4747
Evaluating the diagnostic performance of Dixon and MRS based proton density fat fraction (PDFF) in hepatic steatosis1Institute of Science and Technology for Brain-Inspired Intelligence, Fudan University, Shanghai, China, 2Department of Endocrinology and Metabolism, Zhongshan Hospital, Fudan University, Shanghai, China, 3Oden Institute for Computational Engineering and Sciences, University of Texas at Austin, Austin, TX, United States, 4Philips Healthcare, Shanghai, China, 5Department of Endocrinology and Metabolism, Zhongshan Hospital, Fudan Institute for Metabolic Disease, Human Phenome Institute, Fudan University, Shanghai, China
Synopsis
Keywords: Liver, Liver
Motivation: Steatosis is the histopathologic hallmark of NAFLD. Liver histology is currently the standard for hepatic steatosis diagnosis, which is invasive. Several MRI methods have been validated to accurately measure hepatic fat content.
Goal(s): To evaluate diagnostic performance of different hepatic fat quantification methods.
Approach: We compared hepatic fat content calculated by Dixon MRI and MRS with histology results as reference.
Results: The outcomes show that the fat fraction measured by these two methods highly correlated with steatosis degrades measured by histology. Compared with MRS, fat fraction calculated by Dixon MRI performed better diagnostic capacity in hepatic steatosis.
Impact: Our study demonstrates that the Dixon-based method outperforms the MRS. The use of whole liver automatic segmentation improves diagnostic efficiency, and its performance is comparable to the ROI-based method, making it a promising hepatic fat fraction detection approach in clinic.
Introduction
Hepatic fat content is a significant indicator for diagnosing nonalcoholic fatty liver disease (NAFLD). Current standard for fat fraction quantification is hepatic biopsy, which is invasive [1]. Both Magnetic Resonance Spectroscopy (MRS) and Dixon-based Magnetic Resonance Imaging (MRI) have demonstrated their ability to precisely measure hepatic fat fraction [2]. Dixon-based methods offer the advantage of providing full liver coverage during acquisition, making execution and analysis easier [3]. Our aim is to evaluate the diagnostic performance of hepatic steatosis using different MRI methods (Dixon MRI and MRS), with liver biopsy as the reference standard. In Dixon-based MRI, we used both manually labeled ROI and fully automatic whole liver segmentation (WLS) to measure hepatic proton density fat fraction (PDFF). The diagnostic performance of the automatic method was also investigated compared to manual ROI and MRS.Materials and Methods
The workflow of the methods is demonstrated in Figure 1.Data Acquisition
The study had the a priori approval from the institutional review boards of the Zhongshan Hospital Fudan University. We recruited 61 patients with clinically confirmed or suspected NAFLD. All participants received liver biopsy and underwent MR scans on a 3T Philips Ingenia CX scanner (Philips, Best, The Netherlands). The imaging protocol included a pointed-resolved MRS sequence (single-voxel size = 2×2×2cm3 , TR/TE = 2000/50ms, Flip angle = 90°, scan duration = 16s ), and an axial three-dimensional multi-echo modified Dixon gradient echo sequence (resolution = 2.27×2.27×3mm3, echo train = 6, flip angle = 3°, number of slices = 80).
Imaging Processing
The data of MRS were interpreted using Philips software by an experienced reader who was blinded to MRI and histologic results. MRS PDFF was calculated as the area of peak fat divided by the sum of the peak water and fat areas, then multiplied by 100. Dixon-based PDFF was obtained using two methods. The first one used manual ROIs. Five ROIs were manually labeled using the Philips Interspace Portal, avoiding large vessels, ducts, and hepatic lesions. One representative region was selected for evaluating the whole liver fat fraction. The second method used automated whole liver segmentation (WLS). We employed 3d_fullres nnUnet [4] with the TrainerV2_DA3 strategy to train 435 Dixon images acquired from Shanghai Panorama Medical Imaging Center, Zhongshan Hospital and Ruijin Hospital for liver segmentation. The segmented whole liver regions were used to calculate averaged liver fat fraction.
Statistical Analysis
Data analysis was carried out using R software version 4.3.2. Correlations between PDFF measured by three methods and histologic steatosis grades were assessed by using Spearman correlation coefficient. Receiver operating characteristic (ROC) analysis was performed to evaluate the diagnostic performance of the three methods. Cutoff values with specificity greater than 90% were selected to rule-in different grades of hepatic steatosis. The DeLong test was used to compare the area under the receiver operating characteristic curves (AUCs) of ROI, WLS and MRS.
Results
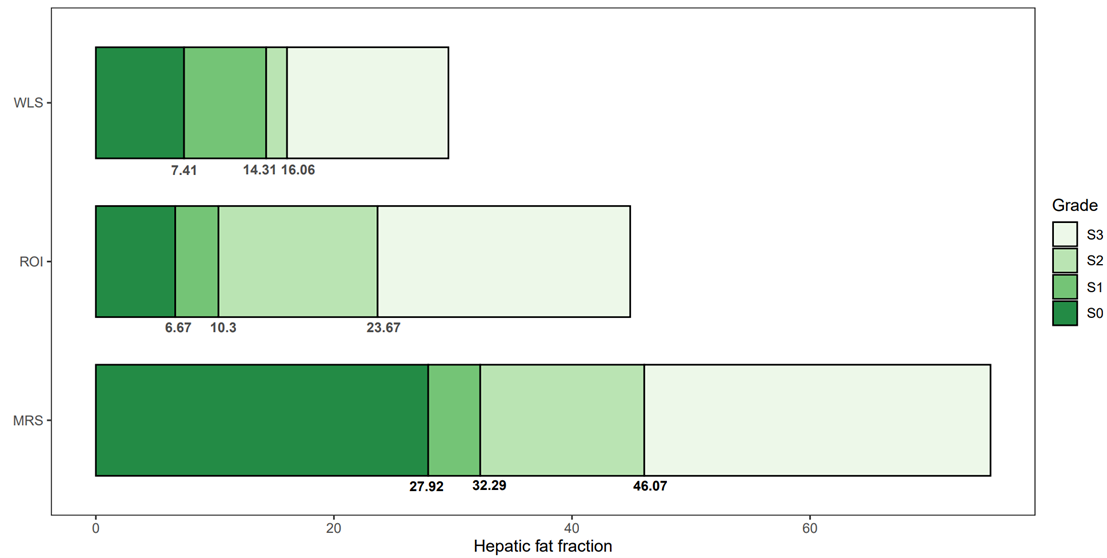
A total of 61 participants were included (39 male, 41.59 ± 13.78 years) (Figure 2). PDFF measured by all the three methods demonstrated a strong correlation with histology steatosis degrades (rs = 0.79 p<0.001, rs = 0.73 p<0.001, and rs = 0.64 p<0.001, respectively) (Figure 3). Results of Dixon-based two methods showed similar diagnostic performance for steatosis grading (ROI AUC, 0.922; WLS AUC, 0.899), and both were more accurate than MRS (MRS AUC, 0.827) (Figure 4). The ROI cutoff values for ruling-in S1, S2 and S3 were 6.67, 10.3 and 23.67 (%), respectively, and the cutoff values for another two methods are demonstrated in Figure 5.Discussion
The cutoff values for different steatosis grades, which exhibited high specificity, were similar to previous studies [5][6][7]. The MRS had a high threshold for the diagnosis of hepatic steatosis compared to previous study [8], in part owing to the sampling error (i.e., quality of voxel placement) and the inclusion of patients known or suspected NAFLD, rather than healthy volunteers. The cutoff values calculated by MRS at S2-3 and S3 are consistent with previous studies [9]. The cutoff values for different hepatic steatosis grades provided in our study offers insights for clinical application of Dixon based PDFF.Conclusion
Dixon-based method outperforms MRS in diagnostic performance for hepatic steatosis, while the performance of WLS PDFF is similar to that of manual ROI PDFF. The WLS approach is promising to improve the efficiency of clinical diagnosis while maintaining a high accuracy of hepatic fat fraction.Acknowledgements
No acknowledgement found.References
[1] Martí-Aguado D, Jiménez-Pastor A, Alberich-Bayarri Á, et al. Automated whole-liver MRI segmentation to assess steatosis and iron quantification in chronic liver disease[J]. Radiology, 2022, 302(2): 345-354.
[2] Kang B K, Kim M, Song S Y, et al. Feasibility of modified Dixon MRI techniques for hepatic fat quantification in hepatic disorders: validation with MRS and histology[J]. The British journal of radiology, 2017, 91(1089): 20170378.
[3] Brancato V, Della Pepa G, Bozzetto L, et al. Evaluation of a Whole-Liver Dixon-Based MRI Approach for Quantification of Liver Fat in Patients with Type 2 Diabetes Treated with Two Isocaloric Different Diets[J]. Diagnostics, 2022, 12(2): 514.
[4] Isensee F, Jaeger P F, Kohl S A A, et al. nnU-Net: a self-configuring method for deep learning-based biomedical image segmentation[J]. Nature methods, 2021, 18(2): 203-211.
[5] Tang A, Desai A, Hamilton G, et al. Accuracy of MR imaging-estimated proton density fat fraction for classification of dichotomized histologic steatosis grades in nonalcoholic fatty liver disease. Radiology. 2015;274(2):416-425.
[6] Middleton MS, Van Natta ML, Heba ER, et al. Diagnostic accuracy of magnetic resonance imaging hepatic proton density fat fraction in pediatric nonalcoholic fatty liver disease. Hepatology. 2018;67(3):858-872.
[7] Middleton MS, Heba ER, Hooker CA, et al. Agreement Between Magnetic Resonance Imaging Proton Density Fat Fraction Measurements and Pathologist-Assigned Steatosis Grades of Liver Biopsies From Adults With Nonalcoholic Steatohepatitis. Gastroenterology. 2017;153(3):753-761.
[8] Szczepaniak LS, Nurenberg P, Leonard D, et al. Magnetic resonance spectroscopy to measure hepatic triglyceride content: prevalence of hepatic steatosis in the general population. Am J Physiol Endocrinol Metab. 2005;288(2):E462-E468.
[9] Georgoff P, Thomasson D, Louie A, Fleischman E, Dutcher L, Mani H, Kottilil S, Morse C, Dodd L, Kleiner D, Hadigan C. Hydrogen-1 MR spectroscopy for measurement and diagnosis of hepatic steatosis. AJR Am J Roentgenol. 2012 Jul;199(1):2-7.
Figures
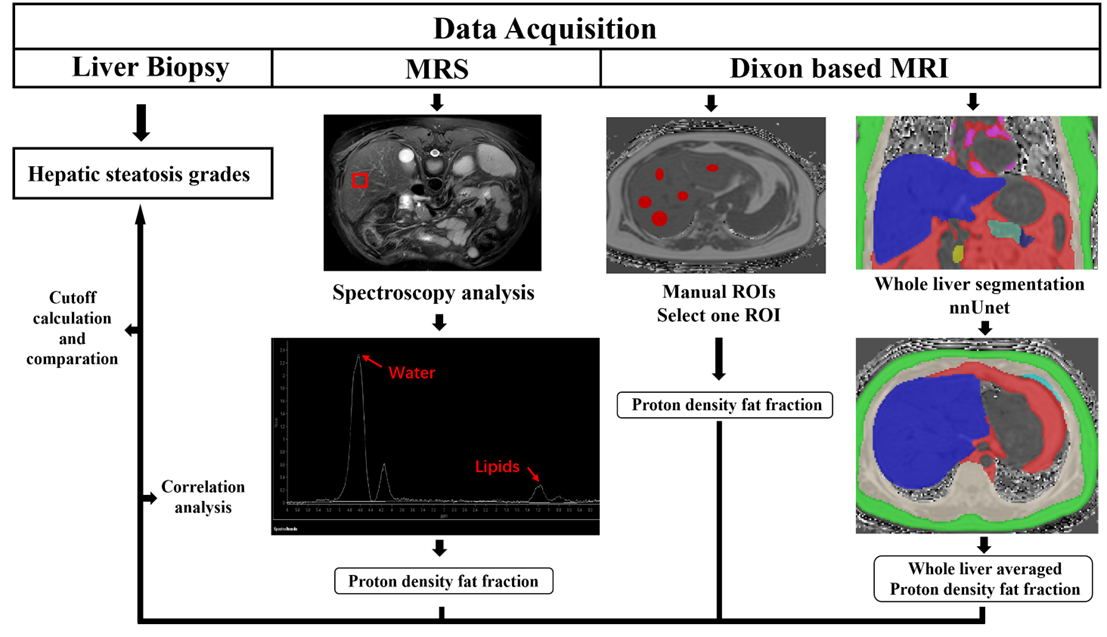
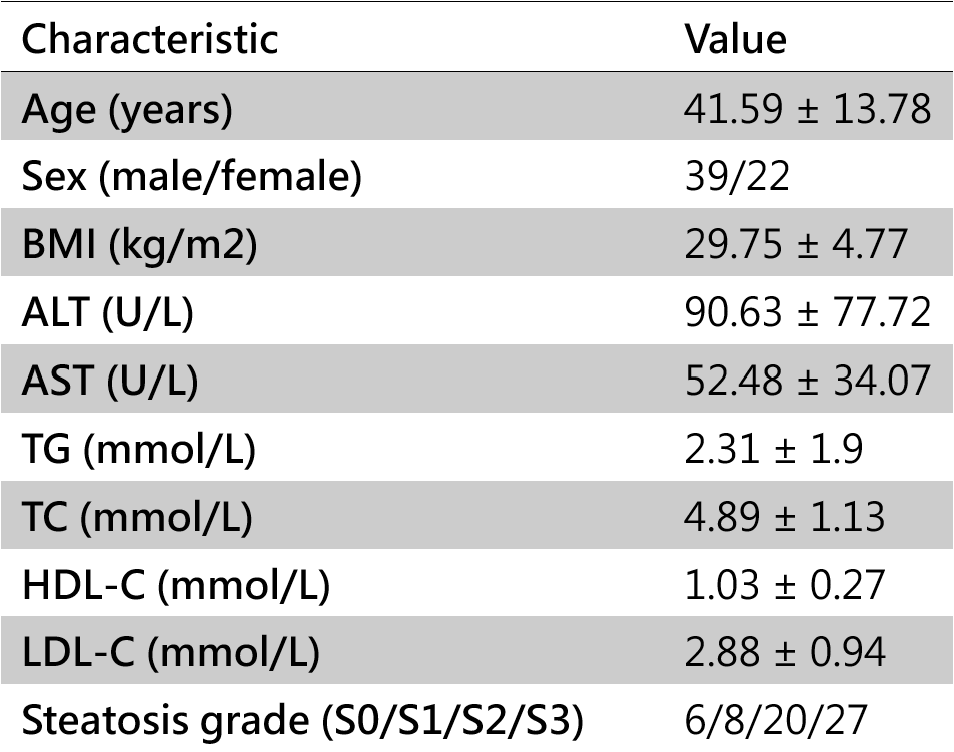
Figure 2: Baseline Characteristics.
Note.— Data are presented as mean ± standard deviation or n. BMI = body mass index, ALT = alanine aminotransferase, AST = aspartate aminotransferase, TG = triglyceride, TC = total cholesterol, LDL-C = low density lipoprotein cholesterol, HDL-C = high density lipoprotein cholesterol.
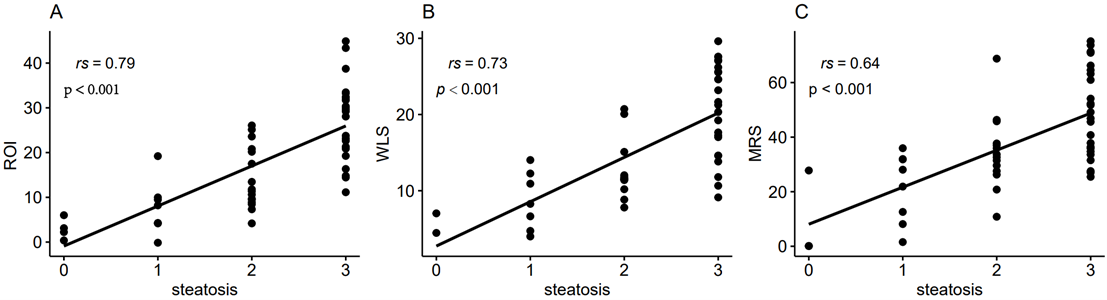
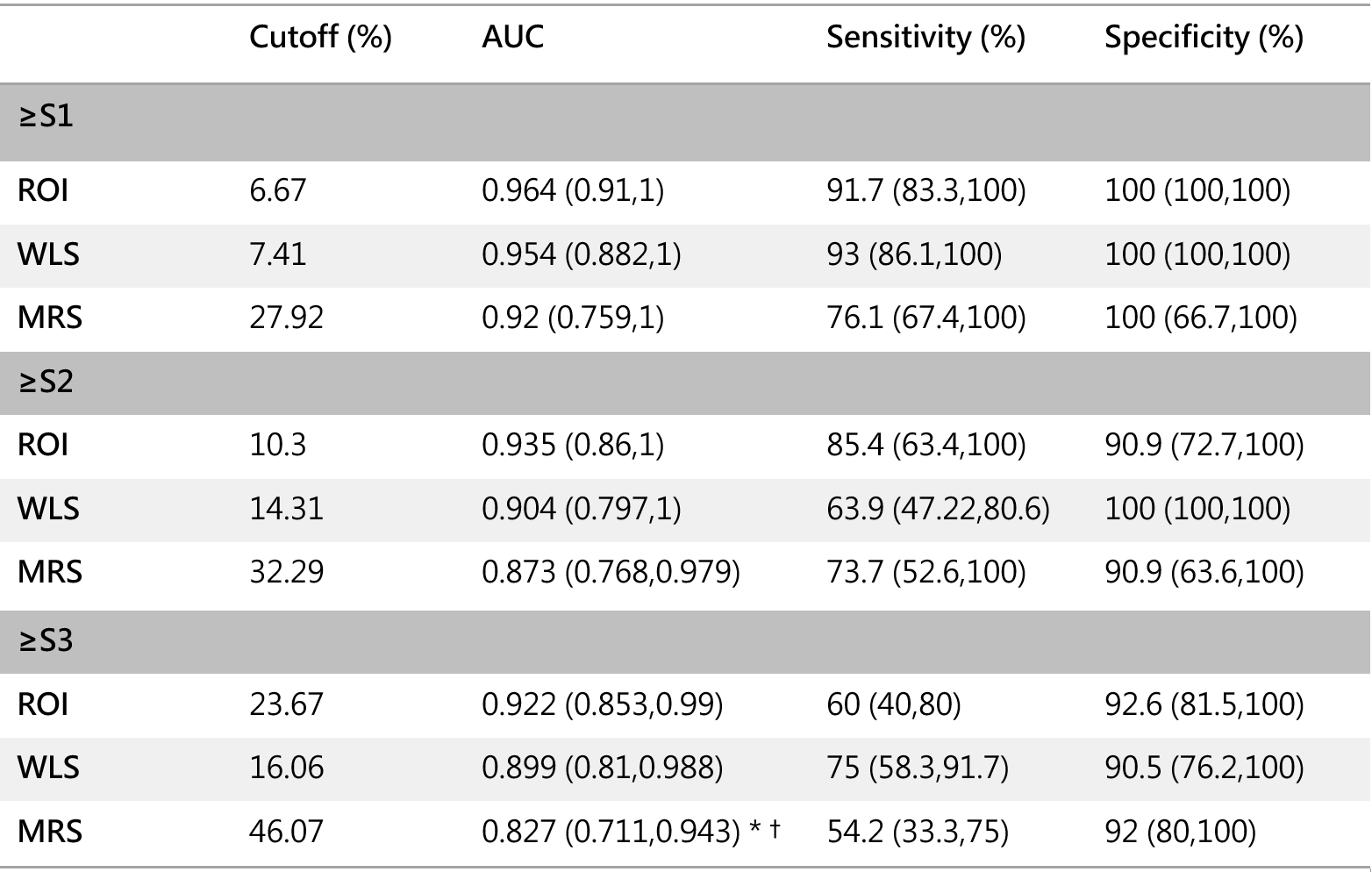
Figure 4: Diagnostic Performance of ROI, WLS and MRS Thresholds for Steatosis.
Note.—Numbers in brackets are 95% CIs. ROI = region of interest, WLS = whole-liver segmentation, MRS = magnetic resonance spectroscopy
*P value < 0.05 compared with ROI.
†P value < 0.05 compared with WLS.