4718
Radiomics for Deep Brain Stimulation outcome prediction using Quantitative Susceptibility Mapping (RadDBS-QSM)1Electrical and Computer Engineering, Cornell University, New York, NY, United States, 2Electrical and Computer Engineering, Johns Hopkins University, Baltimore, MD, United States, 3Radiology, Weill Cornell Medicine, New York, NY, United States, 4Biomedical Engineering, Cornell University, New York, NY, United States, 5Neurosurgery, Mount Sinai Hospital, New York, NY, United States, 6Changhai Hospital, Shanghai, China
Synopsis
Keywords: Diagnosis/Prediction, Radiomics
Motivation: To improve outcome prediction for deep brain stimulation (DBS) surgery using radiomic features on quantitative susceptibility maps (QSMs).
Goal(s): To address the inconsistent levodopa challenge test (LCT) prediction for DBS outcomes by describing the target variable, motor symptom improvement, as a weighted sum of QSM radiomic features.
Approach: A least absolute shrinkage and selection operator (LASSO) model is implemented, trained, and tested on patient data and known DBS outcomes.
Results: Model predictions outperform the conventional LCT prediction and estimate DBS improvement from preoperative motor symptom scores and radiomic features on QSM.
Impact: The levodopa challenge test estimates patient response to deep brain stimulation surgery, presenting undesirable side effects and inconsistent outcomes. Radiomic prediction of deep brain surgery outcomes using quantitative susceptibility maps aims to provide a numerical measure of symptom improvement.
Introduction
Deep brain stimulation (DBS) is a treatment for motor symptoms and dyskinesia in advanced Parkinson’s disease.1 Patient selection is determined by the preoperative levodopa challenge test (LCT),2 widely documented as an inconsistent predictor for DBS improvements.3,4 As the surgery is complex and costly, there is a need to accurately predict DBS outcomes as measured by the improvement in a patient’s UPDRS-III4 scores before and after the procedure. Prior work demonstrates correlation between specific radiomic features in quantitative susceptibility maps (QSM)5,6 and classification of DBS outcomes.7 In this work, it is demonstrated that radiomic features obtained from QSMs can accurately predict specific numerical DBS outcomes.Theory
Continuous outputs can be predicted from least absolute shrinkage and selection operator (LASSO) model of the form: $$w^*=\mathrm{argmin}\frac{1}{2N} ||U-X_{\Phi}w||^2_2+\lambda||w||_1$$ Where $$$N$$$ is the sample size, $$$U$$$ is the target prediction, $$$N \times 1$$$ $$$X_{\Phi}$$$ is the feature matrix $$$(N \times M)$$$ where $$$M$$$ is the product of the number of features $$$P$$$ and number of regions of interest (ROIs) $$$R$$$ and the weights $$$w$$$ are $$$M \times 1$$$. Weights $$$\hat{w}$$$ can also be computed given a set of augmented features $$$\hat{X_{\Phi}}$$$ and targets $$$\hat{U}$$$ from $$$\hat{N}$$$ samples. In synthetic data, dataset imbalance is addressed by assigning “rare” cases a high relevance value $$$\phi$$$ and remaining cases a low relevance value. The dataset is balanced by oversampling rare values and undersampling remaining values. Synthetic pairs $$$(\hat{X_{\Phi}},\hat{U})$$$ are generated by randomly selecting a $$$k$$$ nearest neighbor of a rare pair $$$(X_{\Phi},U)$$$ and adding a perturbation as outlined by SMOTER and SMOGN.8,9Methods
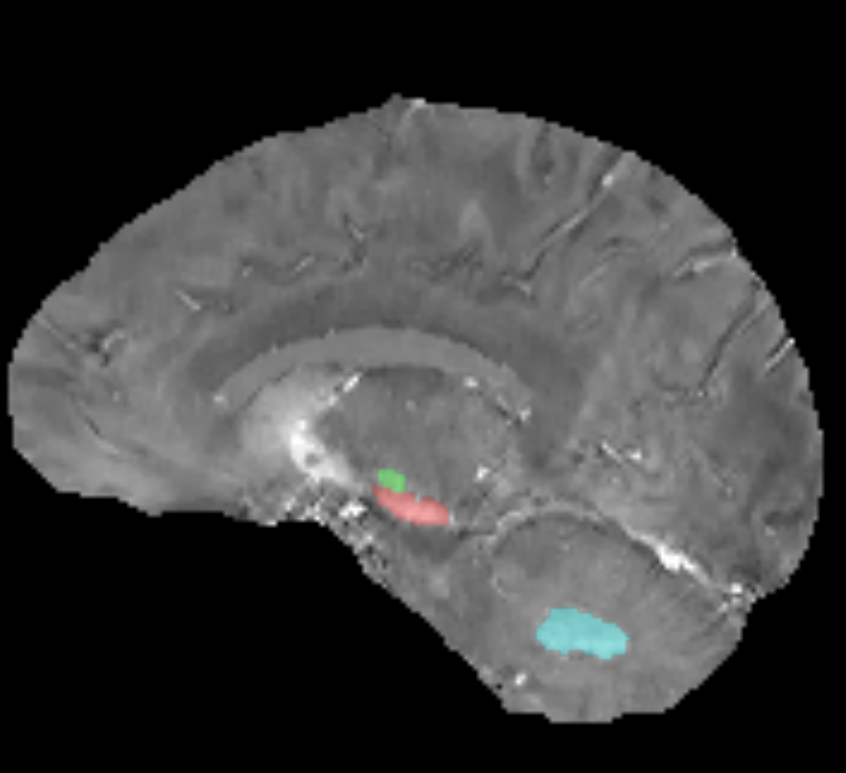
Data was collected across 2 sites. At Site 1, 35 candidates for DBS surgery were acquired with a multi-echo gradient echo (mGRE) sequence10 with 10 echoes, acquired resolution $$$0.8 \times 0.8 \times 1 mm^3$$$ interpolated to $$$0.5 mm^3$$$ resolution, acquisition matrix of $$$320 \times 320 \times 180$$$, acceleration factor of 2, repetition time $$$TR=44.1 ms$$$ and scan time of 13 minutes. At Site 2, 37 candidates were acquired using a bipolar mGRE sequence6 with 6 echoes, voxel size $$$0.9 mm^3$$$, acquisition matrix of $$$256 \times 256 \times 160$$$, acceleration factor of 2, $$$TR$$$ of $$$28 ms$$$. QSMs were reconstructed using MEDI-L111 and features were extracted using the pyradiomics12 pipeline from the substantia nigra, subthalamic nucleus, red nucleus, and dentate nucleus (Figure 1) in the QRadAR Toolbox.13 A LASSO14 model from the scikit-learn library15 was implemented. Data was augmented using SMOGN8 for dataset imbalance with relevance $$$\phi=1$$$ assigned to the patient with minimal and maximal improvements and a relevance of $$$\phi=0$$$ to median improvement following DBS surgery. The overall pipeline is shown in Figure 2. For regularization parameters, leave one out cross validation was performed on Site 2 data ($$$\lambda_{LASSO}=0.05$$$ and $$$\lambda_{LASSO+SMOGN}=0.06$$$) (Figure 3). Models were trained and tested on $$$N-1$$$ cases with the leave-one-out method on the Site 1 dataset (LASSO) and the augmented, synthetic $$$\hat{N}-1$$$ dataset (SMOGN+LASSO). Both models were tested on each omitted patient in the Site1 dataset $$$N$$$ times. Effect of resolution were assessed by downsampling the Site 1 data by 2 (Figure 4). Site 1 images were retrained using leave-one-out cross validation with 10 patients withheld (Figure 5). The predictive power of LCT, LASSO, and SMOGN+LASSO was evaluated using linear regression (correlation $$$r$$$, slope $$$m$$$, intercept $$$b$$$, significance $$$p$$$).Results
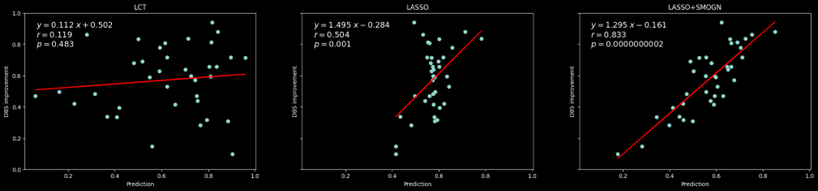
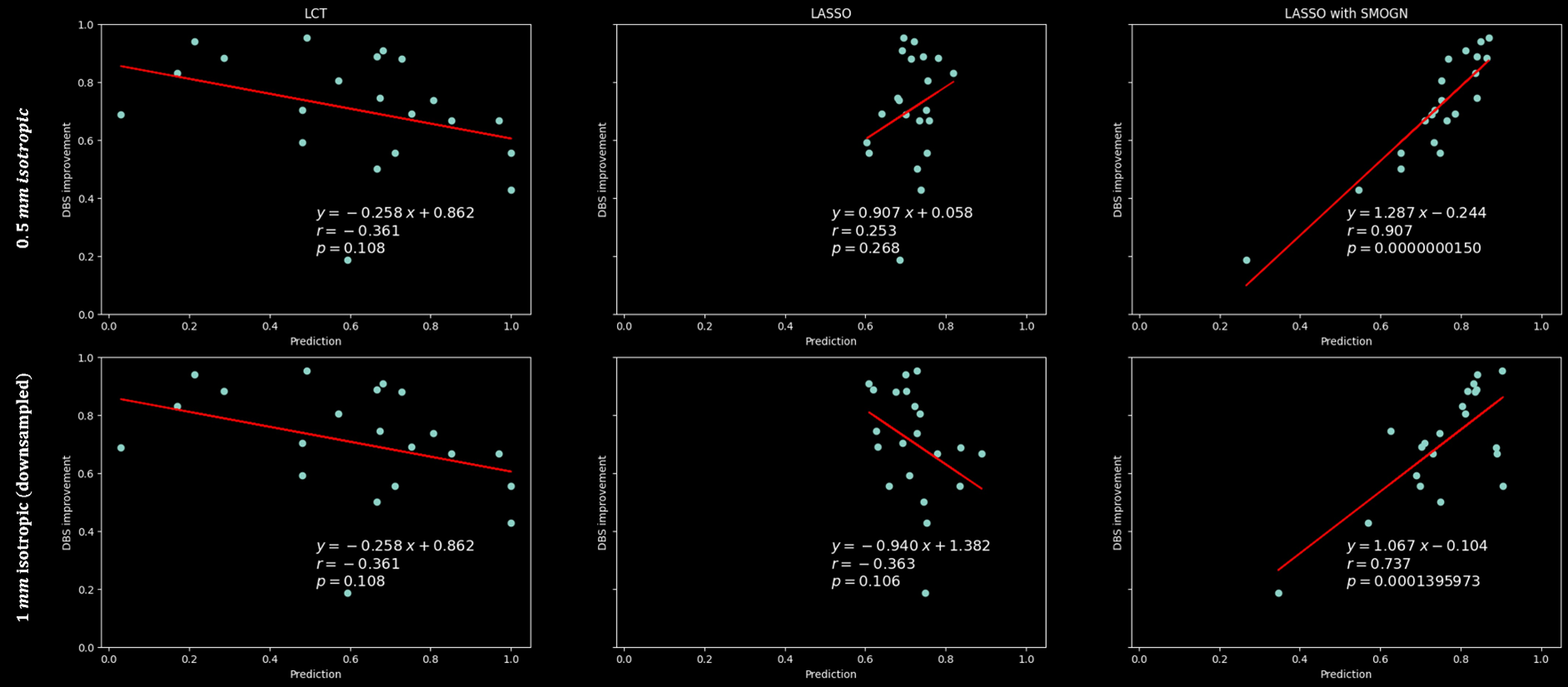
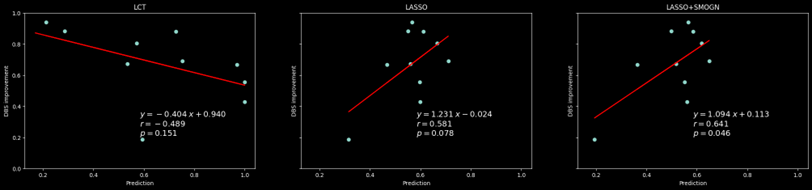
SMOGN+LASSO $$$(r=0.83, m=1.3, b=-0.16, p \approx 0)$$$ predicts outcomes in DBS and outperforms the LASSO model $$$(r=0.50, m=1.1, b=0.5, p < 0.01)$$$ trained on Site 2 dataset (Figure 3). Both outperform LCT $$$(r=0.12, m=-0.26, b=0.86, p=0.11)$$$ which shows no significant correlation (Figure 3). The Site 1 data demonstrate similar trends, LASSO+SMOGN $$$(r=0.91, m=1.3, b=-0.24, p \approx 0)$$$ outperforming LASSO $$$(r=0.25, m=0.91, b=0.06, p=0.27)$$$, with LCT $$$(r=-0.36, m=0.94, b=1.38 p \approx 0)$$$ (Figure 4). Downsampling degrades LASSO performance $$$(r=-0.36, m=0.94, b=1.38, p=0.11)$$$ (Figure 4). On a small number of withheld patients, LCT gives $$$(r=-0.49, m=-0.4, b=0.94, p=0.15)$$$, LASSO gives $$$(r=0.58, m=1.2, b=-0.024, p = 0.078)$$$ and LASSO+SMOGN gives $$$(r=0.64, m=1.09, b=-0.01, p=0.046)$$$ (Figure 5). Predictive features (nonzero LASSO weights) included wavelet decomposition skewness, minima, small gray level dependence, and local binary pattern gray level run length run variance over the substantia nigra, subthalamic nucleus, red nucleus and dentate nucleus.Conclusion
Radiomic features on QSM can improve the accuracy of DBS prediction as compared to LCT. The accuracy is shown to improve with spatial resolution, likely due to the presence of high-frequency wavelet decompositions in predictive features. Future directions include evaluating the effect of learned undersampling16 and super-resolution techniques17-22 on QSM radiomics predictions.Acknowledgements
No acknowledgement found.References
1. Groiss SJ, Wojtecki L, Südmeyer M, Schnitzler A. Review: Deep brain stimulation in Parkinson’s disease. Therapeutic Advances in Neurological Disorders. 2009;2(6):379-391. doi:10.1177/1756285609339382
2. Saranza G, Lang AE. Levodopa challenge test: indications, protocol, and guide. Journal of Neurology. 2020;doi:10.1007/s00415-020-09810-7
3. Lachenmayer ML, Mürset M, Antih N, et al. Subthalamic and pallidal deep brain stimulation for Parkinson’s disease—meta-analysis of outcomes. npj Parkinson's Disease. 2021;7(1)doi:10.1038/s41531-021-00223-5
4. Zaidel A, Bergman H, Ritov YA, Md ZI. Levodopa and subthalamic deep brain stimulation responses are not congruent. Movement Disorders. 2010;25(14):2379-2386. doi:10.1002/mds.23294 5. Huang W, Ogbuji R, Zhou L, Guo L, Wang Y, Kopell BH. Motoric impairment versus iron deposition gradient in the subthalamic nucleus in Parkinson’s disease. Journal of Neurosurgery. 2020;135(1):284-290. doi:10.3171/2020.5.jns201163
6. Zhao W, Yang C, Tong R, et al. Relationship Between Iron Distribution in Deep Gray Matter Nuclei Measured by Quantitative Susceptibility Mapping and Motor Outcome After Deep Brain Stimulation in Patients With Parkinson's Disease. Journal of Magnetic Resonance Imaging. 2023;58(2):581-590. doi:10.1002/jmri.28574
7. Liu Y, Xiao B, Zhang C, et al. Predicting Motor Outcome of Subthalamic Nucleus Deep Brain Stimulation for Parkinson's Disease Using Quantitative Susceptibility Mapping and Radiomics: A Pilot Study. Front Neurosci. 2021;15:731109. doi:10.3389/fnins.2021.731109
8. Branco P, Torgo L, Ribeiro RP. SMOGN: a pre-processing approach for imbalanced regression. PMLR; 2017:36-50.
9. Torgo L, Ribeiro RP, Pfahringer B, Branco P. SMOTE for Regression. Springer Berlin Heidelberg; 2013:378-389.
10. Dimov AV, Gupta A, Kopell BH, Wang Y. High-resolution QSM for functional and structural depiction of subthalamic nuclei in DBS presurgical mapping. Journal of Neurosurgery. 2019;131(2):360-367. doi:10.3171/2018.3.jns172145
11. De Rochefort L, Liu T, Kressler B, et al. Quantitative susceptibility map reconstruction from MR phase data using bayesian regularization: Validation and application to brain imaging. Magnetic Resonance in Medicine. 2010;63(1):194-206. doi:10.1002/mrm.22187
12. Van Griethuysen JJM, Fedorov A, Parmar C, et al. Computational Radiomics System to Decode the Radiographic Phenotype. Cancer Research. 2017;77(21):e104-e107. doi:10.1158/0008-5472.can-17-0339
13. Roberts AG, Romano D, Zhang J, et al. QRadAR: An Open-source Toolbox for Quantitative Magnetic Resonance Radiomics Analysis and Reproducibility. presented at: International Society of Magnetic Resonance in Medicine (Submitted); 2023; Singapore.
14. Tibshirani R. Regression Shrinkage and Selection Via the Lasso. Journal of the Royal Statistical Society: Series B (Methodological). 1996;58(1):267-288. doi:https://doi.org/10.1111/j.2517-6161.1996.tb02080.x
15. Pedregosa F, Varoquaux Ge, Gramfort A, et al. Scikit-learn: Machine Learning in Python. arXiv pre-print server. 2018-06-05 2018;doi:None arxiv:1201.0490
16. Zhang J, Nguyen TD, Solomon E, et al. <scp>mcLARO</scp>: Multi‐contrast learned acquisition and reconstruction optimization for simultaneous quantitative multi‐parametric mapping. Magnetic Resonance in Medicine. 2023;doi:10.1002/mrm.29854
17. Eskreis-Winkler S, Zhou D, Liu T, et al. On the influence of zero-padding on the nonlinear operations in Quantitative Susceptibility Mapping. Magnetic Resonance Imaging. 2017;35:154-159. doi:10.1016/j.mri.2016.08.020
18. Moevus AD, Mathieu; De Leener, Benjamin Improving Deep Learning MRI Super-Resolution for Quantitative Susceptibility Mapping. Magnetic Resonance in Medicine; 2021:
19. Roberts AG, Spincemaille P, Kovanlikaya I, Tsiouris AJ, Nguyen T, Wang Y. SWISeR: Multi-Field Susceptibility-Weighted Image Super-Resolution. presented at: International Society of Magnetic Resonance in Medicine; 2022; London, England.
20. Roberts AG, Zhang J, Spincemaille P, Nguyen T, Wang Y. SuperQ: 3D Super-Resolution of Quantitative Susceptibility Maps. Magnetic Resonance Phase, Susceptibility, and Electrical Properties Mapping. 2022;
21. Roberts AG, Zhang J, Spincemaille P, Nguyen T, Wang Y. Choice of Architecture in 3D Super-Resolution of Quantitative Susceptibility Maps. presented at: International Society of Magnetic Resonance in Medicine; 2023; Toronto, Canada.
22. Bachrata BB, Steffen; Grabner, Günther; Trattnig, Siegfried; Robinson, Simon. Isotropic QSM in seconds using super-resolution 2D EPI imaging in 3 orthogonal planes. Magnetic Resonance in Medicine; 2022:
Figures