4721
Evaluating Fetoplacental Response to Hypercapnia in Pregnant Rats: A comparison between T2* MRI and Photoacoustic Imaging1Biomedical engineering and physics, Amsterdam UMC, location University of Amsterdam, Amsterdam, Netherlands, 2Department of CDL research, University Medical Center Utrecht, Utrecht, Netherlands, 3Department of Obstetrics, University Medical Center Utrecht, Wilhelmina Children’s Hospital, Utrecht, Netherlands
Synopsis
Keywords: Small Animals, Oxygenation
Motivation: T2* MRI and photoacoustic imaging (PAI) offer non-invasive oxygenation measures, but their comparative effectiveness for placental study remains untested.
Goal(s): Our goal was to directly compare T2* MRI and PAI's ability and effectiveness to assess placental and fetal organ oxygenation responses under normoxic hypercapnia challenge.
Approach: Using pregnant rats, the study involved sequential scans of fetoplacental units with T2* MRI and PAI under normoxic hypercapnia challenge.
Results: We found discrepancies between MRI and PAI in detecting oxygenation changes. MRI displayed a marked response in placental oxygenation, not as prominently reflected in PAI measurements.
Impact: T2* MRI could accurately captures fetoplacental responses to hypercapnia, outperforming photoacoustic imaging. Investigating this performance gap is essential before combining these techniques in preeclampsia and fetal growth restriction studies.
Introduction
Preeclampsia (PE) and fetal growth restriction (FGR) are complex pregnancy-related conditions resulting from placental insufficiency. In the absence of a cure and relying on monitoring strategies, there is a clear need for animal models alongside advanced preclinical imaging techniques 1–3, allowing non-invasive assessment of relevant outcome parameters such as hemodynamic stress, microvascular function and oxygenation in placenta and fetal organs. In this respect, T2* MRI is commonly used as it is sensitive to oxy/deoxy-hemoglobin changes. More recently, photoacoustic imaging (PAI) was introduced, which could provide direct quantitative estimates of oxygenation in real-time based on the differences in the photoacoustic effect between oxy- and deoxyhemoglobin. However, a comparison between these techniques to study placental oxygenation has never been performed. The aim of this study was therefore to provide a direct comparison between T2* MRI and PAI in assessing oxygenation responses in placenta and fetal organs modulated by a normoxic hypercapnia challenge.Methods
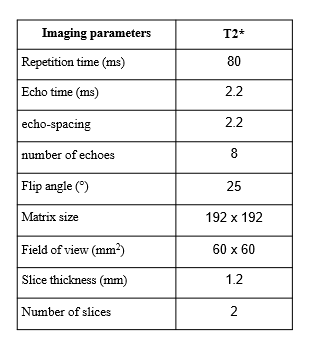
Pregnant Sprague Dawley rats (n=6) were subjected to a CO2 challenge at gestation days (GD) 18 and 19. For each rat, while under isoflurane anesthesia, several fetoplacental units were scanned sequentially using both MRI and PAI. During the procedures for both MRI and PAI, the gas supplied to the pregnant rats was adjusted from normoxia (21% O2, 79% N2) to normoxic hypercapnia conditions (5% CO2, 21% O2, 74% N2), and then reverted to normoxia.MRI measurements were performed with a 7T small animal scanner (MR Solutions, Guildford, UK). First, multi-slice T2-weighted anatomical imaging was performed to localize the placentas. For several of the fetuses, multi-slice respiratory-gated T2*-weighted MRI (Table 1) was performed for a total of 21 dynamics and total acquisition time of 12-15 min. Multi-gradient-echo data were reconstructed with BART4 toolbox using temporal regularization for all dynamics, after which quantitative T2* maps were calculated for each dynamic.
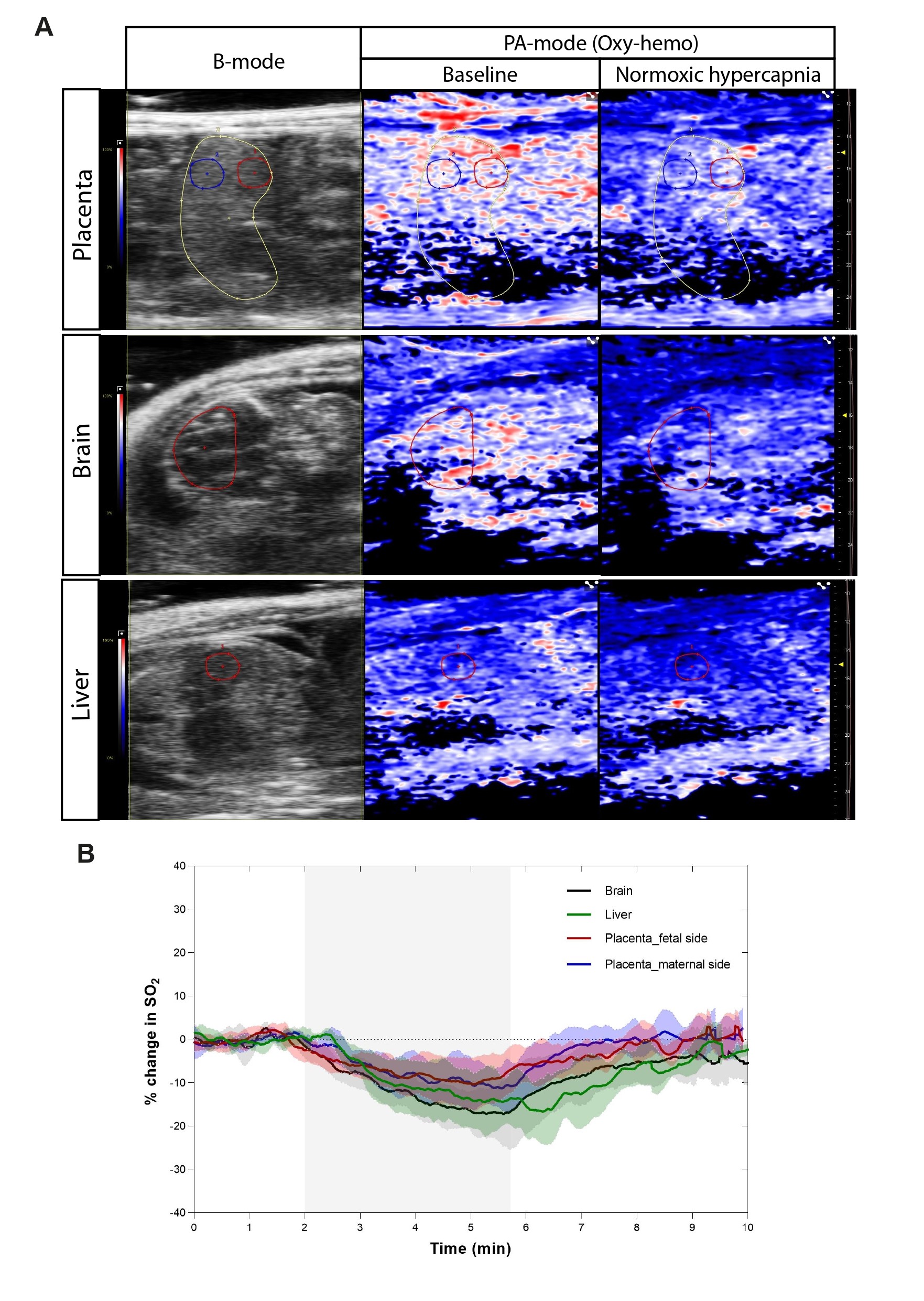
PAI was performed using a 21 MHz probe (LZ-250; 75 μm axial resolution) connected to the VevoLAZR PA imaging system (Fujifilm Visualsonics Inc., Toronto, Canada). For each high-resolution scan, light from the laser was directed onto the uppermost fetoplacental units, which were positioned at the optical focus between 10 and 15 mm. Data for SaO2 was specifically collected at two wavelengths, 750 nm and 850 nm, in the Oxyhemo mode.
Results
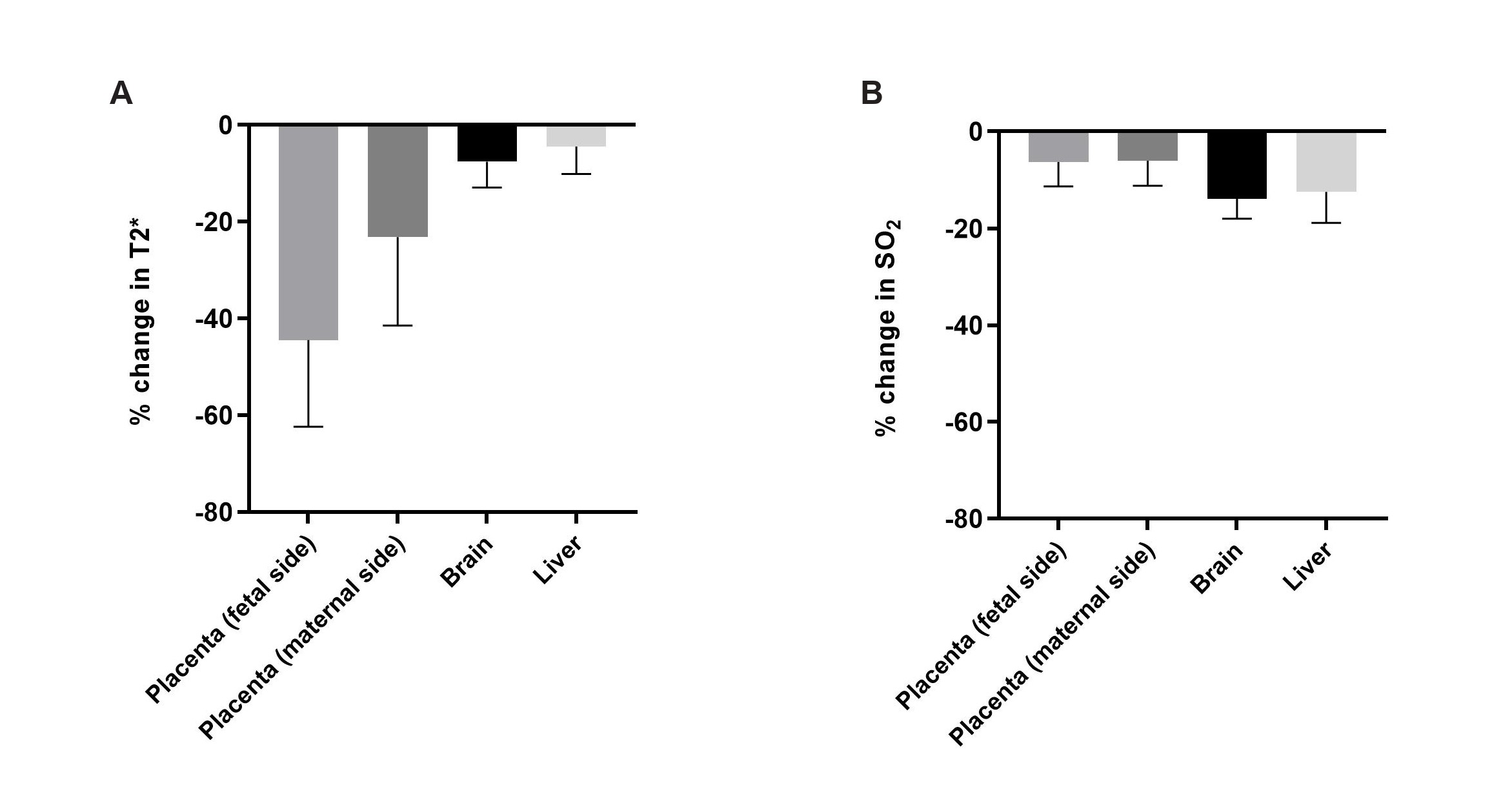
Upon exposure to normoxic hypercapnia, MRI measurements (Figure 1) showed a significant reduction in T2* by 44.4±17.9% (p=0.003) in the placenta's fetal side exhibited, which was larger compared to the maternal side (23.2±18.3%; p=0.084). Interestingly, MRI revealed much larger effects compared to PAI, the latter showing only a reduction in oxygenation values of 6.3±5.1% (p=0.043) and 6.0±5.2% (p=0.056) in the placenta’s fetal and maternal side respectively (Figure 2). Figure 3 shows all results including those from fetal organs. More specifically, fetal liver revealed no significant reduction of T2* during the hypercapnic challenge (4.4±5.6%; p=0.117), whereas PAI revealed a small effect on oxygenation values (12.5±6.2%; p=0.039). Similar changes were observed for the fetal brain, with T2* and PAI oxygenation changes of 7.6±5.3% (p=0.020) and 13.9±4.0% (p<0.001), respectively.Discussion and Conclusion
Interestingly, our results do not show comparable changes in oxygenation between MRI and PAI after normoxic hypercapnia. Specifically, T2* MRI displayed a pronounced response from the placenta, likely due to enhanced sensitivity to the paramagnetic properties of deoxyhemoglobin in the whole tissue. The potential difficulty of PAI to detect the full extent of changes in the placenta might stem from its indirect measurement of hemoglobin concentrations via optical absorption of light in the blood, which could be affected by the preferential absorption in larger blood vessels, obscuring the absorption at the capillary level.Our findings did not align with a prior study suggesting brain-sparing mechanisms when examining the impact of normoxic hypercapnia on pregnant animals anesthetized with pentobarbital using T2* MRI1. Nevertheless, the observed changes in the fetal side of the placentas in our research mirrors the alterations seen in the placentas in the referenced study, both showing an approximate change of 44%.
Additionally, our findings reveal the flexibility of fetoplacental blood flow, evident from the swift onset and subsequent reversal of alterations in oxygenation metrics. This research highlights the ability of T2* MRI to accurately capture these physiological changes. In conclusion, MRI and PAI do not show comparable oxygenation changes in placenta and fetal organs after a hypercapnic challenge. Our results warrant further investigations to understand the source of these differences, before these techniques can be used as complementary techniques to study PE and FGR.
Acknowledgements
No acknowledgement found.References
1. Ginosar Y, Gielchinsky Y, Nachmansson N, et al. BOLD-MRI demonstrates acute placental and fetal organ hypoperfusion with fetal brain sparing during hypercapnia. Placenta. 2018;63:53-60. doi:10.1016/j.placenta.2017.09.005
2. Ganesh T, Estrada M, Yeger H, Duffin J, Margaret Cheng HL. A non-invasive magnetic resonance imaging approach for assessment of real-time microcirculation dynamics. Sci Reports 2017 71. 2017;7(1):1-11. doi:10.1038/s41598-017-06983-6
3. Arthuis CJ, Novell A, Raes F, et al. Real-Time Monitoring of Placental Oxygenation during Maternal Hypoxia and Hyperoxygenation Using Photoacoustic Imaging. Zenclussen AC, ed. PLoS One. 2017;12(1):e0169850. doi:10.1371/journal.pone.0169850
4. Martin Uecker, Frank Ong, Jonathan I Tamir, Dara Bahri, Patrick Virtue, Joseph Y Cheng, Tao Zhang, and Michael Lustig, Berkeley Advanced Reconstruction Toolbox, Annual Meeting ISMRM, Toronto 2015, In Proc. Soc. Mag. Reson. Med. 23:2486
Figures