4754
Longitudinal 129Xe MRI Gas-exchange and Exercise Intolerance in Long-COVID1Department of Radiology, University of Iowa, Iowa City, IA, United States, 2Department of Iowa, University of Iowa, Iowa City, IA, United States, 3Institute for Clinical and Translational Sciences, University of Iowa, Iowa City, IA, United States, 4Roy J. Carver Department of Biomedical Engineering, University of Iowa, Iowa City, IA, United States, 5Department of Physics, University of Iowa, Iowa City, IA, United States, 6Department of Internal Medicine, University of Iowa, Iowa City, IA, United States
Synopsis
Keywords: Lung, COVID-19, Hyperpolarized Xenon MRI, Long COVID, Exercise tests
Motivation: Long-COVID symptoms are experienced by 10-20% of COVID-19 patients. 129Xe MRI ventilation and gas-exchange measurements may provide insights into long-COVID-19 patients' recovery.
Goal(s): Use 129Xe MRI to monitor longitudinal recovery (>1 year following infection) of long-COVID patients.
Approach: Thirteen long-COVID participants were evaluated longitudinally using pulmonary function tests, six-minute walk distance (6MWD), quality-of-life, and 129Xe MRI imaging measurements.
Results: Improvements in FEV1 and FVC%pred, dyspnea following exercise, and clinically significant improvements in 6MWD were observed. No significant differences in imaging measurements were observed between visits or between COVID and control groups. Dyspnea and MRI gas-exchange were correlated.
Impact: 129Xe MRI measurements in long-COVID participants suggest persistent gas-exchange abnormalities and exercise intolerance, offering valuable insights for future management and rehabilitation of these patients.
INTRODUCTION
Approximately 10-20% of patients infected with coronavirus disease 2019 (COVID-19) will experience symptoms more than 12 weeks following the acute infectious stage,1 better known as long-COVID. While the underlying processes responsible for long-COVID remain poorly understood, pulmonary injury and cardiovascular changes may contribute to the development and/or persistence of COVID-19 symptoms. Several investigations have used 129Xe MRI ventilation and gas-exchange measurements to evaluate post-COVID-19 patients. These sensitive measurements revealed abnormal ventilation defect percent (VDP)2,3 and gas-exchange3-6 within 3 months of infection, both of which improved, but did not normalize, following at least one year of recovery.7-9 Here, we aimed to use 129Xe MRI to provide insight into the longitudinal recovery (>1 year following infection) of long-COVID-19 patients.METHODS
We prospectively analyzed thirteen participants who were previously infected with COVID-19 and whose prior history or current symptoms caused by COVID-19 infection include at least one of the following: hospitalization due to infection, evidence of abnormal pulmonary function testing, or abnormalities on previous lung CT scan. Participants were evaluated 10-30 months (median=18 months) following COVID-19 infection (baseline/V1) and again 3-6 months (V2) (n=10) and 6-12 months (V3) (n=7) after baseline visit. Healthy controls (HC) (n=11) were analyzed for comparison. Anatomic 1H, 129Xe static ventilation, and gas-exchange MRI were acquired using a 3.0T Premier (GE Healthcare) scanner. Supine participants were coached to inhale a volume of gas equivalent to 20% of the participants’ predicted total lung capacity (ventilation scans: 300 mL 129Xe with remainder N2; gas-exchange: 100% 129Xe; anatomic scans: room air) from end-expiratory tidal breath, with image acquisition under breath-hold conditions. Quantitative MRI analysis was performed as previously described.10,11 Participants also performed spirometry, diffusing capacity of the lungs for carbon monoxide (DLCO), six-minute walk test for six-minute walk distance (6MWD) and St. George's Respiratory Questionnaire (SGRQ). Paired samples t-tests were performed to evaluate differences in COVID participants between timepoints. Univariate analysis of variance was used to compare imaging measurements between COVID and HC, corrected for age. Pearson/Spearman correlations were used to evaluate relationships.RESULTS
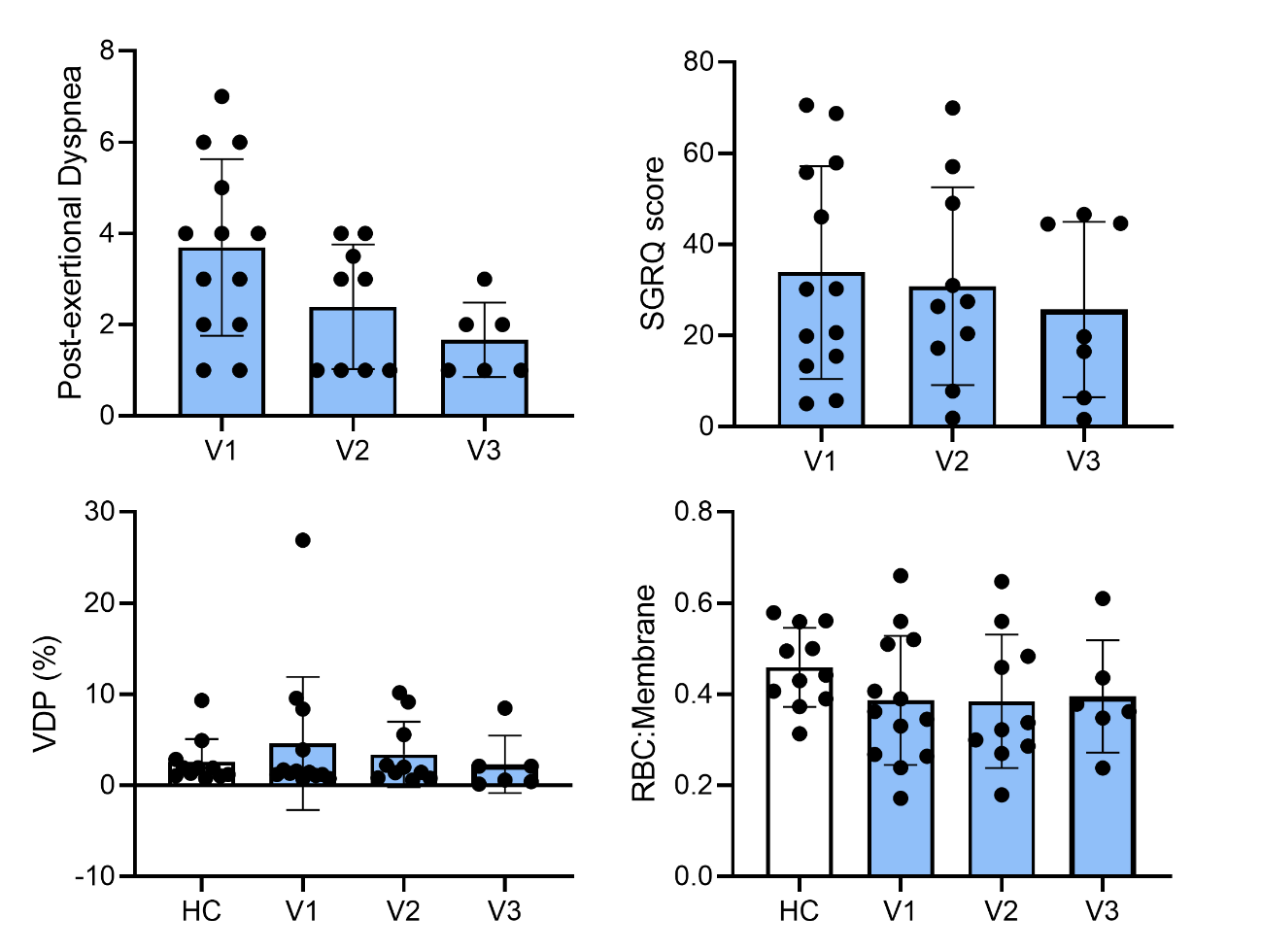
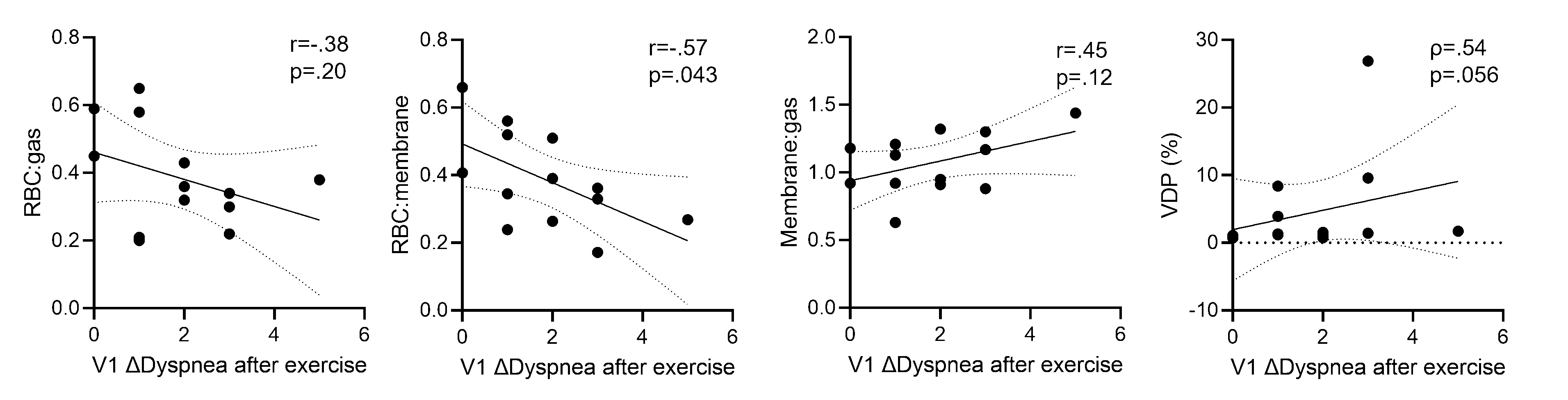
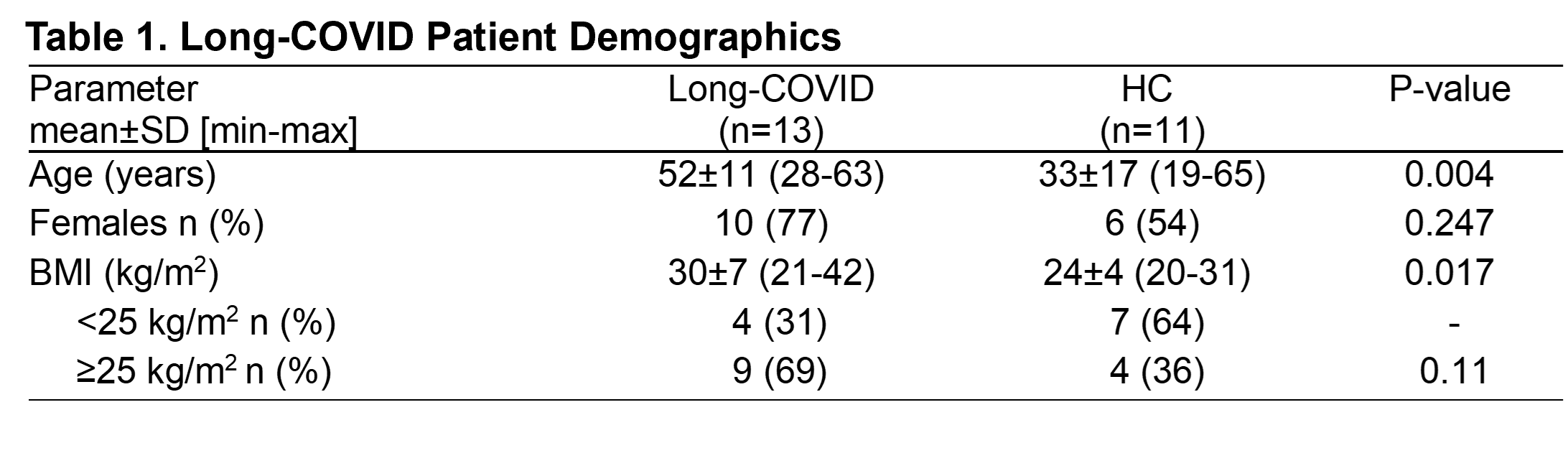
Participant demographics are provided in Table 1 (Figure 1). Thirteen COVID participants were evaluated at V1 (10 females; age=52±11 years, range=28-63 years). Pulmonary function, exercise capacity, quality-of-life and MRI imaging measurements at all time points are summarized in Table 2 (Figure 2) and Figure 3. Forced expiratory volume in the first second (FEV1) (p=.002) and FEV1%pred (p=.02) were improved between V2 and V3, and FVC%pred (p=.05) was improved between V1 and V3. Dyspnea following exercise was nominally improved at V2 and V3 as compared to V1, alongside clinically significant improvements12 in 6MWT distance in 4/9 participants at V2. There were no significant differences in imaging measurements across visits, or between COVID and HC groups. At V1, VDP was abnormal13 in 4/13 participants; clinically significant improvements in VDP (2%)13 were also observed in 2/3 participants at V2. Figure 4 shows correlations for V1 imaging measurements and exercise capacity. The change in dyspnea following exercise at V1 was correlated to RBC:membrane (ρ=-0.57, p=0.043) and VDP (ρ=0.54, p=0.059). Change in 6MWD between V1 and V2 trended towards correlation with RBC:gas (r=-0.65, p=0.057).DISCUSSION
This pilot study investigates the complex and multifaceted nature of long-COVID, specifically focusing on its impact on pulmonary function as well as quality-of-life. 129Xe MRI comparisons, at all time-points, between HC and COVID participants did not demonstrate a significant difference. Furthermore, MRI ventilation and gas-exchange were minimally changed over time across COVID patients, similar to previous findings.7-9 However, nominal improvements were observed in VDP, SGRQ and 6MWD in some patients, showing that optimization in imaging may reflect the amelioration of clinical presentation. While the change in pulmonary function was statistically significant over time, these measures were normal at baseline and mildly changed. Our correlation analysis suggests that imaging measurements of ventilation and gas-exchange detect subclinical disease associated with post-exertional dyspnea. These findings may point towards a subset of long-COVID participants who could potentially benefit from pulmonary rehabilitation.14 Further analysis in a larger and more clinically diverse cohort may help understand the nature of lung injury remodeling of these patients.CONCLUSION
In a pilot cohort of long-COVID participants, 129Xe MRI measurements of ventilation and gas-exchange pointed towards a potential COVID phenotype with persistent gas-exchange abnormalities and exercise intolerance, providing encouraging insights for the management and rehabilitation of long-COVID patients.Acknowledgements
No acknowledgement found.References
1. WHO. Coronavirus Disease (COVID-19): Post COVID-19 condition. (2023).
2. Kooner, H.K., et al. (129)Xe MRI ventilation defects in ever-hospitalised and never-hospitalised people with post-acute COVID-19 syndrome. BMJ Open Respir Res 9(2022).
3. Li, H., et al. Damaged lung gas exchange function of discharged COVID-19 patients detected by hyperpolarized (129)Xe MRI. Sci Adv 7(2021).
4. Matheson, A.M., et al. Persistent (129)Xe MRI Pulmonary and CT Vascular Abnormalities in Symptomatic Individuals with Post-acute COVID-19 Syndrome. Radiology 305, 466-476 (2022).
5. Grist, J.T., et al. Lung Abnormalities Detected with Hyperpolarized (129)Xe MRI in Patients with Long COVID. Radiology 305, 709-717 (2022).
6. Grist, J.T., et al. Hyperpolarized (129)Xe MRI Abnormalities in Dyspneic Patients 3 Months after COVID-19 Pneumonia: Preliminary Results. Radiology 301, E353-E360 (2021).
7. Saunders, L.C., et al. Longitudinal Lung Function Assessment of Patients Hospitalized With COVID-19 Using (1)H and (129)Xe Lung MRI. Chest 164, 700-716 (2023).
8. Matheson, A.M., et al. Longitudinal follow-up of postacute COVID-19 syndrome: DL(CO), quality-of-life and MRI pulmonary gas-exchange abnormalities. Thorax 78, 418-421 (2023).
9. Kooner, H.K., et al. Postacute COVID-19 Syndrome: (129)Xe MRI Ventilation Defects and Respiratory Outcomes 1 Year Later. Radiology 307, e222557 (2023).
10. Zha, W., et al. Semiautomated Ventilation Defect Quantification in Exercise-induced Bronchoconstriction Using Hyperpolarized Helium-3 Magnetic Resonance Imaging: A Repeatability Study. Acad Radiol 23, 1104-1114 (2016).
11. Kaushik, S.S., et al. Single-breath clinical imaging of hyperpolarized (129)Xe in the airspaces, barrier, and red blood cells using an interleaved 3D radial 1-point Dixon acquisition. Magn Reson Med 75, 1434-1443 (2016).
12. Polkey, M.I., et al. Six-minute-walk test in chronic obstructive pulmonary disease: minimal clinically important difference for death or hospitalization. Am J Respir Crit Care Med 187, 382-386 (2013). 13. McIntosh, M.J., et al. 129Xe MRI Ventilation Defects in Asthma: What is the Upper Limit of Normal and Minimal Clinically Important Difference? Academic Radiology (2023).
14. Paz, L.E.S., Bezerra, B., Pereira, T.M.M. & da Silva, W.E. COVID-19: the importance of physical therapy in the recovery of workers' health. Rev Bras Med Trab 19, 94-106 (2021).
Figures
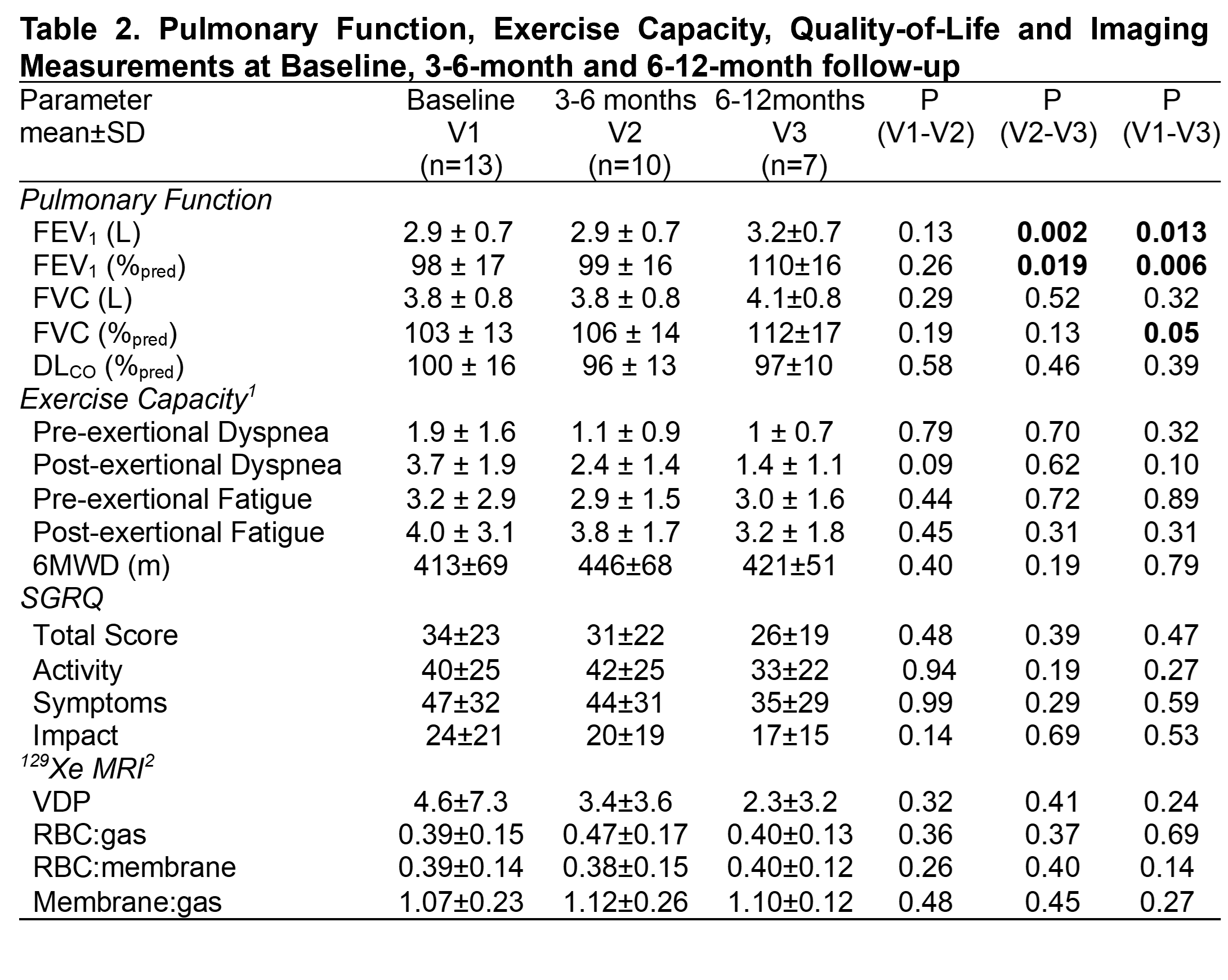
Abbreviations: FEV1=forced expiratory volume in first second; %pred=percent of predicted value; FVC=forced vital capacity; DLCO=diffusing capacity of the lung for carbon monoxide; 6MWD=six- minute walk distance; SGRQ=St. George’s Respiratory Questionnaire; MRI=magnetic resonance imaging; VDP=ventilation defect percent; RBC=red blood cell P=p value for paired samples t-test between time points
1: at V2 n=9, at V3 n=6; 2: at V3 n=6