4759
Functional lung imaging with ultrashort echo times achieved by half pulses1Medical Physics Group, University Clinic and Outpatient Clinic for Radiology, University Hospital Halle (Saale), Halle (Saale), Germany, 2Halle MR Imaging Core Facility, Medical Faculty, Martin-Luther-University Halle-Wittenberg, Halle (Saale), Germany, 3Department of Diagnostic and Interventional Radiology, University Hospital Wuerzburg, Wuerzburg, Germany
Synopsis
Keywords: Lung, Lung
Motivation: While ventilation and perfusion mapping in lung can be realized by Cartesian imaging, low signal intensities, due to rapid relaxation, remain challenging and ultrashort echo times might improve robustness. Currently, the promising approach of half pulse excitation for 2D-UTE imaging was not yet employed for functional lung imaging.
Goal(s): To evaluate the suitability of half pulse excitation for functional lung imaging.
Approach: Functional lung imaging was performed in a healthy volunteer by radial acquisitions after sinc or half pulse excitation.
Results: Complex sum of two half pulse acquisitions provides morphological depiction of lung tissue and ventilation maps, but no information on lung perfusion.
Impact: The use of half pulses for functional lung imaging did not provide an improvement, as no information on perfusion can be gained. Therefore, other approaches are necessary to improve robustness in the detection of pathologies characterized by ventilation-perfusion mismatches.
Introduction
MR imaging of the lung is very challenging but of high interest for functional analysis, especially in pediatric patients or to monitor chronic lung diseases1–3. Main challenges lie in the low proton density and the ultra-short relaxation times. To overcome the latter, acquisitions with ultrashort echo times (UTE) can be employed. Lung pathologies can be characterized by ventilation or perfusion defects, e.g. Asthma or COPD, and might be distinguished by deficit patters in one or both parameters. In some pathologies, location and extent, especially of ventilation-perfusion mismatches, can be of interest for treatment or outcome, e.g. mucus plugs in cystic fibrosis or lung embolisms.In 2D acquisitions, which are required for perfusion imaging, ultra-short echo times can be achieved, for example, by a half pulse excitation4,5.
The aim of this study is to evaluate the suitability of a half pulse excitation for SElf-gated Non-Contrast-Enhanced FUnctional Lung imaging (SENCEFUL)6.
Methods
Coronal 2D measurements of the lungs were performed in a healthy volunteer on a 3T-MRI (Siemens MAGNETOM PrismaFit).First, a spoiled gradient echo acquisition, featuring a sinc-shaped excitation pulse and a centre-out golden angle radial readout trajectory, was conducted as reference. A second and third measurement featured the same trajectory but used a half-sinc excitation pulse. These two measurements differed by an opposing polarity of the slice selection gradient. Slice profile measurements were conducted by shifting the readout gradient onto the slice selection axis. Figure 1 sketches main sequence features and provides an overview of all acquisition parameters.
For all acquisitions the temporal data was retrospectively gated into 30 respiratory and 21 cardiac phases using the DC signal. Located in the center of k-space the DC signal is intrinsically covered by each radial readout. Image reconstruction was performed by gridding using GROG and subsequent 2D Fourier transform. Additionally, a fourth set of images was created by adding the complex data of each cardiac/respiratory bin for the two half pulse measurements with opposing gradient directions.
Functional parameter maps were determined using the standard SENCEFUL algorithm6.
Results
Figure 2 shows measured slice profiles for all excitation pulses used in this study, as well as the profile derived by complex addition of the half pulse slice profiles at opposing gradient directions. In contrast to the standard sinc pulse (FWHM=9.5mm, FWTM=17.1mm), half pulses (FWHM= 13.3mm, FWTM=47.5mm) clearly show an extended excitation area with an increased FWHM (full width at half maximum) and even more strongly enlarged FWTM (full width at tenth of maximum), whereas a sharp profile can be derived from the complex sum combination (FWHM=7.6mm, FWTM=13.3mm).Morphological images of the healthy volunteer (Figure 3 top row) confirm this effect. From the radial sinc pulse acquisition, smooth ventilation maps can be reconstructed by the standard SENCEFUL algorithm (Figure 3 center row). For each of the half pulse acquisitions, ventilation cannot be quantified using the standard algorithm. Nevertheless, combination of these two acquisitions can provide robust ventilation maps.
Likewise, a perfusion map is available from the acquisition with sinc pulse excitation (Figure 3 bottom row). No information about perfusion can be obtained with a half pulse excitation, neither by each individual recording nor by their combination.
Discussion
Employing a radial trajectory allows for short echo times and provides further general advantages for functional lung imaging, like robustness towards motion and the intrinsic acquisition of the DC-signal in each readout. In contrast to the more common 3D approach for UTE, the standard 2D acquisition allows to gain perfusion information.Further reduction of echo times can be achieved by using a half pulse excitation. Morphological imaging as well as ventilation quantification is feasible when two measurements with opposing slice selection gradient directions are performed and the complex sum combination is evaluated. The ventilation information relies on signal intensity changes due to expansion and compression of the lung tissue within a given volume and can therefore be restored by such a combination. In contrast, the perfusion information is based on the inflow effect and is therefore directly dependent on the excitation slice profile. Thus, the extensive width of the slice profile in each half pulse excitation eliminates the effect already during the acquisition. Consequently, the perfusion information is lost and cannot be restored.
Conclusion
Half pulse excitation can help to shorten echo times in 2D acquisitions. This approach is beneficial for morphological imaging of the lung and ventilation mapping but cannot provide the perfusion information contained in standard 2D acquisitions with full sinc pulses.Acknowledgements
No acknowledgement found.References
1. Hirsch FW, Sorge I, Vogel-Claussen J, et al. The current status and further prospects for lung magnetic resonance imaging in pediatric radiology. Pediatr Radiol. 2020;50(5):734-749. doi:10.1007/s00247-019-04594-z
2. Serai SD, Rapp JB, States LJ, Andronikou S, Ciet P, Lee EY. Pediatric Lung MRI: Currently Available and Emerging Techniques. American Journal of Roentgenology. 2021;216(3):781-790. doi:10.2214/AJR.20.23104
3. Voskrebenzev A, Vogel-Claussen J. Proton MRI of the Lung: How to Tame Scarce Protons and Fast Signal Decay. Journal of Magnetic Resonance Imaging. 2021;53(5):1344-1357. doi:10.1002/jmri.27122
4. Pauly JM. Selective Excitation for Ultrashort Echo Time Imaging. eMagRes. 2012;1(2). doi:10.1002/9780470034590.emrstm1271
5. Manhard MK, Harkins KD, Gochberg DF, Nyman JS, Does MD. 30-Second bound and pore water concentration mapping of cortical bone using 2D UTE with optimized half-pulses. Magnetic Resonance in Medicine. 2017;77(3):945-950. doi:10.1002/mrm.26605
6. Fischer A, Weick S, Ritter CO, et al. SElf-gated Non-Contrast-Enhanced FUnctional Lung imaging (SENCEFUL) using a quasi-random fast low-angle shot (FLASH) sequence and proton MRI. NMR in Biomedicine. 2014;27(8):907-917. doi:10.1002/nbm.3134
7. Josan S, Pauly JM, Daniel BL, Pauly KB. Double half RF pulses for reduced sensitivity to eddy currents in UTE imaging. Magnetic Resonance in Medicine. 2009;61(5):1083-1089. doi:10.1002/mrm.21879
8. Conolly S, Nishimura D, Macovski A, Glover G. Variable-rate selective excitation. Journal of Magnetic Resonance (1969). 1988;78(3):440-458. doi:10.1016/0022-2364(88)90131-X
Figures
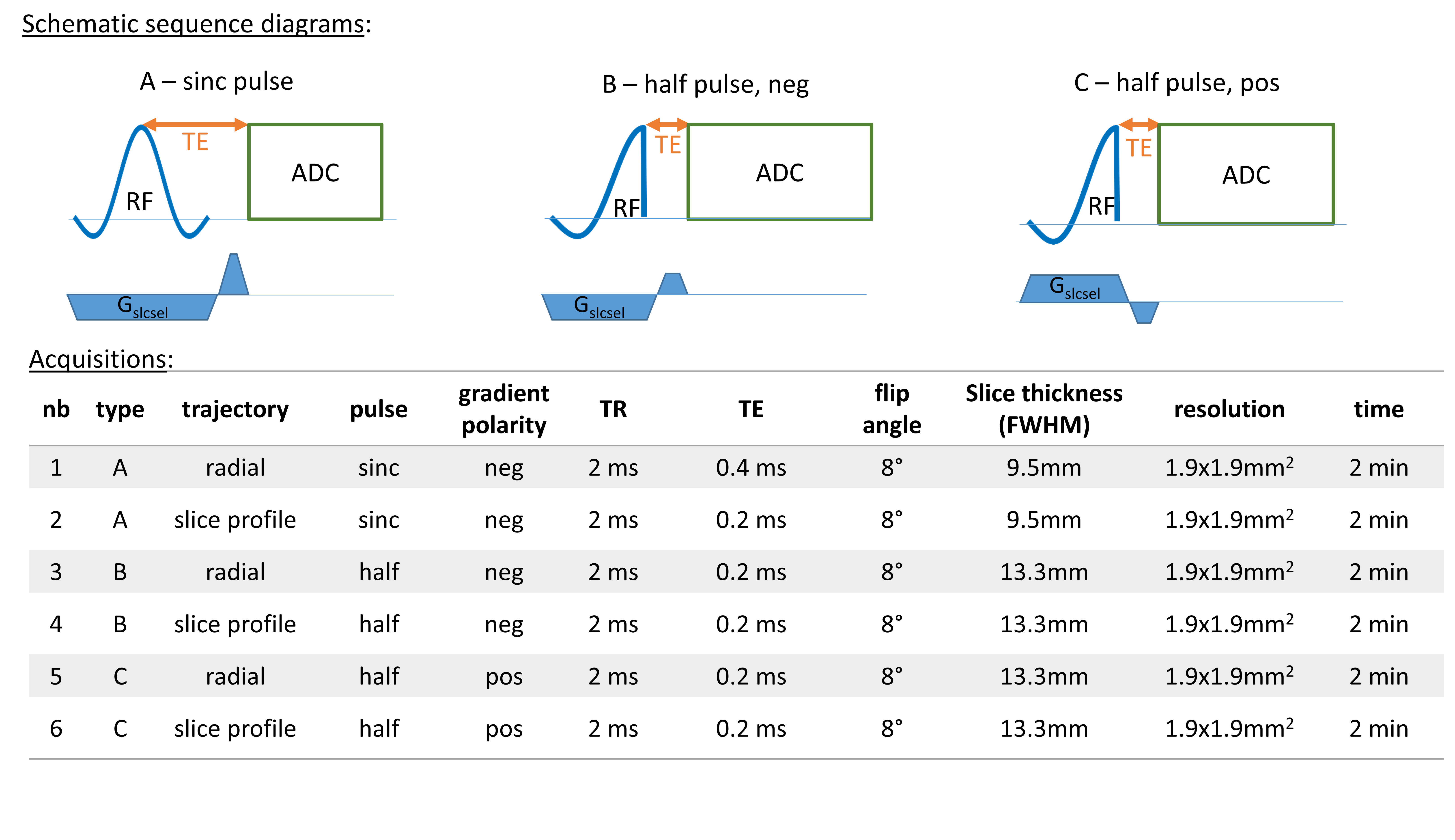
Figure 1: Schematic overview of main sequence features and measurement parameters for all acquisitions performed in this study. RF – excitation pulse, ADC – data acquisition, Gslcsel – Gradient for slice selection, TE – echo time, TR- repetition time, time – total measurement time
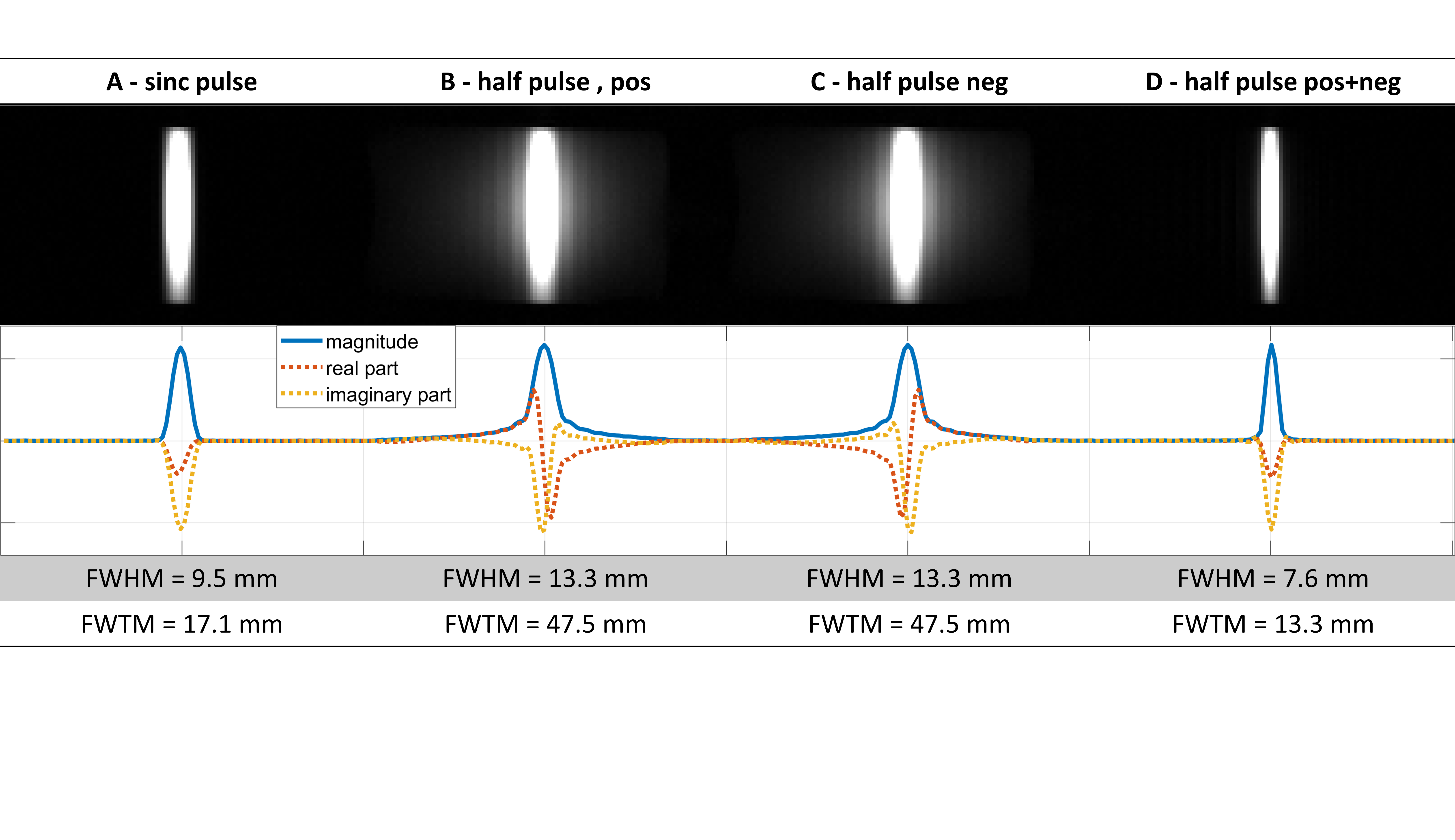
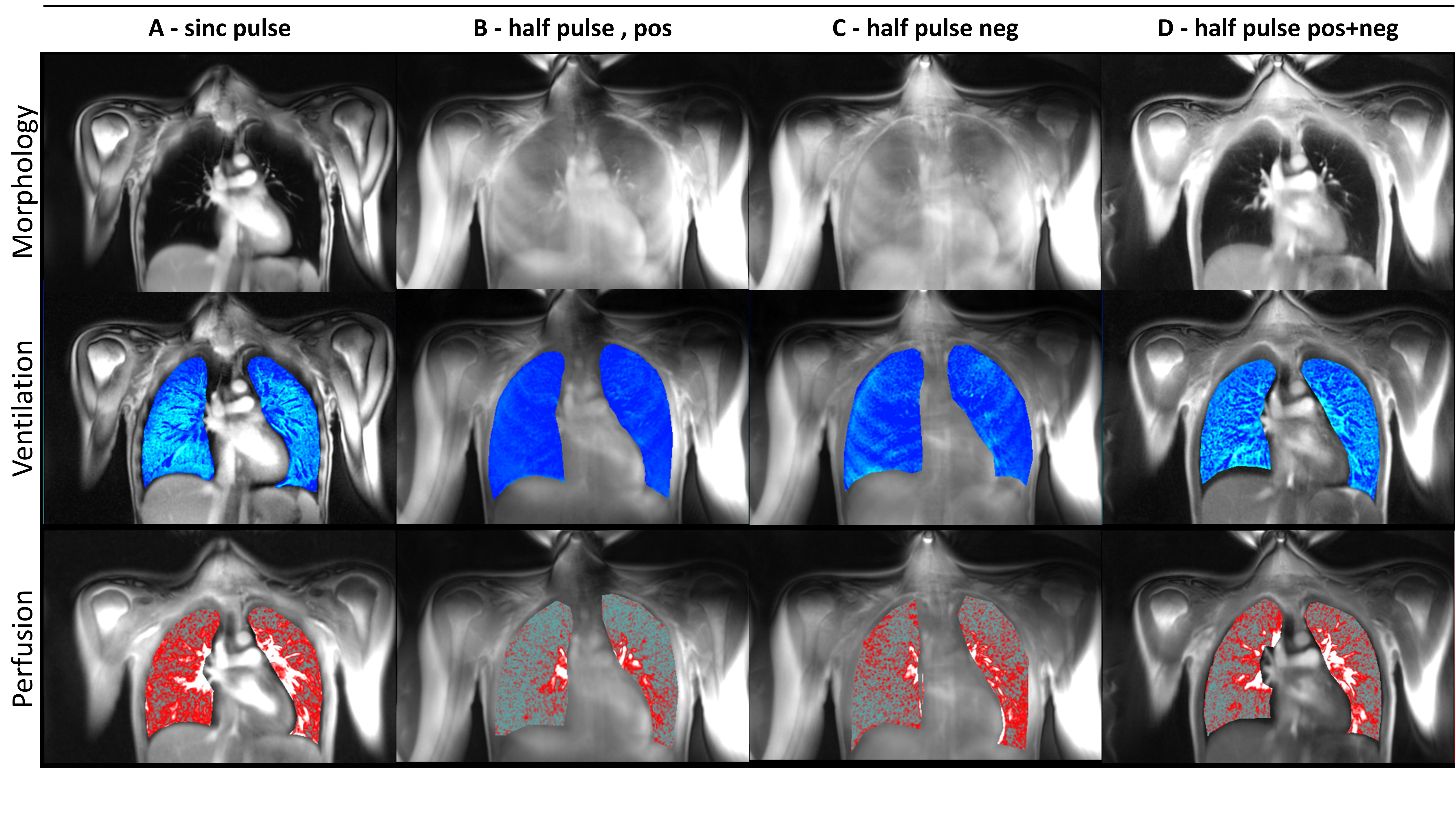
Figure 3: Morphological images (top row), ventilation maps (center row) and perfusion maps (bottom row) of a coronal slice in a healthy volunteer. Images were obtained from radial spoiled GRE acquisitions with A) sinc pulse, B) half pulse and positive slice selection gradient, C) half pulse and negative slice selection gradient and D) the complex sum combination of the two half pulse acquisitions B and C