4753
Low field (60mT) MRI using flexible coil for prostate imaging1Promaxo, Inc., Oakland, CA, United States
Synopsis
Keywords: Prostate, Prostate
Motivation: The low field (60mT) MRI system offers advantages such as affordability and portability.
Goal(s): To develop flexible coils for low field (60mT) MRI to improve image quality.
Approach: Designing a multi-channel receive coil using flexible body coil technology, allowing improved workflow, close proximity to the patient's body and improved SNR.
Results: The flexible coil demonstrated higher SNR in phantom experiment, enhancing image quality and enabling visualization of previously undetected areas in in-vivo experiment.
Impact: The advancements in flexible coils have the potential to improve image guided procedures, facilitating accurate targeted biopsies and ultimately improving patient outcomes.
Introduction/Background
The low field MRI system has advantages including low cost, portable, and shielding free environment (1). The recently developed single-sided low-field (60 mT) MRI system (Promaxo Inc., Oakland, California, United States) has shown higher cancer detection rates over the standard of care by providing MR image guidance to transperineal biopsy procedures (2). The early product consisted of a rigid receive coil, designed based on the average body size and shape, which may not accommodate the varying size of individual patients. This limitation can result in reduced image quality and awkward patient positioning depending on the patient size. Flexible coils are designed to conform closely to the patient's body, reducing the gap between the coil and the area being imaged (3). This close proximity improves the signal-to-noise ratio and enhances image quality, allowing for better visualization. In this abstract, we have shown the recent developments of flexible coils for low field (60mT) MRI, which offers improved image quality. These advancements in flexible coils have the potential to provide accurate targeted biopsy for prostate cancer, improving patient outcomes.Methods/Materials
Coil Configuration: Rigid body coil and Flexible body CoilMulti-channel receive coil was designed for prostate imaging (Fig. 1b). The rigid body coil and the flexible body coil were made by the same RG-223/U coaxial cable with diameter of 5.38mm and impedance of 50 ohm (3). The rigid body coil was fixed to the in housing plastic structure and the flexible body coil was fixed to foam.
Acquisition and Reconstruction
The 7 min T2-weighted pulse sequence uses broadband, chirped RF pulses in a CHORUS type sequence to minimize the effects of B1 inhomogeneity. RARE phase encoding with a center out spiral trajectory was used. In this trajectory, each echo in the echo train phase encodes a different kx-ky point while kz is frequency encoded with the permanent z gradient used as the readout gradient (4). The sequence has echo train length varying from 8 to 12 echoes, a TR = 1.45 sec, and with an echo spacing varying from 5.4 to 3.2 millisecs. Images were reconstructed with 1.5 mm x 1.5 mm in plane resolution, an effective field of view of 180 mm x 180 mm, and a slice thickness of 2.75 mm. The reconstruction was performed using an iterative, conjugate gradient least square (CGLS) method with Tikhonov regularization.
Phantom Experiments
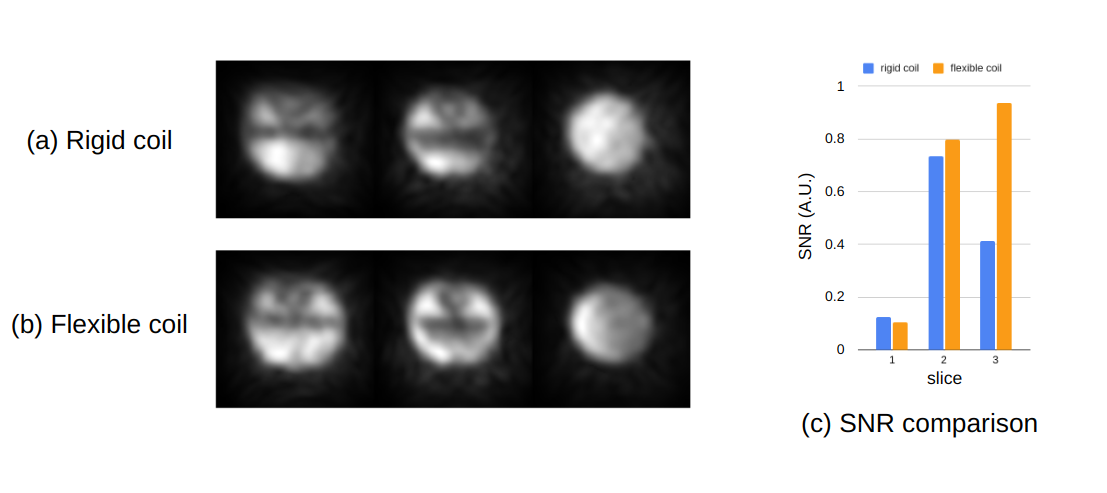
The American College of Radiology (ACR) MRI phantom is a 203.2 mm diameter cylinder, and 173.40 mm tall with various fixtures inside. The in housing plastic structure was used to fix the flexible body coil at the same position according to ACR phantom. The snr was calculated by the ratio between the average value of homogenous pixels in the ACR phantom and the standard deviation of background.
In-vivo experiments
A healthy volunteer 77 years old male without any disease was scanned. Consent to use the data and images were obtained under IRB protocol.
Results
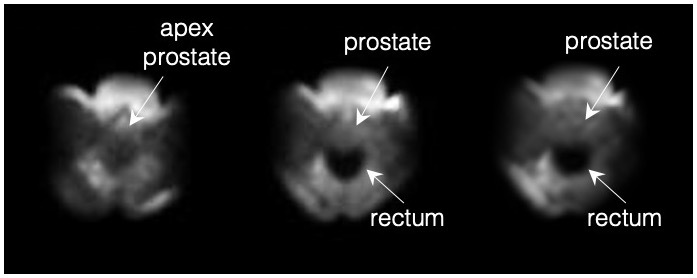
The phantom experiment shows that the flexible coil can acquire higher snr as the slice becomes farther from the magnet (Fig. 2c). The In-vivo experiment shows that the flexible coil can acquire the signal from anatomy deeper into the body/prostate (Fig. 3)Conclusion
We have demonstrated that the flexible nature of the self-shielded coil design allows for similar if not improved image quality over the rigid coil design. The flexible nature assists in the image guided procedures and will improve the entire patient workflow of the system.Acknowledgements
n/aReferences
1. Liu, Y., Leong, A.T.L., Zhao, Y. et al. A low-cost and shielding-free ultra-low-field brain MRI scanner. Nat Commun 12, 7238 (2021). https://doi.org/10.1038/s41467-021-27317-1
2. Satya, P., Adams, J., Jr, Venkataraman, S. S., Kumar, D., Narayanan, R., Nacev, A., & Macaluso, J. N., Jr (2022). Office-Based, Single-Sided, Low-Field MRI-Guided Prostate Biopsy. Cureus, 14(5), e25021. https://doi.org/10.7759/cureus.25021
3. Wang, B., Siddiq, S.S., Walczyk, J. et al. A flexible MRI coil based on a cable conductor and applied to knee imaging. Sci Rep 12, 15010 (2022). https://doi.org/10.1038/s41598-022-19282-6
4. Perlo J, Casanova F, Blümich B. 3D imaging with a single-sided sensor: an open tomograph. J Magn Reson. 2004 Feb;166(2):228-35. doi: 10.1016/j.jmr.2003.10.018. PMID: 14729034.
Figures