4739
Assessment of Lipid Levels in Newly Diagnosed Diabetic Obese Patients Treated with GLP-1 Inhibitors Using MRI-PDFF1Radiology, Zhongda Hospital, Medical School, Southeast University, Nanjing, China, 2Endocrinology, Zhongda Hospital, Medical School, Southeast University, Nanjing, China
Synopsis
Keywords: Endocrine, Diabetes
Motivation: GLP-1 receptor agonists have shown favorable effects in improving obesity and ectopic fat deposition in type 2 diabetes patients. MRI-PDFF can serve as a tool for continuous, dynamic assessment of lipid content changes in patients.
Goal(s): Dynamic monitoring of fat content and lipid deposition changes in type 2 diabetes obese patients receiving glucagon-like peptide-1 receptor agonist treatment using MRI-PDFF.
Approach: 21 male diabetic patients received 3-month treatment: semaglutide (n=12) or loxenatide (n=9). Clinical data collected, pre/post 3.0T MRI scans (T1WI, T2WI, MRI-PDFF) measured fat.
Results: The semaglutide group showed significant fat reduction in multiple organs, while the loxenatide group reduced pancreatic fat fraction.
Impact: Semaglutide effectively controls blood glucose and body weight in type 2 diabetes obese patients. It also significantly reduces SAT and VAT while alleviating ectopic fat deposition. MRI-PDFF represents a non-invasive tool for continuous assessment of lipid content changes following treatment.
Type 2 diabetes is closely associated with obesity and non-alcoholic fatty liver disease. Glucagon-like peptide-1 (GLP-1) receptor agonists such as semaglutide and loxenatide have been demonstrated to play a crucial role in glycemic control, obesity mitigation, and improvement in hepatic fat deposition1,2. However, it is currently unknown which of these two drugs has a superior effect in improving lipid metabolism. Therefore, the precise measurement of fat content in various visceral organs and adipose tissues, as well as the lipid alterations following the administration of GLP-1 receptor agonists, holds paramount clinical significance. The gold standard for determining histological fat content primarily relies on invasive pathological biopsies3, while magnetic resonance imaging proton-density-fat fraction (MRI-PDFF) could potentially serve as a non-invasive, continuous tool for evaluating changes in lipid content in diabetic patients when using semaglutide and loxenatide4.
METHODS
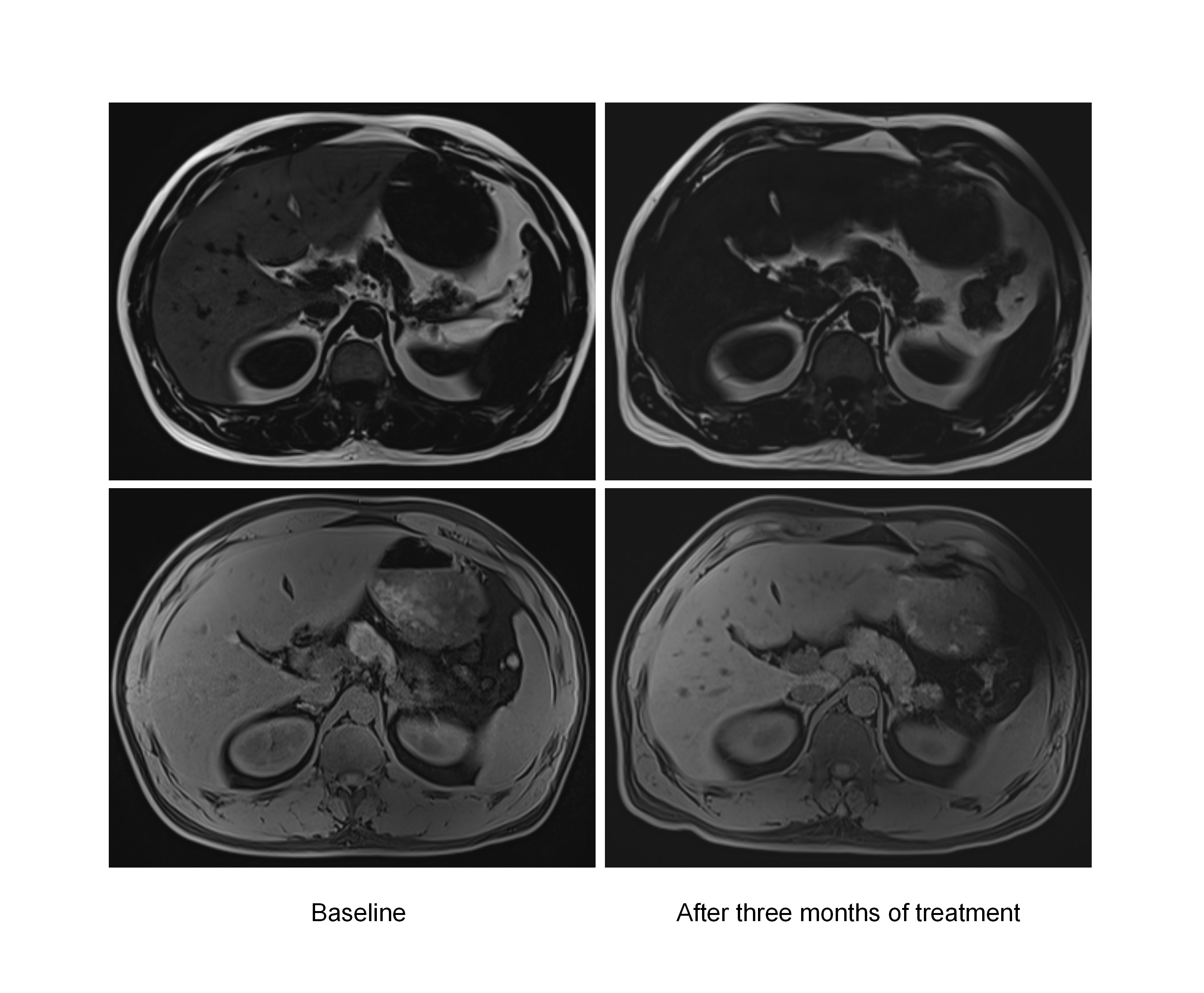
This study enrolled 21 newly diagnosed male obese patients with diabetes between June 2022 and December 2023. All participants were randomly divided into two groups: the semaglutide group (n=12) and the loxenatide group (n=9), and they received continuous treatment for three months. Clinical data for the patients were collected, and full abdominal-pelvic magnetic resonance scans were conducted using a 3.0T magnetic resonance scanner (Vida; Siemens Medical Solutions) both before and after three months of treatment. The scanning sequences consisted of T1-weighted imaging (T1WI), T2-weighted imaging (T2WI), and MRI-PDFF. On T2WI, the areas of subcutaneous adipose tissue (SAT) and visceral adipose tissue (VAT)were measured at the level of the third lumbar vertebra for all enrolled patients. At the pancreatic level, three regions of interest were selected for visceral fat, subcutaneous fat, liver, kidneys, and pancreas, and their average fat content was calculated.
RESULTS
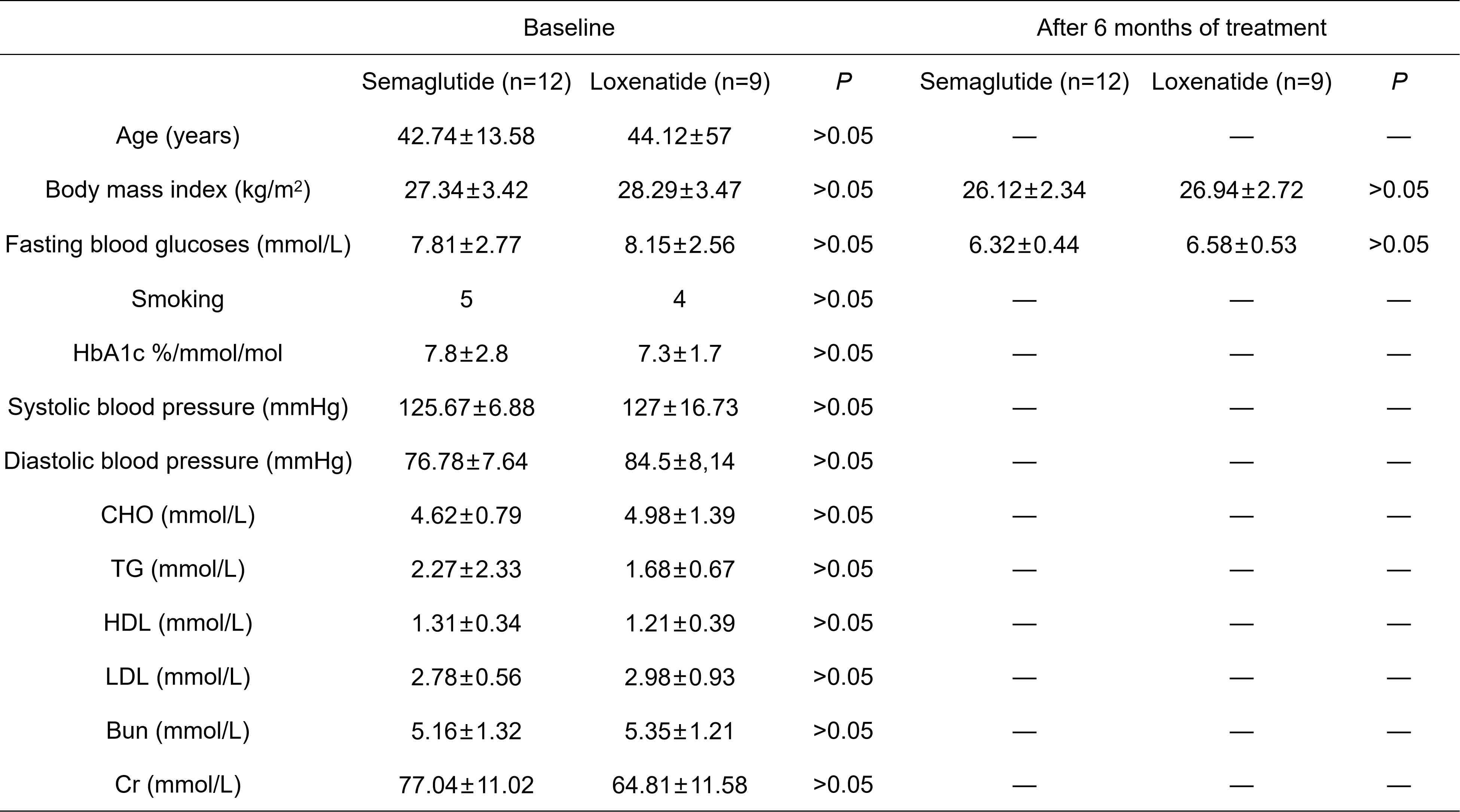
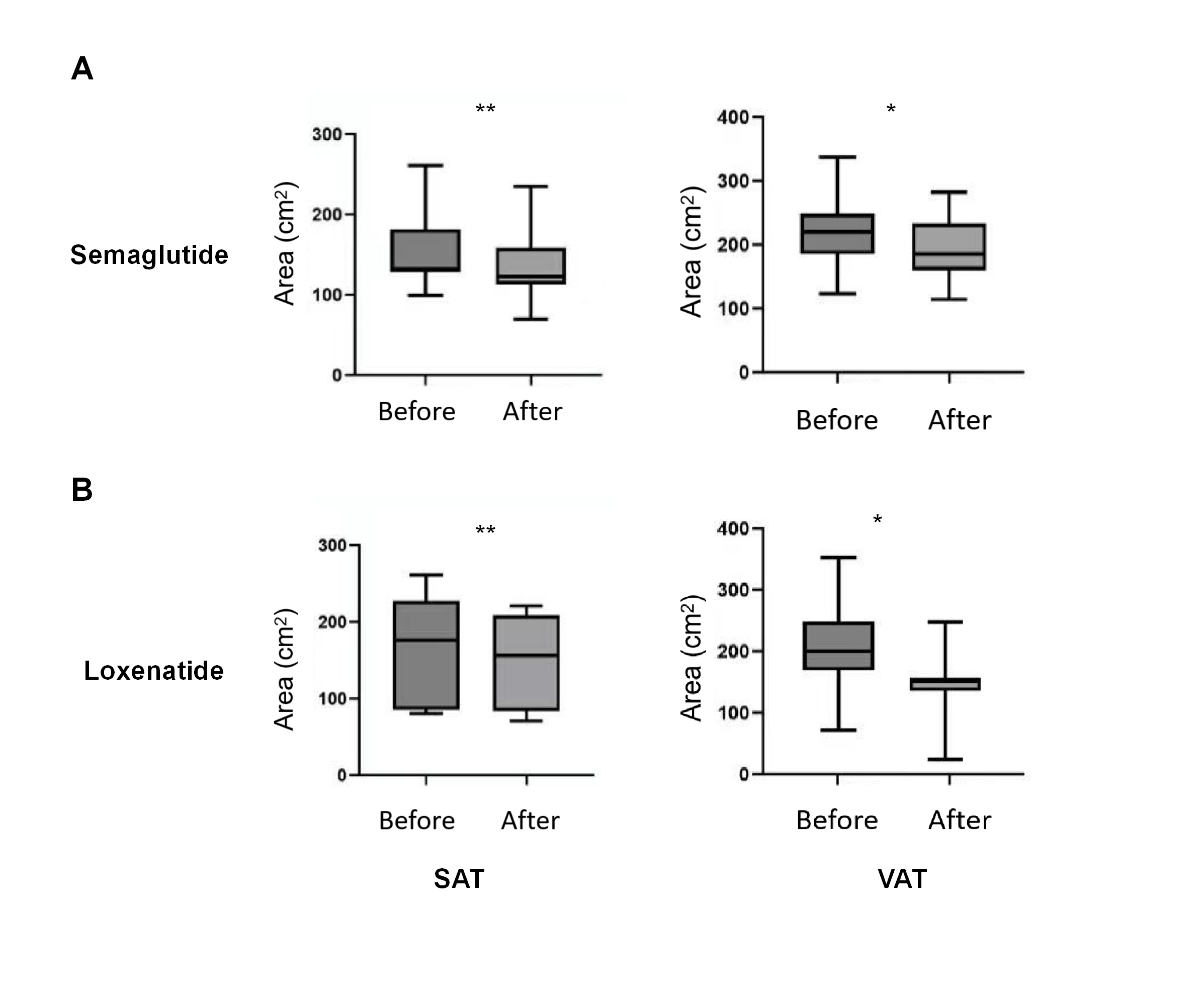
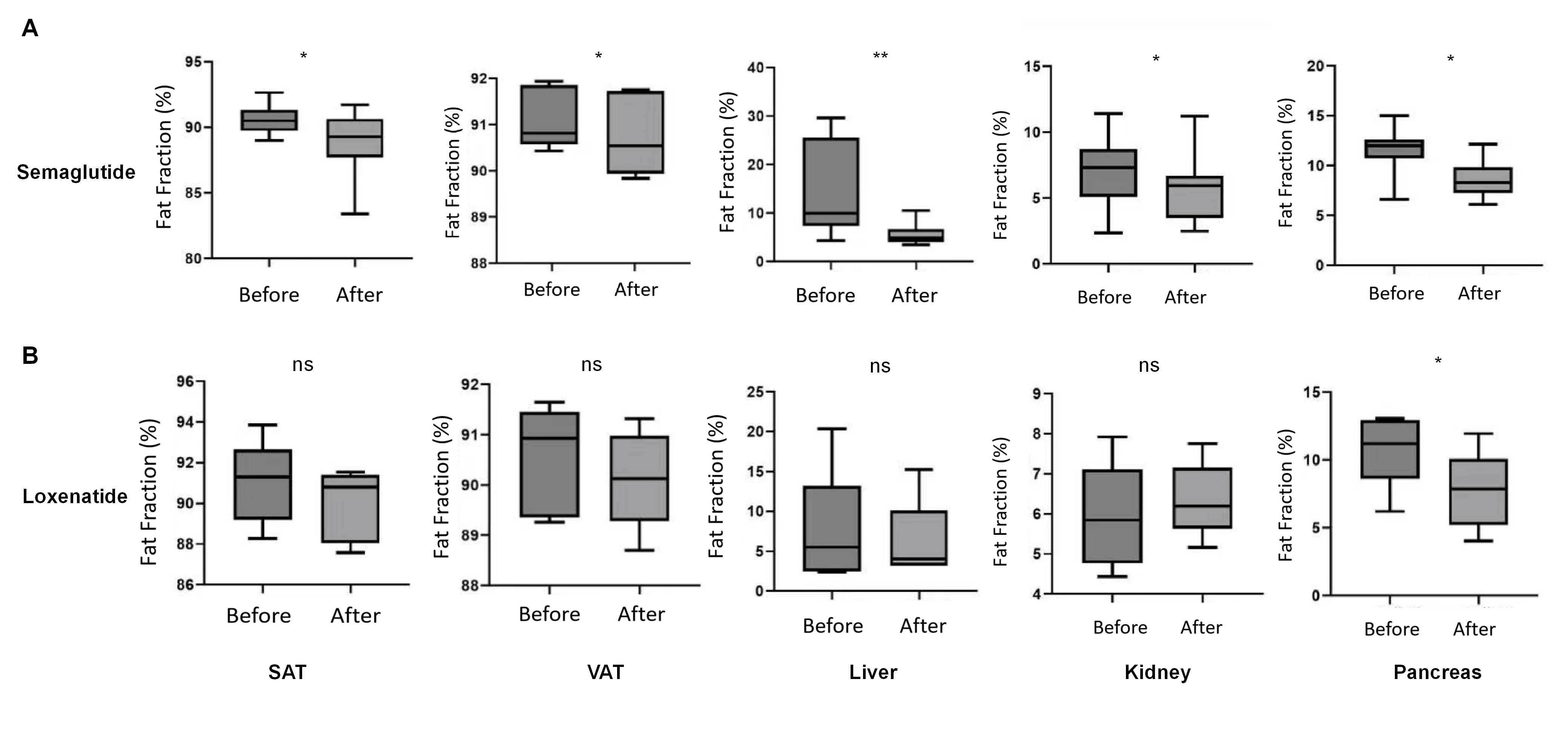
Figure 1 summarizes the clinical characteristics of the two patient groups. Compared to baseline, significant improvements were observed in body weight (Semaglutide: P<0.05; Loxenatide: P<0.05) and fasting blood glucose (Semaglutide: P<0.05; Loxenatide: P<0.05) for both groups. Quantitative analysis of T2-weighted images showed that at baseline, there were no statistically significant differences in SAT (Semaglutide vs. Loxenatide: 153.73±53.23 cm² vs. 160.59±42.58 cm², P>0.05) and VAT (Semaglutide vs. Loxenatide: 222.37±73.88 cm² vs. 182.84±69.37 cm², P>0.05) areas between the two groups. However, after treatment, both groups exhibited a significant reduction in SAT (Semaglutide: 137.54±42.91 cm², P<0.05; Loxenatide: 148.5±53.13 cm², P<0.05) and VAT (Semaglutide: 195.28±51.03 cm², P<0.05; Loxenatide: 148.51±46.24 cm², P<0.05) compared to baseline, as demonstrated in Figures 2 and 3. In the Semaglutide group, fat fraction in SAT (Before: 90.62%[IQR:90.10-91.15%], After: 88.80%[IQR:87,12-90.25%], P<0.05), VAT (Before: 90.80%[IQR:90.63-91.85%], After: 90.1%[IQR:89.23-91.34%], P<0.05), liver (Before: 9.98%[IQR:8.28-24.45%], After: 5.37%[IQR:4.29-6.29%], P<0.01), kidneys (Before: 7.12%[IQR:5.14-8.69%], After: 6.29%[IQR:4.10-5.45%], P<0.05), and pancreas (Before: 11.84%[IQR:6.73-12.55%], After: 8.23%[IQR:7.16-9.06%], P<0.05) significantly decreased compared to baseline, while in the Loxenatide group, only pancreatic fat fraction (Before: 11.26%[IQR:8.73-12.52%], After: 7.48%[IQR:5.26-9.66%], P<0.05) showed a significant reduction, as depicted in Figure 4.
DISCUSSION
For newly diagnosed obese patients with type 2 diabetes, both semaglutide and loxenatide have shown promising results in glycemic control and weight reduction. T2WI analysis revealed a significant reduction in SAT and VAT fat for both semaglutide and loxenatide. Analysis of organ fat fractions through MRI-PDFF indicated that, in comparison to loxenatide, semaglutide exhibited superior efficacy in improving ectopic fat deposition, particularly in cases of fatty liver. This suggests that MRI-PDFF may provide a more sensitive means of detecting treatment-related fat changes compared to histological assessments.
CONCLUSION
Semaglutide effectively controls fasting blood glucose and reduces body weight in obese individuals with type 2 diabetes. It also significantly reduces SAT and VAT while alleviating ectopic fat deposition in visceral organs. MRI-PDFF represents a non-invasive tool for continuous assessment of lipid content changes in diabetes patients following treatment.
Acknowledgements
This study has received funding by National Nature Science Foundation of China (81871412 and 82272064), Jiangsu Provincial Science and Technique Program (BK20221461), Postgraduate Research & Practice Innovation Program of Jiangsu Province (KYCX21_0159, KYCX22_0297, and KYCX23_0323).References
1.Campbell JE, Müller TD, Finan B, et al. GIPR/GLP-1R dual agonist therapies for diabetes and weight loss-chemistry, physiology, and clinical applications. Cell Metab. 2023;35(9):1519-1529.2.Newsome PN, Ambery P. Incretins (GLP-1 receptor agonists and dual/triple agonists) and the liver. J Hepatol. 2023:S0168-8278(23)05046-8.
3.Nauck MA, Wefers J, Meier JJ. Treatment of type 2 diabetes: challenges, hopes, and anticipated successes. Lancet Diabetes Endocrinol. 2021;9(8):525-544.
4.Tamaki N, Ajmera V, Loomba R. Non-invasive methods for imaging hepatic steatosis and their clinical importance in NAFLD. Nat Rev Endocrinol. 2022;18(1):55-66.
Figures