4758
3D Diffusion-Prepared FLASH for Prostate MRI Near Metallic Implants1Radiology, Stanford University, Stanford, CA, United States, 2Bioengineering, Stanford University, Stanford University, CA, United States, 3Electrical Engineering, Stanford University, Stanford, CA, United States
Synopsis
Keywords: Prostate, New Signal Preparation Schemes
Motivation: Diffusion weighted imaging (DWI) is critical for prostate MRI, but echo planar imaging (EPI) DWI suffers from severe distortion in patients with hip implants or excessive bowel gas, often rendering images unusable.
Goal(s): To develop 3D DWI of the prostate with minimal distortion from nearby metal.
Approach: We compared a diffusion prepared, phase-navigated, fast low-angle shot (FLASH) readout sequence to EPI DWI to assess image quality, distortion correction and diffusion contrast.
Results: Phantom experiments demonstrate the reduced FOV, distortion correction and ADC accuracy. Images in human subjects avoid the severe signal loss and distortion of EPI DWI in the subject with metal.
Impact: We showed that 3D diffusion-prepared FLASH enables DWI where EPI often fails near hip replacements. Increased robustness of prostate imaging protocols to the presence of metal and/or bowel gas may obviate the need for contrast injection in these patients.
Introduction
Diffusion weighted (DW) imaging in the prostate is commonly used for tumor detection and assessment1. However, the commonly used multi-shot DW-EPI is limited by sensitivity to off-resonance. In patients with metallic hip replacements or severe bowel gas, EPI suffers from severe geometric distortion, dropouts, and pile-up2. Cartesian encoding with short readouts is an alternative robust to geometric distortion from off-resonance.We present a reduced FOV, diffusion-prepared, 3D Cartesian Fast Low Angle Shot (FLASH) sequence and reconstruction for distortionless imaging of the prostate. Phantom studies show a reduction in geometric distortion for the 3D DW-FLASH sequence compared to DW-EPI in the presence of metal. Patients with and without hip replacements were also scanned to demonstrate the effectiveness in vivo.
Methods
A phase-insensitive diffusion preparation was paired with 3D Cartesian FLASH to enable high RF bandwidth, distortionless diffusion-weighted imaging. The first 16 lines of the FLASH readout were used to sample central k-space for shot-to-shot phase correction (Rz = 2, Ry = 4). A reduced y FOV in the A/P direction was added to reduce the sampling requirement for phase navigation. Reduced FOV was achieved by reversing the amplitude of the slice-select gradient in the tipup pulse of the preparation (Figure 1). All acquisitions were performed at 3T on a Signa Premier (GE Healthcare, Milwaukee, WI). DW-FLASH was acquired with b-value 0, 800 s/mm2 (1/4 NEX). Other parameters: encoded FOV 24 cm, prepared PE FOV 12 cm, matrix size 128 × 128 × 24, slice thickness 3 mm, ETL 96, FA 4° during first 16, 12° for rest of echo train, TE prep 38 ms, TE FLASH 2.2 ms, TR FLASH 4.0 ms, RBW +/-20 kHz, scan time 5:45, anterior AIR coil (GE Healthcare) + posterior spine coil, preparation RF bandwidth 800 Hz.Sensitivity maps were obtained by applying ESPIRIT3 to the b = 0 s/mm2 data, and phase navigators were reconstructed with parallel imaging4. The full reconstruction used an L1-wavelet-regularized reconstruction.
To demonstrate the reduced FOV, phantom data was acquired using a diffusion phantom consisting of a center water bottle (to mimic the prostate), vials with different concentrations of acetone and water to achieve different ADCs5, and water and peanut oil placed on either side. To demonstrate the distortionless imaging near the implant, the same phantom setup was scanned with a hip replacement placed in lieu of the peanut oil. Vendor-provided 4-shot DW-EPI MUSE was acquired for comparison. The sequence was applied in vivo in three patients with and without hip replacements undergoing MRI of the prostate, following IRB approval and informed consent. The clinical protocol includes, 4-shot DW-EPI MUSE (voxel size 1.5 × 1.5 × 4.2 mm, b = 50, 800 s/mm2), and T2-weighted images.
Results
Phantom images demonstrating the preparation with and without the reduced FOV are shown in Figure 2. The excited FOV of the phantom is reduced with little residual signal outside the passband. Phantom images with the metal hip replacement placed adjacent are shown in Figure 3. DW-EPI exhibits warping in the tubes and signal loss due to low excitation bandwidth and T2* decay. DW-FLASH is robust to this off-resonance, with no apparent distortion in the phantom and less shading.Figure 4 shows images from a patient without implants, and a patient with a non-metallic hip replacement that exhibited little artifact in DW-EPI. DW-FLASH has different T2-weighting, but fat exhibits very low ADC in DW-FLASH, suggesting that the phase navigator strategy is effective.
Figure 5 shows images from a patient with a bilateral hip replacement. The prostate in DW-EPI exhibits shading and geometric distortion. The prostate is clearly depicted in the b = 0 s/mm2 FLASH, but some shading is present DW-FLASH image resulting in elevated ADCs, likely due to failures in phase navigation caused by poor patient cooperation.
Discussion
DW-FLASH obtains distortionless images in cases where DW-EPI suffers from severe geometric distortion and dropout. The high RF bandwidth of the 3D FLASH sequence excites more spins near the prostate, and reduces shading near the metallic implant. DW-FLASH did not employ fat suppression since inversion recovery is required to achieve robust fat suppression near the implant. Employing STIR would reduce SNR, and the SNR of the sequence is limited since the stimulated echo reduces the signal by 2×. Future work includes evaluation in more patients with metallic hip replacements to evaluate the diagnostic quality of the images in the cases where DW-EPI fails.Conclusion
Reduced FOV diffusion-prepared FLASH offers an approach to prostate DWI that is robust to off-resonance, reducing distortion and signal loss artifacts that affect EPI.Acknowledgements
Research support from GE Healthcare. Karolinska Neuro MR Physics Group for pulse sequence programming support.References
1. Maurer MH, Heverhagen JT. Diffusion weighted imaging of the prostate-principles, application, and advances. Transl Androl Urol. 2017 Jun;6(3):490-498. doi: 10.21037/tau.2017.05.06. PMID: 28725591; PMCID: PMC5503962.
2. Czarniecki M, Caglic I, Grist JT, et al. Role of PROPELLER-DWI of the prostate in reducing distortion and artefact from total hip replacement metalwork. European Journal of Radiology. 2018 102:213-219.
3. Uecker M, Lai P, Murphy MJ, Virtue P, Elad M, Pauly JM, Vasanawala SS, Lustig M. ESPIRiT--an eigenvalue approach to autocalibrating parallel MRI: where SENSE meets GRAPPA. Magn Reson Med. 2014 Mar;71(3):990-1001. doi: 10.1002/mrm.24751. PMID: 23649942; PMCID: PMC4142121.
4. Chen NK, Guidon A, Chang HC, Song AW. A robust multi-shot scan strategy for high-resolution diffusion weighted MRI enabled by multiplexed sensitivity-encoding (MUSE). Neuroimage. 2013 May 15;72:41-7. doi: 10.1016/j.neuroimage.2013.01.038. Epub 2013 Jan 28. PMID: 23370063; PMCID: PMC3602151.
5. Wang X, Reeder SB, Hernando D. An acetone-based phantom for quantitative diffusion MRI. J Magn Reson Imaging. 2017;46(6):1683-1692. doi:10.1002/jmri.25727
Figures
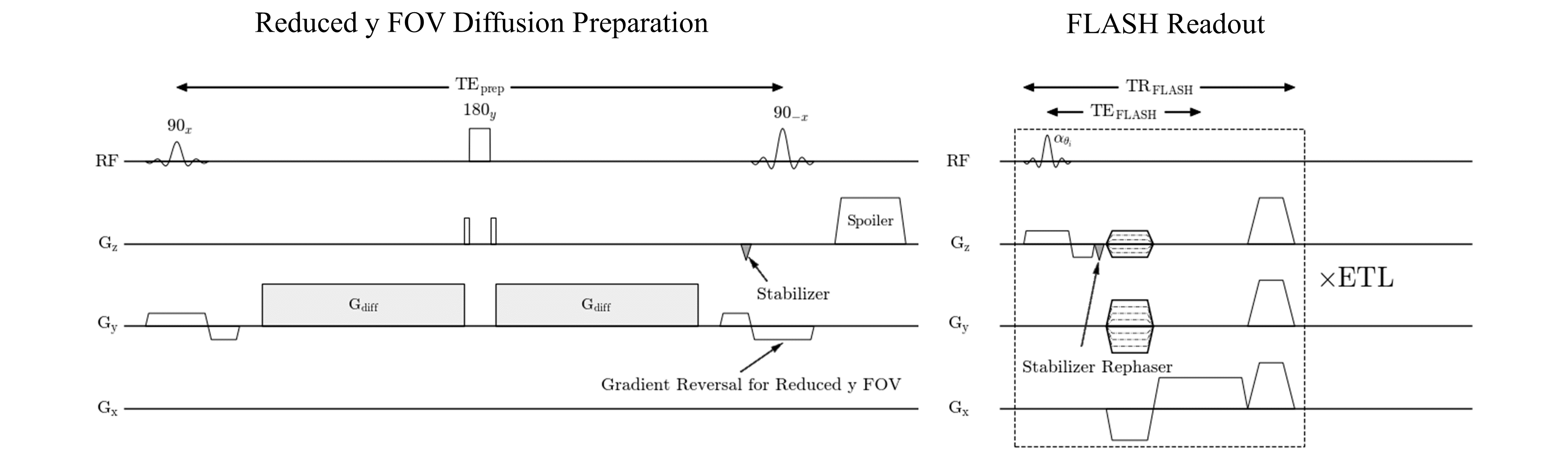
Figure 1: Sequence diagram including reduced y FOV diffusion preparation and FLASH readout.
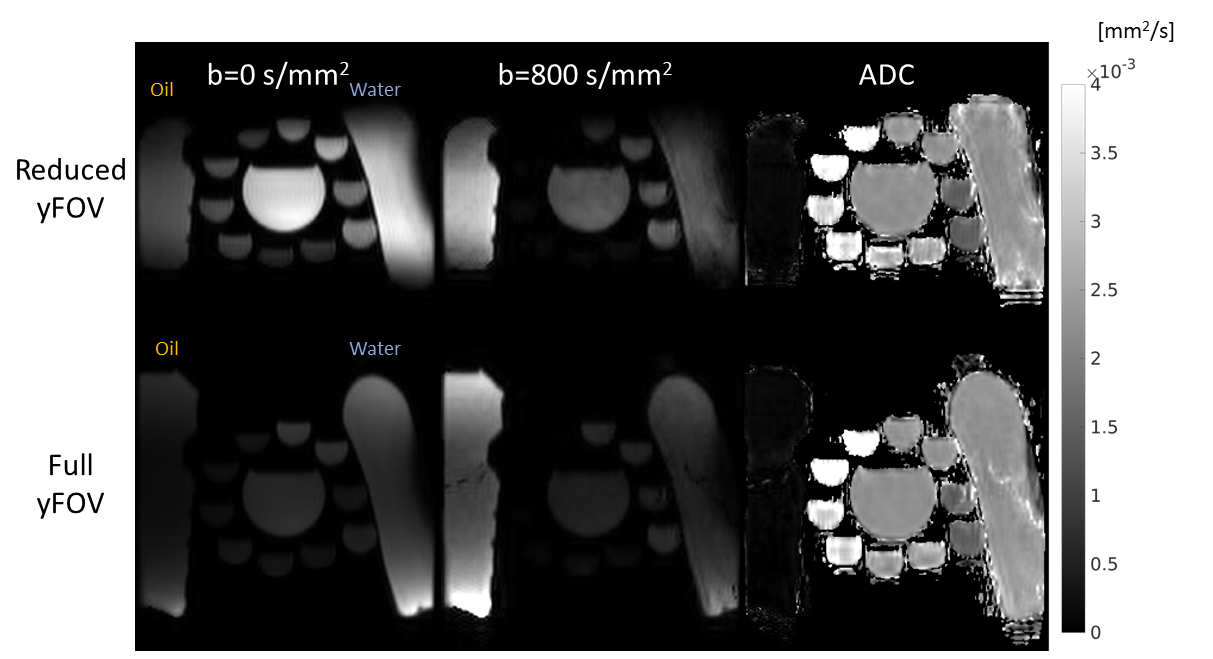
Figure 2: Effect of reduced yFOV on 3D FLASH images. Comparable ADCs are achieved with and without the reduced FOV. The preparation successfully suppresses signal outside the prescribed excitation volume.
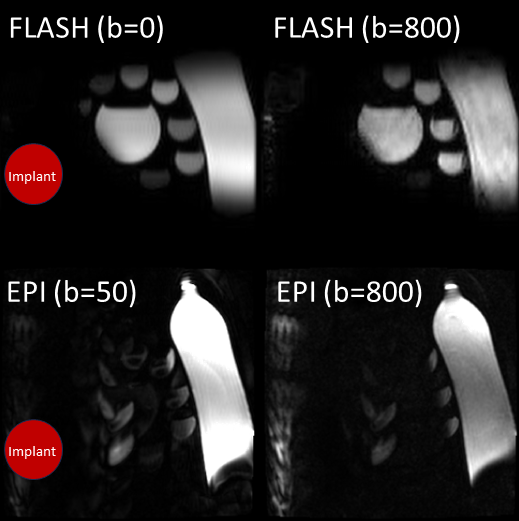
Figure 3: Effect of metal hip replacement on DW-FLASH and DW-EPI. Off-resonance distortion and low excitation bandwidth in DW-EPI eliminates signal in the diffusion phantom.
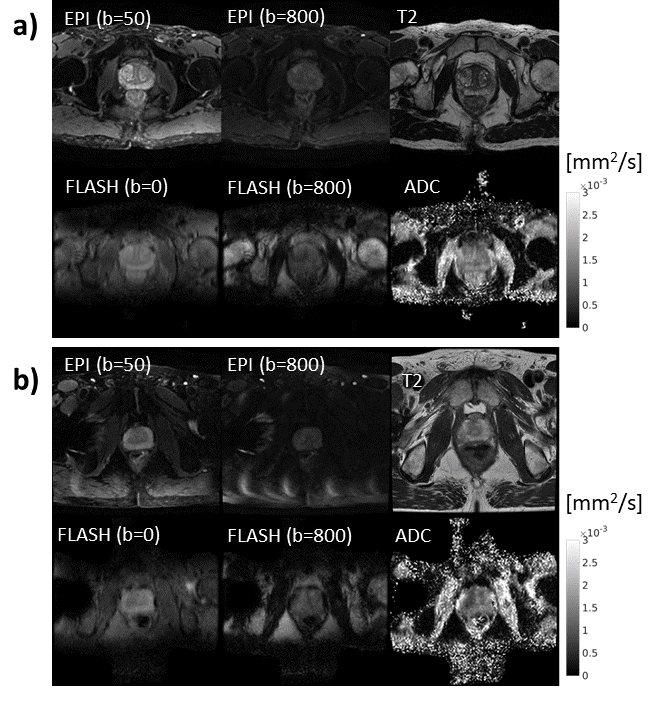
Figure 4: DW-FLASH compared to DW-EPI for a) a patient with no artifact, and b) a patient with a minimally disruptive hip replacement artifact. Axial T2 images are also shown for the given slice as an anatomic reference.
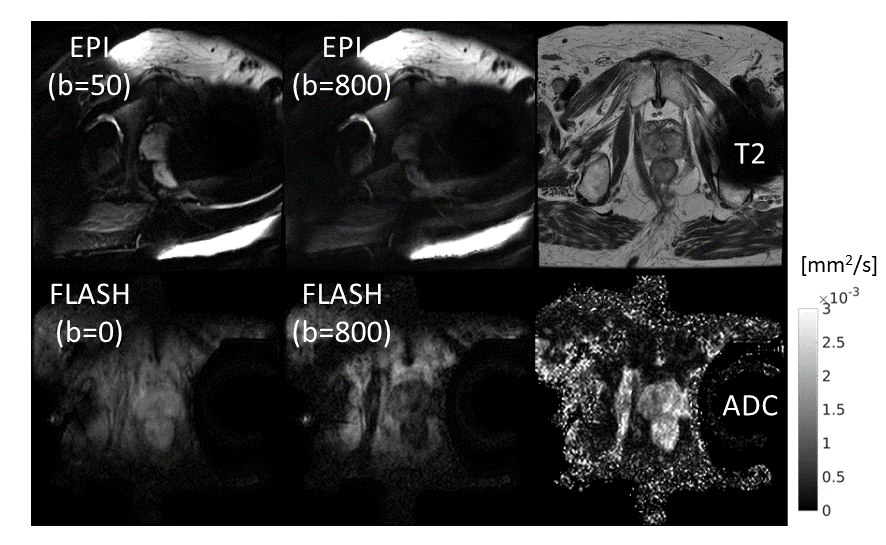
Figure 5: DW-FLASH compared to DW-EPI for a patient with a severely disruptive hip replacement artifact.