necessarily be limited to only a few spectroscopic frames to minimize breath-hold duration. Here, we sought to evaluate differences between image-acquisition-integrated and separately acquired spectra, assess their repeatability, and estimate the number of averages to optimize repeatability.Methods
Dedicated 129Xe spectra were acquired according to consortium guidelines (500 spectra, TR=15ms, a=20˚)6,7. Image-acquisition-integrated spectra were acquired by appending 10 dissolved-phase acquisitions (same TR and flip angle) to consortium-standard Dixon-based gas-exchange imaging. Dedicated spectra were analyzed by averaging 1 second of data (67 frames), whereas the integrated spectra simply averaged the 10 available frames. All spectra were processed using time-domain fitting8 (MATLAB) to evaluate RBC/M and RBC shift. We used 3 data sets to assess agreement between and repeatability of the dedicated versus image-integrated spectroscopy. Agreement was evaluated using 161 scan pairs of dedicated and image-integrated spectra acquired in the same subjects. Repeatability of dedicated spectroscopy and image-integrated spectroscopy was evaluated from 37 pairs of each. An additional 145 pairs of dedicated spectroscopy data were used to determine the number of averages needed to achieve optimal repeatability.Comparisons between scans and repeatability were evaluated using Bland-Altman plots and quantified by the coefficient of repeatability (CR), and intra-class correlation coefficient (ICC) as defined below:
$$\begin{gathered}C R=1.96 \times S D\left(\operatorname{scan}_1-\operatorname{scan}_2\right) \\I C C=\frac{M S B S-M S W S}{M S B S+(k-1) M S W S}\end{gathered}$$
Here MSBS is the mean-square between subjects, MSWS is the mean-square within subjects, and k is the number of repeated scans per subject9.
Results
Comparison of dedicated and integrated spectra (Figure 2) revealed only modest limits of agreement, although the bias was close to 0 for both RBC/M and RBC shift. The repeatability of the dedicated spectra was substantially better than that of the integrated spectra (Figure 3). The ICC of RBC/M was higher than that of the RBC shift for almost all scenarios. However, when averaging of dedicated spectra was reduced to 10 frames, the repeatability also worsened (Figure 4). Expanding the number of scan pairs improved the confidence of the repeatability. Intra-class correlation coefficient and coefficient of repeatability are optimal when using 145 scan pairs and 67 averages. Using 145 pairs of dedicated spectra and 1 sec of averaging yielded CRs of 0.078 and 0.42 for RBC/M and RBC shift, respectively. When averaging is reduced from 67 to only 10, both worsen. Using these pairs to test the effect of averaging (Figure 5) revealed that 10 or fewer averages decreased repeatability and 1.1 sec of averaging was optimal.Discussion
The relatively broad limits of agreement between dedicated and integrated spectra, coupled with the superior repeatability of dedicated spectra, suggests that the number of averages plays a significant role. Indeed, a careful study of repeatability as a function of averages showed that, at around 10 averages or fewer, repeatability worsens. The repeatability of spectral parameters appears to be optimal when averaging is increased to about 1.1s, or 73 frames. Note, however, that integrated spectra may still suffer from being appended at the end of a breath-hold scan, and, if patients cannot hold their breath for the duration, an erroneous spectrum may be collected. Nonetheless, the current work suggests that if sufficient averages are collected, it may be feasible to establish a fully integrated exam of functional and anatomical imaging with spectroscopy.Acknowledgements
No acknowledgement found.References
1. Kaushik S.S., Robertson S.H., Freeman M.S., et al. Single-breath clinical imaging of hyperpolarized 129Xe in the airspaces, barrier, and red blood cells using an interleaved 3D radial 1-point Dixon acquisition. Magn Reson Med 75, 1434–1443 (2016)
2. Weatherley N.D. et al., Hyperpolarised xenon magnetic resonance spectroscopy for the longitudinal assessment of changes in gas diffusion in IPF. Thorax May 74, 500-502 (2019)
3. Matheson, A., et al. Persistent 129Xe MRI Pulmonary and CT Vascular Abnormalities in Symptomatic Individuals with Post-Acute COVID-19 Syndrome. Radiology 305, 466-476 (2022)
4. Marshall, H., et al. 129Xe and Free-Breathing 1H Ventilation MRI in Patients With Cystic Fibrosis: A Dual-Center Study. JMRI June 57, 1908-1921 (2023)
5. Norquay G. et al., 129Xe chemical shift in human blood and pulmonary blood oxygenation measurement in humans using hyperpolarized 129Xe NMR. Magn Reson Med 77,1399-1408 (2017)
6. Niedbalski, P. J. et al. Protocols for multi-site trials using hyperpolarized 129Xe MRI for imaging of ventilation, alveolar-airspace size, and gas exchange: A position paper from the 129Xe MRI clinical trials consortium. Magn Reson Med 86, 2966–2986 (2021)
7. Niedbalski, P. J. et al. A single-breath-hold protocol for hyperpolarized 129Xe ventilation and gas exchange imaging. NMR Biomed. 36, e4923 (2023)
8. Bier, E. A. et al. A protocol for quantifying cardiogenic oscillations in dynamic 129Xe gas exchange spectroscopy: The effects of idiopathic pulmonary fibrosis. NMR Biomed 32, (2019).
9. Bechtel, A. et al. Repeatability of pulmonary 129Xe static spectroscopy and dynamic spectroscopy fit methods: a reader study in ISMRM 2021 Annual Meeting and Exhibition (2023)
Figures
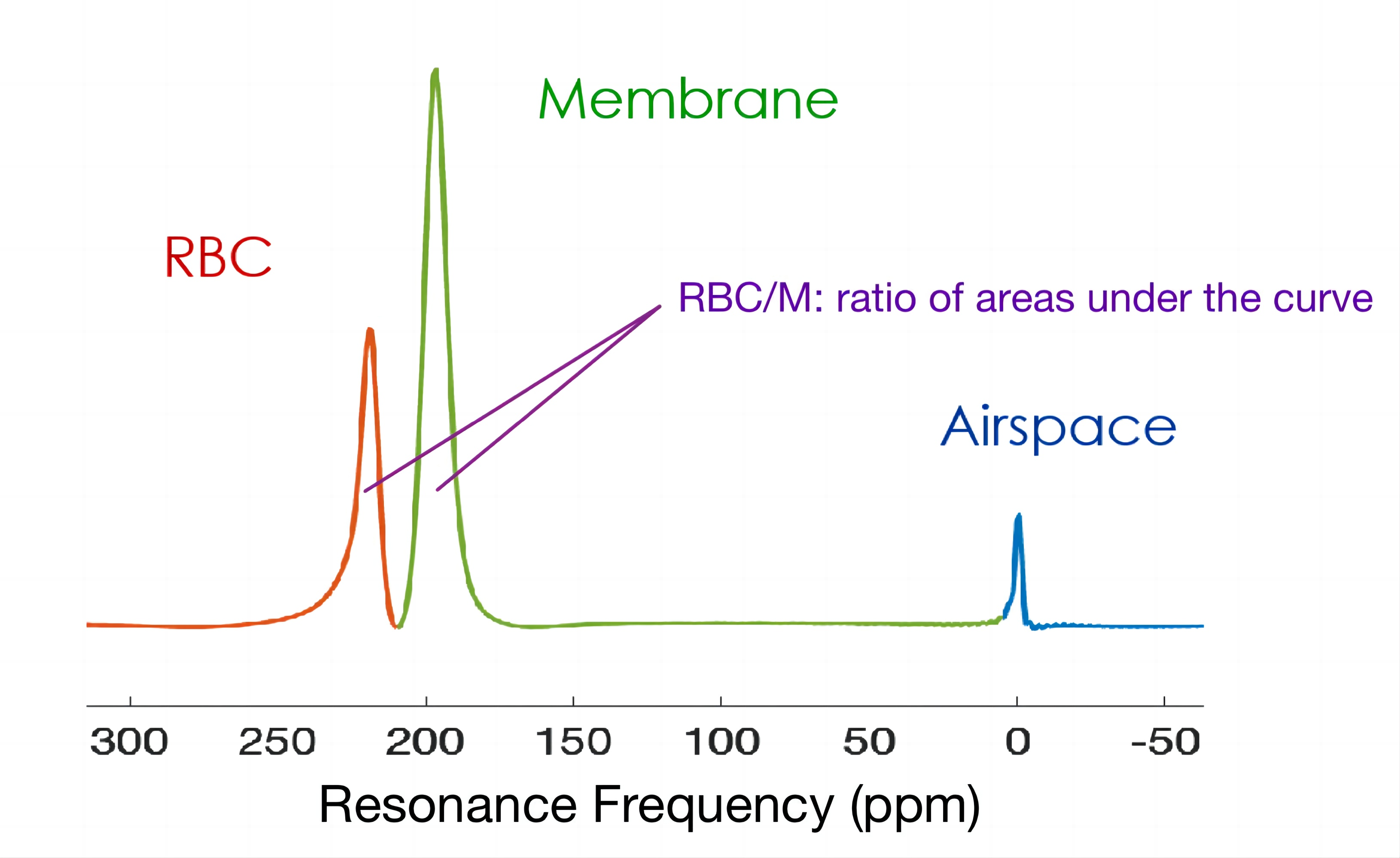
Figure 1. Representative phased 129Xe spectrum showing the RBC and membrane resonances. RBC/M ratio refers to the ratio of areas under the curve, and RBC chemical shift is measured relative to the airspace peak.
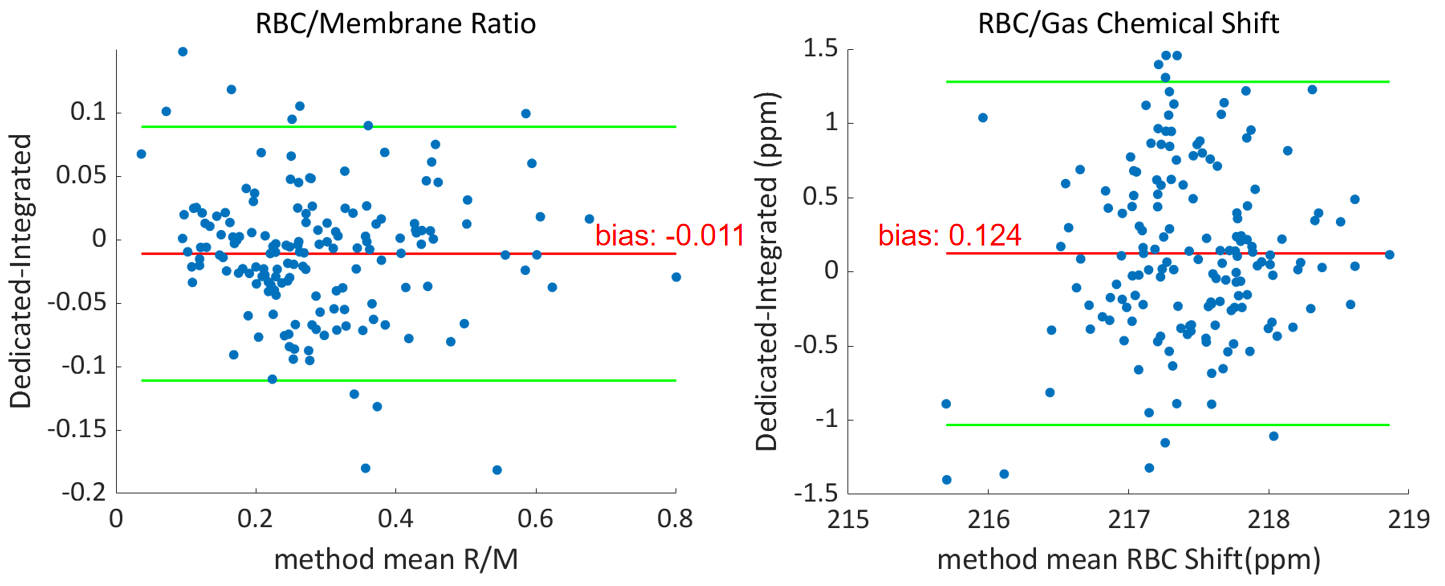
Figure 2. Bland-Altman plots comparing the level of agreement for RBC/M and RBC frequency shift between dedicated vs integrated spectra. The bias (labeled in the graph in red) for both RBC/M and RBC shift is nearly negligible between the methods. However, the limits of agreement between the two methods are much broader than published repeatability metrics.
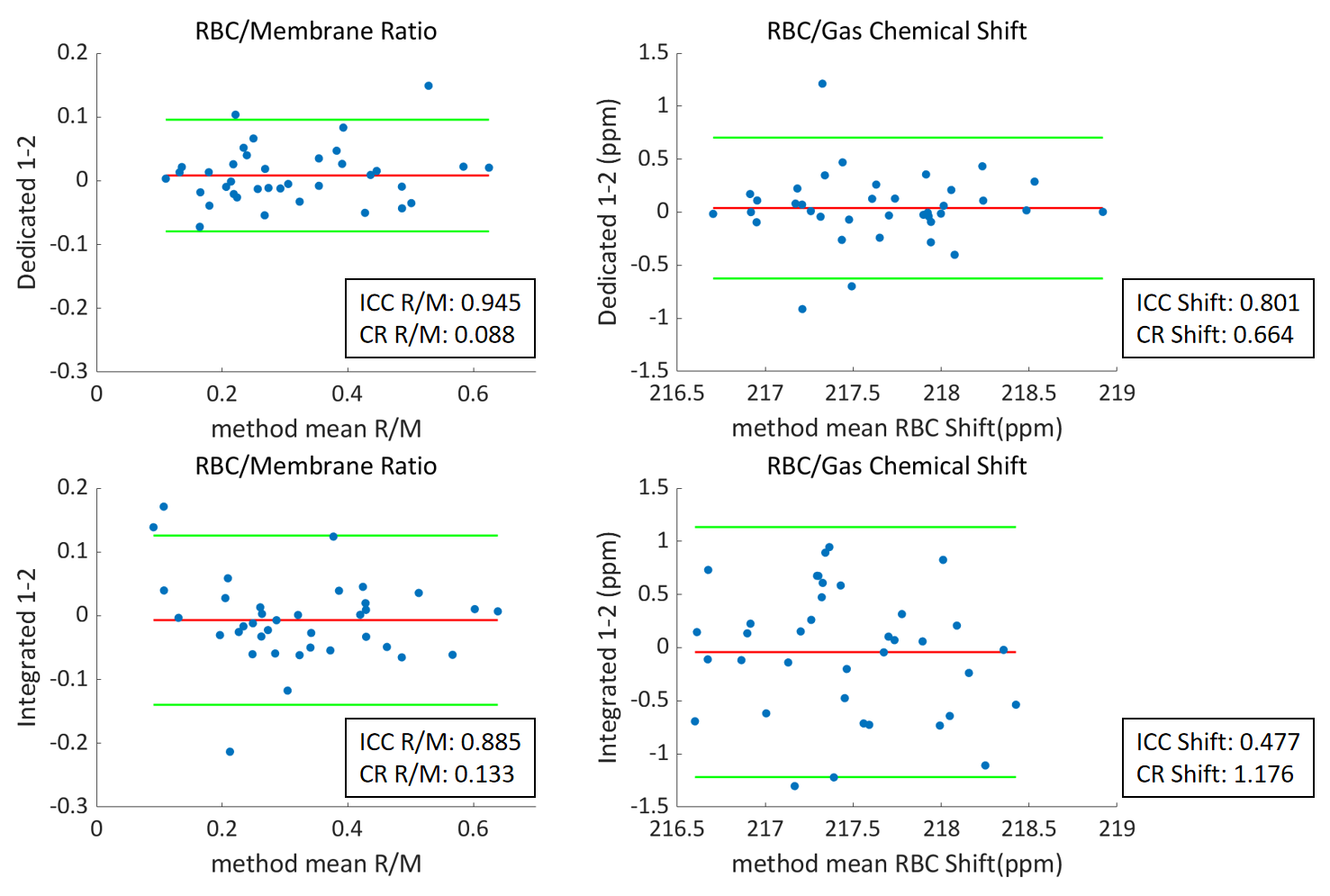
Figure 3. Bland-Altman plots showing repeatability of RBC/M and RBC chemical shift for dedicated spectroscopy(top) vs image-integrated spectroscopy (bottom) acquired from 37 pairs of scans for each. The ICC and CR for each parameter are labeled beside each plot. The repeatability of the dedicated spectra is considerably higher than that of the image-integrated ones.
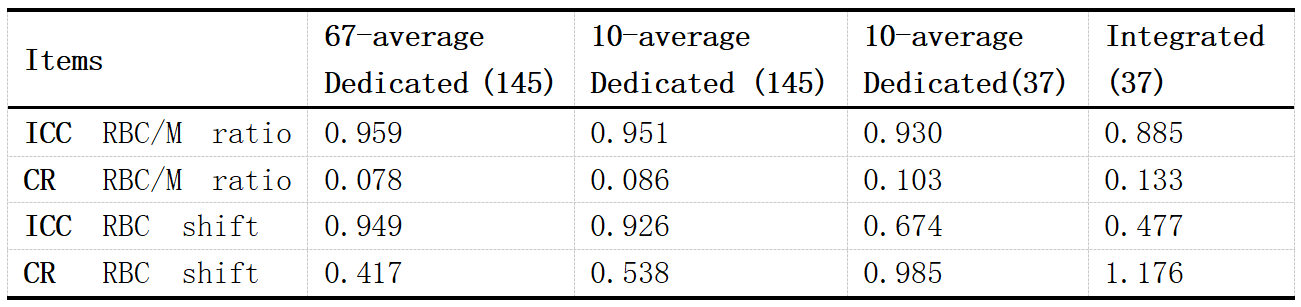
Figure 4. Effects of reducing the number of scan pairs or averages on the repeatability of dedicated spectra. Intra-class correlation coefficient and coefficient of repeatability are optimal when using 145 scan pairs and 67 averages. When averaging is reduced from 67 to only 10, both worsen. And when the number of scan pairs is reduced to 37, the ICC and CR worsen to a level that nearly matches that of the integrated method.
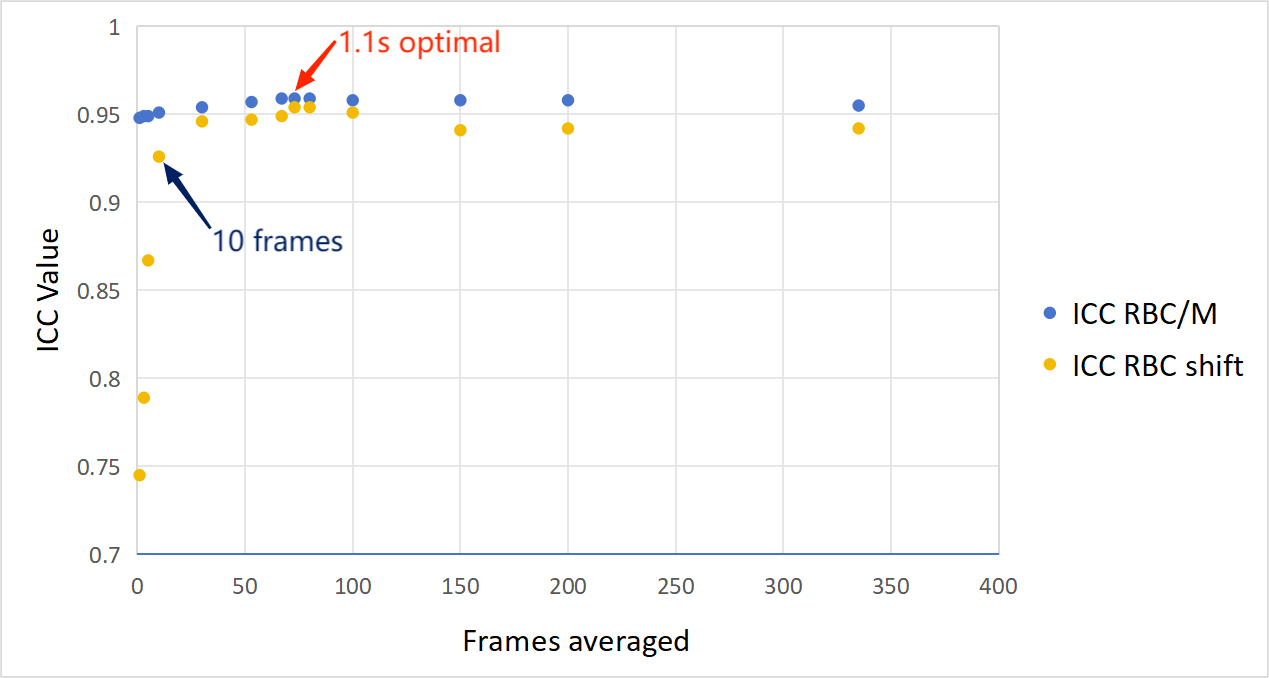
Figure 5. (a) Visualized relationship between ICC and the number of the frames averaged for both RBC/M and RBC shift. Particularly, the ICC for RBC shift decreases substantially at 10 frames, while 73 frames, or 1.1s of averaging, appears optimal.