4722
Value of intravoxel incoherent motion magnetic resonance imaging in evaluating renal fibrosis in rabbits with renal artery stenosis1Radiology, Third Affiliated Hospital of Soochow University, Changzhou, China, 2Philips Healthcare, Shanghai, China, Shanghai, China
Synopsis
Keywords: Small Animals, Quantitative Imaging
Motivation: Intravoxel incoherent motion (IVIM) imaging can evaluate tissue microperfusion and diffusion information respectively, which can more accurately evaluate renal fibrosis (RF) in chronic kidney disease.
Goal(s): IVIM can reflect the occurrence and development of RF from two aspects of perfusion and diffusion respectively. It has a great application prospect for the evaluation of RF.
Approach: The dynamic changes of renal cortical and medullary signal with the progression of fibrosis were monitored by IVIM, and the compensatory effect of the contralateral kidney was analyzed.
Results: Some IVIM parameters of the renal cortex and medulla were moderately or strongly negatively correlated with RF.
Impact: Early detection and dynamic evaluation of the process of RF are crucial for reversing renal function damage. IVIM can reflect the development of RF from two aspects of perfusion and diffusion, which has a great application prospect for evaluating RF.
Introduction
Chronic kidney disease (CKD) has become a global public health problem[1]. Most CKD will inevitably develop into chronic renal failure due to renal fibrosis (RF). Early detection and dynamic evaluation of the process of RF are essential for reversing renal function damage and improving the quality of life of CKD patients[2-4]. The monitoring RF process has always relied on renal biopsy, but it is difficult to repeat because of sampling bias, potential bleeding and other complications, which cannot meet the needs of dynamic observation. Serological indicators also cannot reflect single renal function[5]. Intravoxel incoherent motion (IVIM) imaging can evaluate tissue microperfusion and diffusion information respectively, which can more accurately reveal the interaction between water molecular motion and tissue structure[6-10]. It has been used to evaluate renal function damage and graft fibrosis[11-12]. We aimed to use IVIM to monitor the dynamic changes of renal cortical and medullary signal with the progression of fibrosis, and analyze the compensatory effect of the contralateral kidney, which could provide a non-invasive and reliable imaging method for the early diagnosis, accurate staging and efficacy evaluation of RF.Methods
The rabbit RF model was established by left renal artery stenosis. The rabbits were randomly divided into control group (n=8) and RF group (n=70). The IVIM sequence scanning were conducted in Philips Ingenia 3T MR scanner (Philips, Ingenia, Netherlands) with a 16-channel head and neck coil. IVIM was acquired using echo planar imaging (EPI) sequence. The IVIM parameters were: TR/TE = 3000/75 ms; FOV = 150×150 mm; scan matrix = 68×68; 8 slices; b = 0, 10, 20, 50, 100, 200, 400, 600, 800 and 1200 s/mm2. IVIM images were analyzed by MITK Diffusion post-processing software. All rabbits were sacrificed immediately after the last MR Examination for Masson staining. The average percentage of fiber area over the total cross-sectional area was calculated using Image J software. SPSS 26.0 and GraphPad Prism 9.4 software were used for statistical analysis. The differences of IVIM parameters of bilateral renal cortex and medulla between groups were compared by independent sample t test. Spearman correlation analysis was used to compare the correlation between the IVIM parameters and the degree of RF. The receiver operating characteristic (ROC) curve was used to determine the efficacy of IVIM parameters of left renal cortex and medulla for the diagnosis and staging of RF.Results
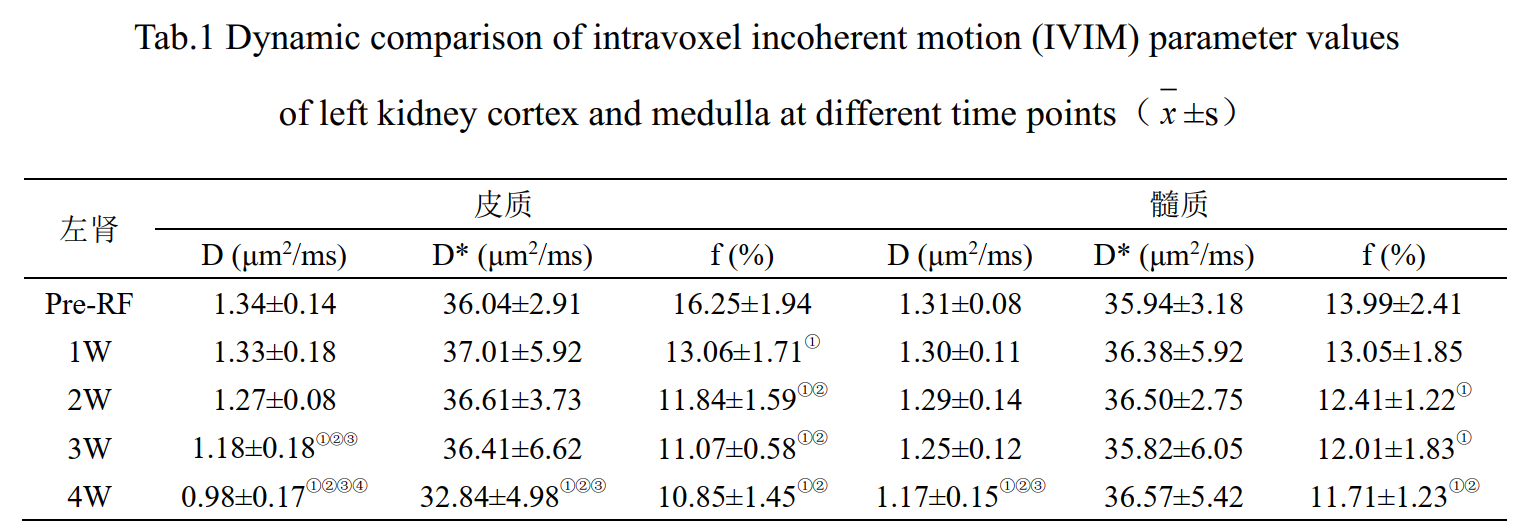
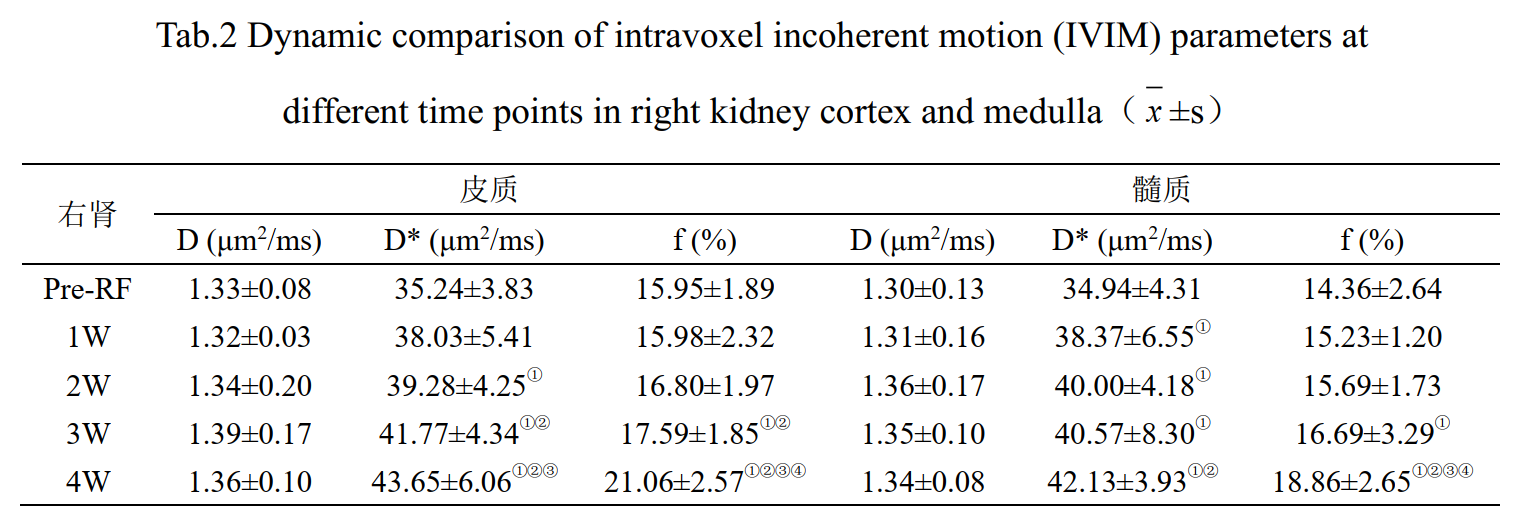
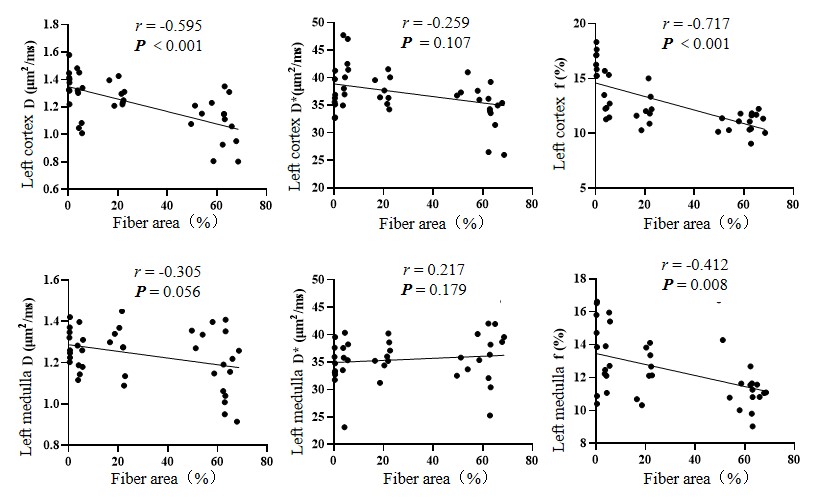
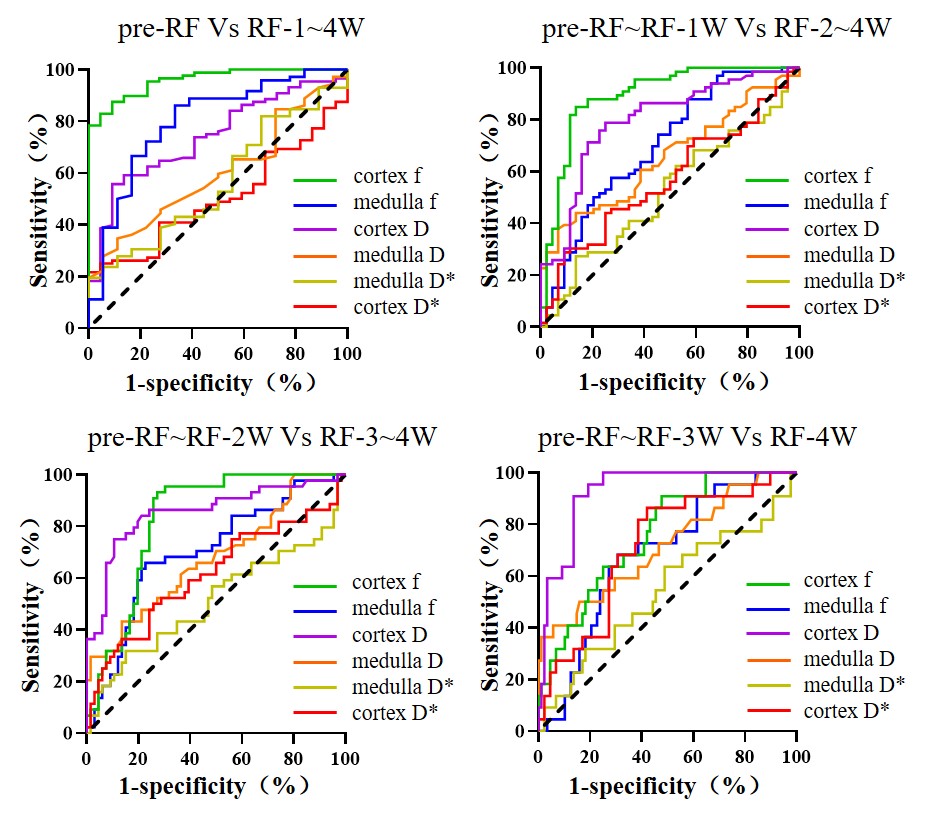
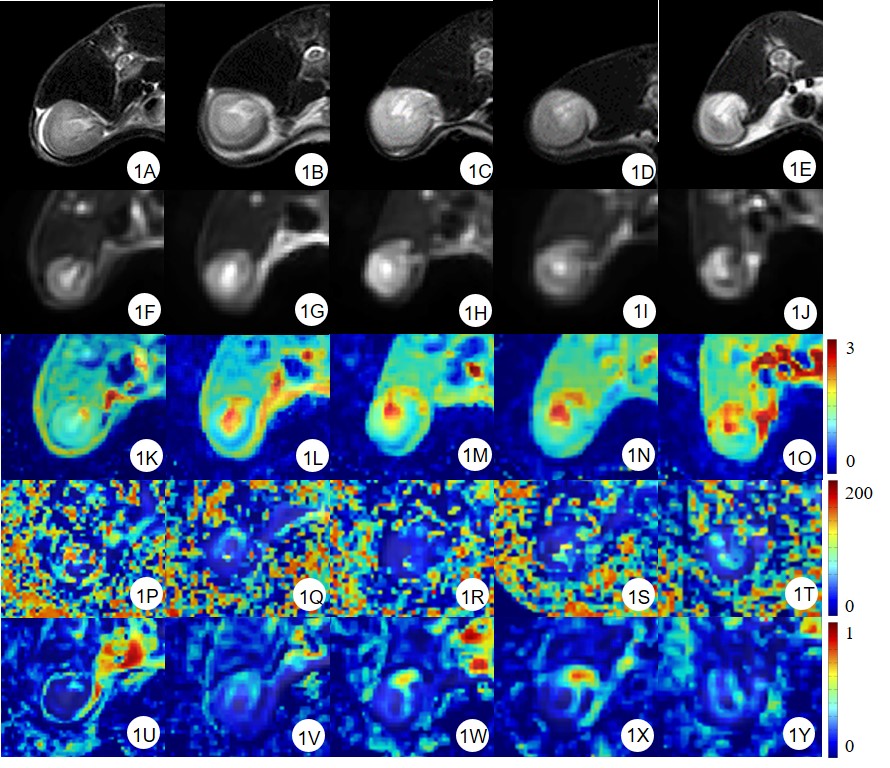
With the progression of RF, the boundary between cortex and medulla was not clear, and the IVIM image signal decreased gradually (Figure 1). In the RF group, The D* values of left renal cortex were significantly different between RF-4W and (pre-RF, RF-1-2W) subgroups. The f values of the left renal cortex and medulla in the pre-RF, RF-3W and 4W subgroups were statistically different (Table 1). The f values of the right renal cortex and medulla in the pre-RF and RF-4W subgroups were statistically different (Table 2). Spearman correlation test showed that the D and f values of left renal cortex and the f value of left renal medulla were moderately or strongly negatively correlated with the degree of RF (r = -0.595, -0.717, -0.412, P all <0.01) (Figure 2). The f value was the best to identify pre-RF and RF-1-4W, pre-RF~RF-1W and RF-2-4W. The D value was the best to identify pre-RF~RF-2W and RF-3~4W, pre-RF~RF-3W and RF-4W (Figure 3).Discussion
The increase of interstitial fibroblasts and deposition of collagen fibers in the kidney hinder the diffusion of water in the interstitium, resulting in a continuous decrease of D. At the same time, it induces the activation of renin-angiotensin system, which promotes vasoconstriction and decreases the f value. The contralateral (right) kidney has a compensatory effect. Due to the progressive loss of left renal function, the perfusion of the right kidney increased gradually, and also the rate of fluid infusion, resulting in the gradual increase of the D* and f values of the right kidney cortex and medulla. Long-term dynamic observation of the contralateral healthy kidney has important implications for the prognosis of the patient. After RF initiation, capillary loss and hypoperfusion are both key features of fibrotic kidneys and drivers of further fibrotic injury[13]. The f may be the most sensitive marker of RF among the three parameters of IVIM. The f and D can be used as reliable indicators for early diagnosis and accurate staging of RF. Conclusion: IVIM can evaluate the dynamic changes of microcirculation reduction and interstitial collagen deposition in RF from two levels of perfusion and diffusion, which provides imaging evidence for long-term monitoring and clinical management of RF.Acknowledgements
No acknowledgement found.References
1. WANG F, OTSUKA T, ADELNIA F, et al. Multiparametric magnetic resonance imaging in diagnosis of long-term renal atrophy and fibrosis after ischemia reperfusion induced acute kidney injury in mice. NMR Biomed. 2022, 35(10): e4786.
2. KIM S Y, KIM H, LEE J, et al. Quantitative magnetic resonance imaging of chronic kidney disease: an experimental in vivo study using rat chronic kidney disease models. Acta Radiol. 2023, 64(1): 404-414.
3. WU J, SHI Z, ZHANG Y, et al. Native T1 mapping in assessing kidney fibrosis for patients with chronic glomerulonephritis. Front Med (Lausanne). 2021, 8:772326.
4. WANG F, QIN S, CAI B, et al. Promising therapeutic mechanism for Chinese herbal medicine in ameliorating renal fibrosis in diabetic nephropathy. Front Endocrinol (Lausanne). 2023, 14:932649.
5. GONZALEZ J, JATEM E, ROIG J, et al. Usefulness of urinary biomarkers to estimate the interstitial fibrosis surface in diabetic nephropathy with normal kidney function. Nephrol Dial Transplant. 2022, 37(11): 2102-2110.
6. MIR M C, CAMPBELL R A, SHARMA N, et al. Parenchymal volume preservation and ischemia during partial nephrectomy: Functional and volumetric analysis. Urology. 2013, 82(2): 263-269.
7. FRIEDLI I, BAID-AGRAWAL S, UNWIN R, et al. Magnetic Resonance Imaging in Clinical Trials of Diabetic Kidney Disease. J Clin Med. 2023, 12(14): 4625. 8. ZHANG Z, CHEN Y, ZHOU X, et al. The value of functional magnetic resonance imaging in the evaluation of diabetic kidney disease: a systematic review and meta-analysis. Front Endocrinol (Lausanne). 2023, 14: 1226830.
9. YU Y M, WANG W, WEN J, et al. Detection of renal allograft fibrosis with MRI: arterial spin labeling outperforms reduced field-of-view IVIM. Eur Radiol. 2021, 31(9): 6696-6707.
10. PHI V V, REINER, C S, KLARHOE M, et al. Diffusion tensor imaging of the abdominal organs: Influence of oriented intravoxel flow compartments. NMR Biomed. 2019, 32(11): e4159.
11. ZHANG J, YU Y, LIU X, et al. Evaluation of Renal Fibrosis by Mapping Histology and Magnetic Resonance Imaging. Kidney Dis (Basel). 2021, 7(2): 131-142.
12. BANE O, HECTORS S J, GORDIC S, et al. Multiparametric magnetic resonance imaging shows promising results to assess renal transplant dysfunction with fibrosis. Kidney Int. 2020, 97(2): 414-420.
13. YU Y, NI Q, WANG Z, et al. Multiparametric Functional Magnetic Resonance Imaging for Evaluating Renal Allograft Injury. Korean J Radiol. 2019, 20(6):894-908.
Figures