4704
Segmentation of Multiple Sclerosis lesions using 7T multi-contrast MRI data1High Filed MR Center, Department of Biomedical Imaging and Image-guided Therapy, Medical University of Vienna, Vienna, Austria, 2Department of Neurology, Medical University of Vienna, Vienna, Austria, 3Comprehensive Center for Clinical Neurosciences & Mental Health, Medical University of Vienna, Vienna, Austria, 4Department of Medical Engineering, Carinthia University of Applied Sciences, Klagenfurt, Austria
Synopsis
Keywords: Diagnosis/Prediction, Machine Learning/Artificial Intelligence
Motivation: The effective treatment of Multiple sclerosis (MS) requires reliable estimates of lesion load and hence precise lesion detection over time. However, current lesion load estimation is either qualitative or too time-consuming.
Goal(s): Our study automates MS lesion segmentation by training DeepMedic for application to 7T multi-contrast MRI data of MS patients.
Approach: Training with all four contrasts achieved the best results compared to Lesion Segmentation Tool (LST)—a conventional/non-deep-learning SPM-based MS lesions segmentation approach.
Results: Our study highlights potential for automating MS lesion detection/segmentation for 7T multi-contrast MRI data, underscoring the importance of accurate ground truth data and high-quality databases for improved detection accuracy.
Impact: The results of this research will impact the user-independent detection/segmentation of multiple sclerosis lesions, making manual assessment by clinicians obsolete and enable fully automated monitoring of lesions load as a quantitative radiological marker of disease progression.
Introduction
Multiple sclerosis (MS) requires early, precise lesion detection for effective treatment planning and prognosis. Manual segmentation is challenging due to small lesion sizes and time-consuming. Recent advancements in deep learning hold potential for automating lesion segmentation in various tasks[1,2]. Nonetheless, MS presents a continued challenge for segmentation accuracy, especially in clinical MRI (FLAIR/MPRAGE at 1.5T and 3T). Our study introduces automated lesion segmentation using 7T multi-contrast MRI data with the DeepMedic network, employing a combination of Binary Cross-Entropy (BCE) and Volume-level sensitivity–specificity (VSS) loss function[3,4].Methods
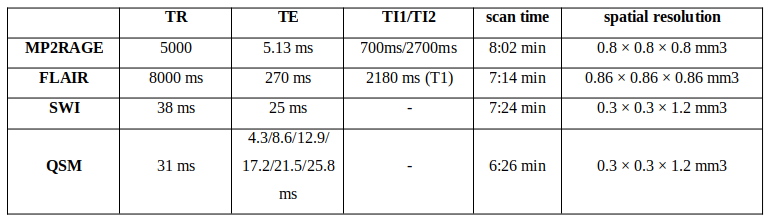
Experimental DataThe database contained multi-contrast 7 Tesla MRI data of 31 MS patients (age 42±15; 26 RRMS and 5 SPMS; EDSS 1,55±3.25). Four different MRI contrasts were measured for each subject: FLAIR, MP2RAGE, QSM, and SWI. Parameters of sequences and some pre-processing steps presented in Table 2.
Training and testing data
For training of the DeepMedic network, 23 subjects from the database were used, along with three subjects for validation. Five subjects were reserved for testing the performance of the neural network. Reference masks of lesions were manually segmented by an experienced neurologist (considered gold standard).
Neural network architecture
The network consists of two main components: a 3D convolutional neural network (CNN) for feature extraction and a fully connected conditional random field (CRF). To enhance the effectiveness of MS lesion detection, it was proposed to combine two loss functions, BCE and VSS [4]. This combination of loss functions allows to assess the performance of MS lesion detection not only at the voxel level but also assesses sensitivity and specificity of lesion detection at the volume level.
Network training
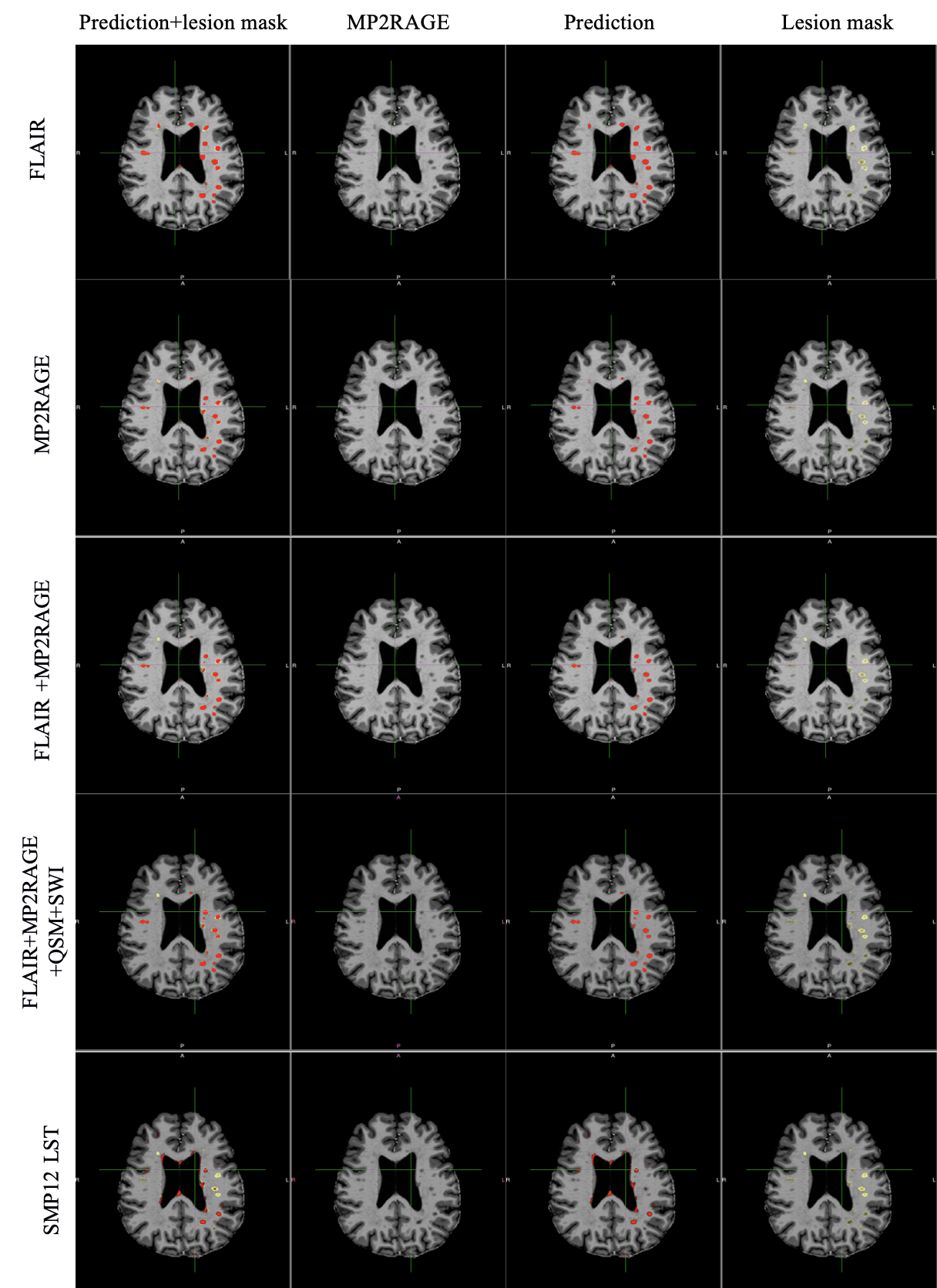
The network was trained using various combinations of contrasts. Initially, only one contrast, either FLAIR or MP2RAGE, was used. Subsequently, training was performed for two different combinations of contrasts: FLAIR+MP2RAGE and all four contrasts. Each training session involved 50 epochs, taking approximately 72 hours to complete. Training and network inference were conducted on an Nvidia DGX station using a single graphics card (Nvidia Tesla V100 32 GB). The network configurations used in our work were recommended by the authors of DeepMedic [3].
Evaluation
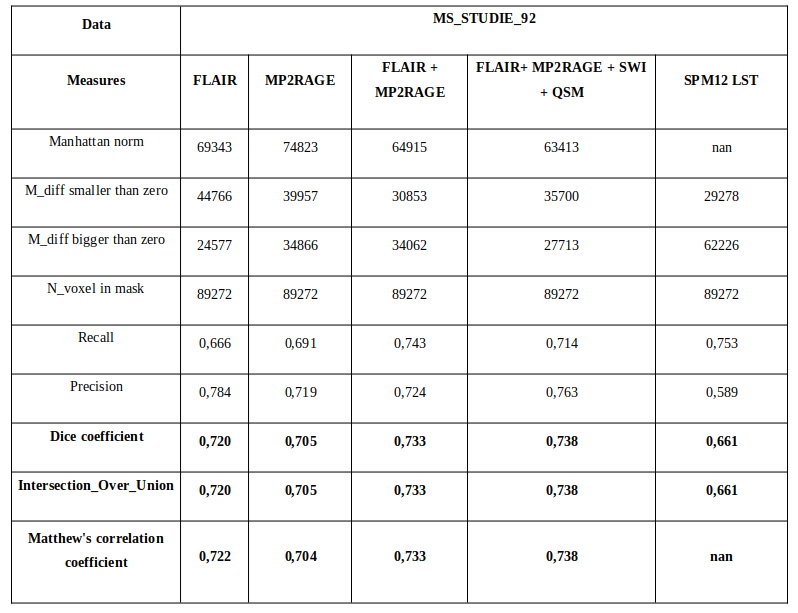
The prediction of lesion mask by different versions of network were evaluated alongside the segmentation with a conventional established approach—Lesion Segmentation Tool (LST) [5]—an extension of SPM12. LSM segmentation used only FLAIR images and did not involve MP2RAGE and others contrasts. To measure sensitivity and accuracy, assessments are made at the lesion level based on confusion matrix. To account for both location and size of segmentation, the Dice Similarity Coefficient (DSC) was used. Additionally, Intersection Over Union and Matthew's correlation coefficient were calculated.
Results
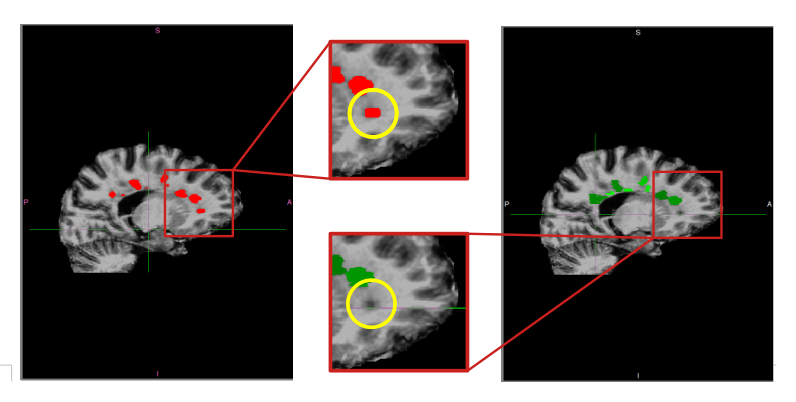
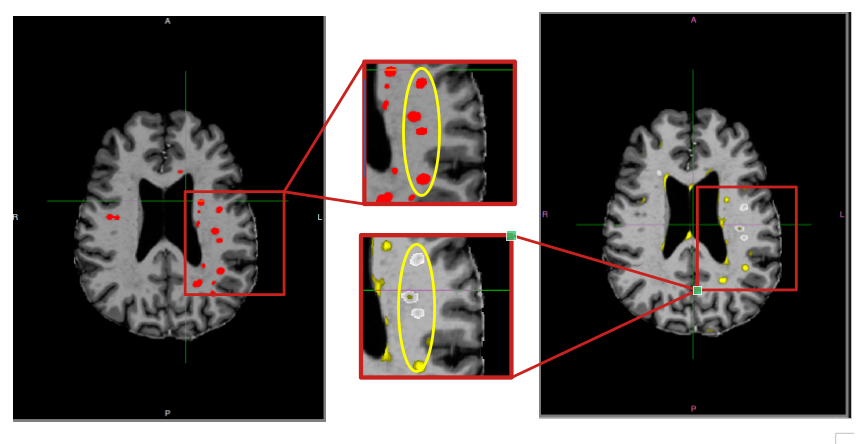
The assessment results after network training on various contrast combinations are presented in Table 1, along with the results from LST (results presented for one patient). Results after training using a single contrast show that FLAIR achieves slightly better lesion detection accuracy (DSC=0.720) than MP2RAGE (DSC=0.705). An example for false positives (FP) lesion segmentation after training with these two contrasts are shown in Figure 2. However, the network achieves better sensitivity and accuracy when trained with all four contrasts (DSC=0.738), as indicated in Table 1. In addition, a comparison was conducted between DeepMedic and SPM12 LST (Figure 1). The data obtained from this comparison indicates that accuracy of DeepMedic trained with FLAIR contrast (DSCmean=0.707) is higher than for SPM12 LST (DSCmean=0.659). A detailed comparison is provided in Table 2 (result presented for three patients). Deep learning lesion segmentation was not only more accurate, but also significantly faster (~3min per patient) than the manual segmentation performed by a clinician (4-5 hours per case).Discussion and Conclusion
In this study, we performed automated MS lesion segmentation using 7T multi-contrast MRI data with the DeepMedic network. We explored various training combinations, including single-contrast (FLAIR or MP2RAGE), dual-contrast (FLAIR and MP2RAGE), and all four contrasts. These combinations provide confidence in distinguishing true positive lesions, though expert assessment is still necessary. Our gold standard relied on a single experienced neurologist's segmentation, that make this limitation. Despite this, four-contrast 7T multi-contrast MRI data-based segmentation with DeepMedic produced excellent results.Additionally, we demonstrated the segmentation advantages of this neural network over SPM12 LST. Nevertheless, challenges in the gold standard contribute to less-than-perfect results, and an expanded dataset with more patients and expert manual segmentations is necessary. Employing two loss functions and high-quality databases can significantly enhance the accuracy of MS lesion detection and segmentation for clinical use.
Acknowledgements
No acknowledgement found.References
- Gros C., De Leener B, et al. Automatic segmentation of the spinal cord and intramedullary multiple sclerosis lesions with convolutional neural networks. Neuroimage. 2019 Jan 1;184:901-915. doi: 10.1016/j.neuroimage.2018.09.081. Epub 2018 Oct 6. PMID: 30300751; PMCID: PMC6759925.
- Zeng C, Gu L, Liu Z, Zhao S. Review of Deep Learning Approaches for the Segmentation of Multiple Sclerosis Lesions on Brain MRI. Front Neuroinform. 2020 Nov 20;14:610967. doi: 10.3389/fninf.2020.610967. PMID: 33328949; PMCID: PMC7714963.
- K. Kamnitsas, C. Ledig, et.al. Efficient multi-scale 3D CNN with fully connected CRF for accurate brain lesion segmentation. Medical Image Analysis,Volume 36, 2017, Pages 61-78, ISSN 1361-8415, https://doi.org/10.1016/j.media.2016.10.004.
- Huang Y, Bert C, et all. Deep learning for brain metastasis detection and segmentation in longitudinal MRI data. Med Phys. 2022 Sep;49(9):5773-5786. doi: 10.1002/mp.15863. Epub 2022 Jul 22. PMID: 35833351.
- Egger et al. (2017). MRI FLAIR lesion segmentation in multiple sclerosis: Does automated segmentation hold up with manual annotation? NeuroImage. Clinical, 13, 264–270. http://doi.org/10.1016/j.nicl.2016.11.020
Figures