4695
Deep Learning Reconstructed Reduced Field-of-View Diffusion Weighted Imaging in Rectal Cancer: Comparison of Image Quality1Radiology, West China Hospital of Sichuan University, Chengdu, China, 2GE Healthcare, MR Research, Beijing, China, Beijing, China
Synopsis
Keywords: AI/ML Image Reconstruction, Pelvis
Motivation: Reduced field-of-view DWI (rDWI) can improve the image quality (IQ) and lesion conspicuity in rectal cancer (RC) while reducing signal-to-noise ratio. Deep learning reconstruction (DLR) can denoise images. The feasibility and performance of DLR in rDWI for RC remains unclear.
Goal(s): To compare the IQ and apparent diffusion coefficient (ADC) values between DLR-rDWI and noDLR-rDWI in RC.
Approach: Objective and subjective IQ analysis were performed. ADC values were calculated. Results of IQ analysis and ADC between DLR-rDWI and noDLR-rDWI were compared.
Results: The IQ of DLR-rDWI was better than noDLR-rDWI (except lesion conspicuity, P=0.157). ADC values was not affected by DLR.
Impact: DLR-rDWI could be considered for inclusion in routine rectal MRI protocols. However, whether DLR can improve lesion conspicuity in RC should be further investigated with smaller lesions. The ability of DLR-rDWI in diagnosis and prediction for RC could be studied.
Introduction
As a non-enhanced magnetic resonance imaging (MRI) technique, diffusion weighted imaging (DWI) can detect the movement of water molecules and assess their diffusivity, providing valuable information about tissue cellularity and biophysical properties1,2, which is crucial for evaluating rectal tumor invasion, lymph node involvement, treatment response, and prognosis3–6. The reduced field-of-view DWI (rDWI) utilizes a 2D spatially selective echo planar radiofrequency pulse followed by a 180° refocusing pulse, has been successfully applied in various organs. This sequence decreases the number of k-space lines by reducing the field-of-view (FOV) in the phase encoding direction, resulting in high spatial resolution images while reducing off-resonance-related artifacts and blurring7. Studies have shown that rDWI had advantages over conventional DWI for rectal cancer in improvement of image quality and lesion conspicuity7,8. Nevertheless, higher spatial resolution brought by reducing FOV can lead to a reduced signal-to-noise ratio (SNR), which possibly degrades image quality (IQ) and influences the calculation of diffusion quantitative parameters, such as the apparent diffusion coefficient (ADC). Consequently, denoising rDWI images is necessary.One of the novel deep learning reconstruction (DLR) algorithms (AIRTM Recon DL [ARDL], GE Healthcare) shows the impressive ability to denoise images in various organs9–15. However, the feasibility and performance of applying ARDL to rDWI in rectal cancer remain unknown. The potential alteration of MRI information in rectal cancer presents a significant challenge for radiologists in achieving accurate diagnosis. Therefore, our study aims to compare the IQ and ADC values between DLR-rDWI and original rDWI (noDLR-rDWI) in the context of rectal cancer.
Methods
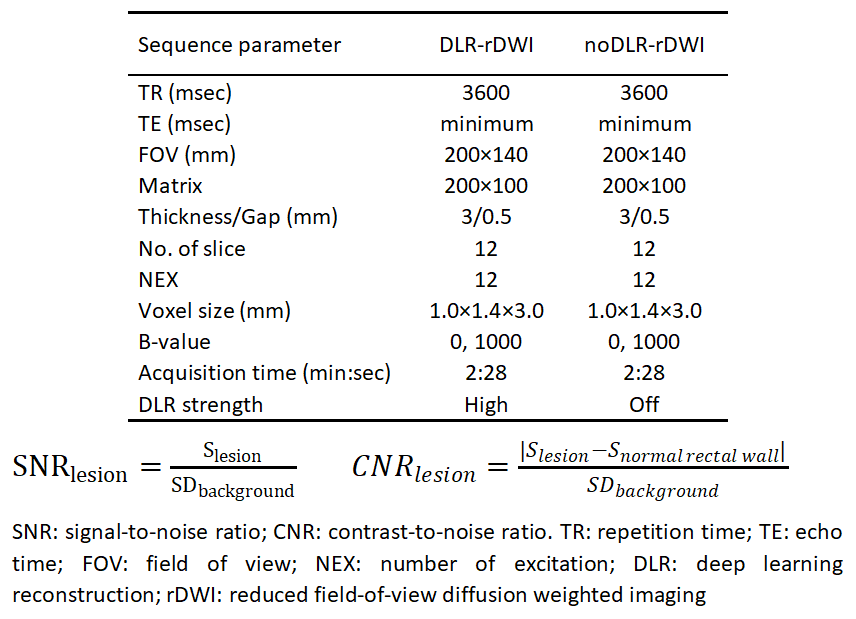
In this prospective study, 42 patients underwent rectal MRI with DLR-rDWI in a 3.0 T MRI scanner (SIGNA Premier, GE Healthcare) using a 30-channel AIRTM coil from September 2023 to October 2023. The inclusion criteria were as follows: histopathological results confirmed rectal carcinoma by biopsy and no previous treatment. Images with severe motion artifacts were excluded. The imaging parameters of rDWI are listed in Figure 1.In objective analysis, mean signal intensity (S) of normal rectal wall, lesions and the standard deviation (SD) of the background in both DLR-rDWI and noDLR-rDWI were measured twice to obtain average values by two radiologists who were blinded to both sequences. The SNR and contrast-to-noise ratio (CNR) of lesions in both sequences were calculated with the formulas10 in Figure 1.
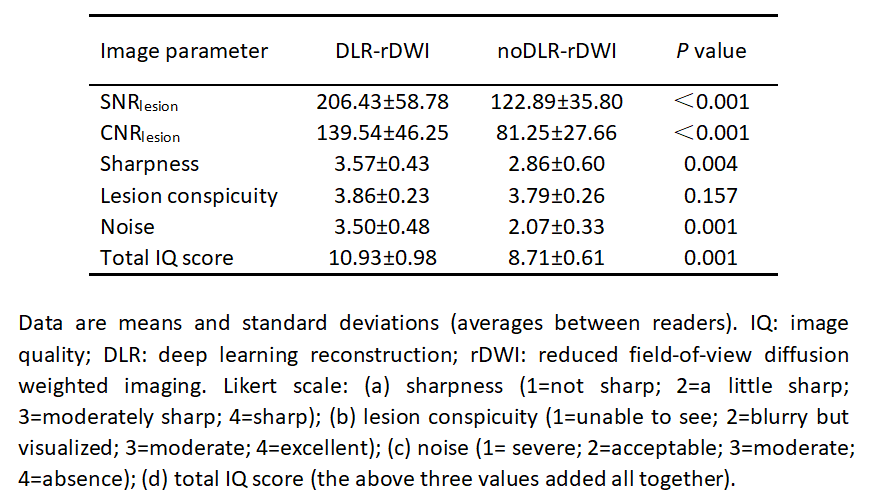
ADC values were measured on the normal rectal wall and the central slice of the tumor in two DWI sequences (b=1000 s/mm2), which was performed separately by two radiologists to obtain average ADC values. In subjective analysis, the aforementioned two radiologists performed assessments and scored two sets of DWI images using the axial high-resolution T2-weighted images as a reference. A Likert scale with scores ranging from 1 to 4 was used (Figure 2).
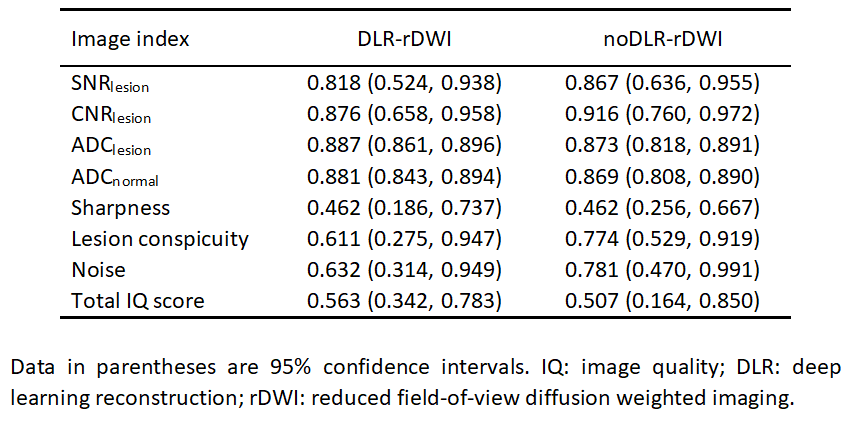
The interobserver variability for objective indexes (SNR, CNR and ADC) and subjective indexes was assessed using the intraclass correlation coefficient (ICC) and weighted kappa statistics, respectively. Differences in objective indexes (SNR, CNR and ADC) and subjective indexes between two DWI sequences were compared using the paired t-test and Wilcoxon signed rank test, respectively. A two-sided P value < 0.05 was considered statistically significant. All statistical analyses will be conducted using SPSS 26.0.
Results
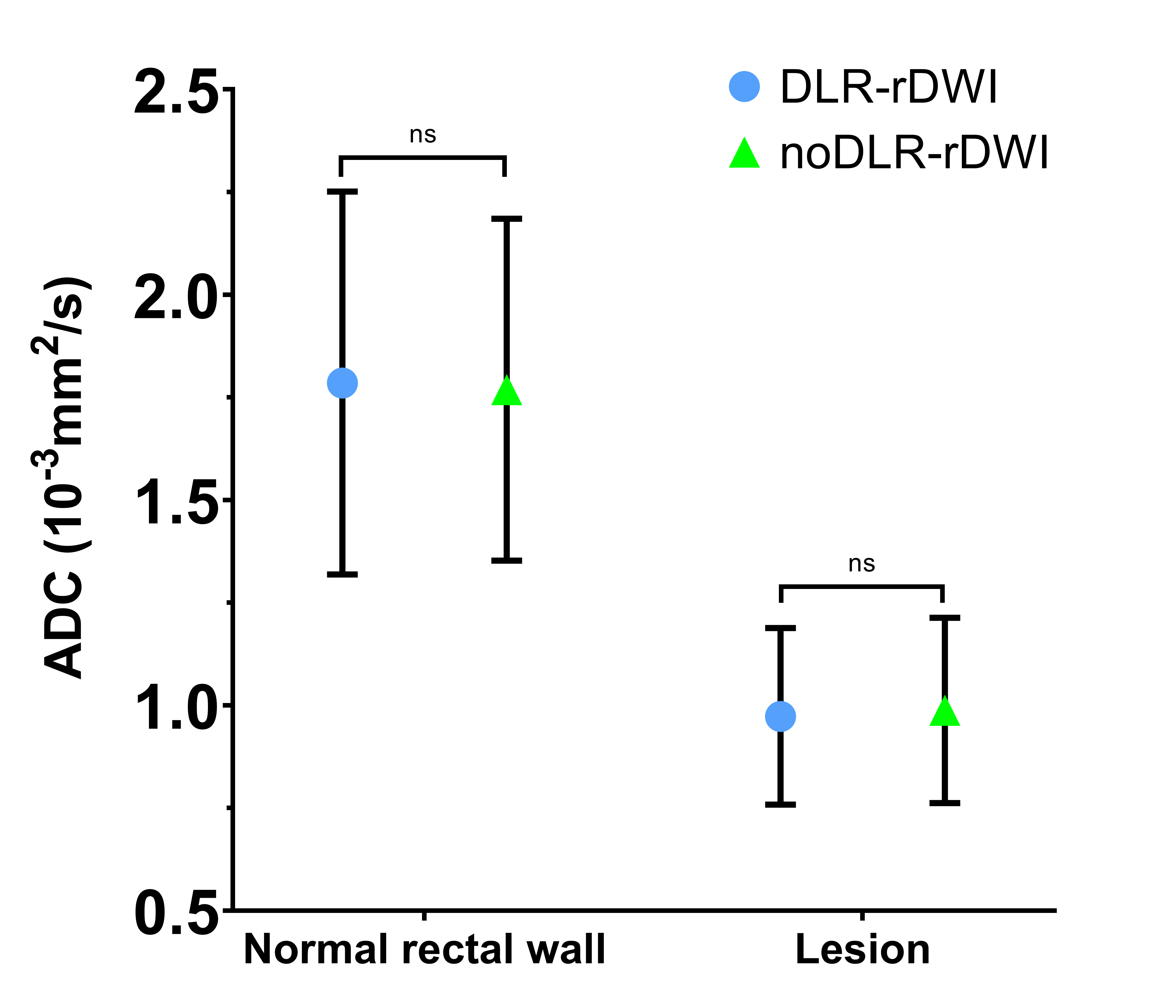
A total of 14 patients (8 men and 6 women, 55.9±6.6 years old) were included. The overall agreement of objective and subjective indexes was good (Figure 3). The SNRlesion and CNRlesion of DLR-rDWI were all higher than those of noDLR-rDWI (P<0.001). The scores of sharpness, noise and total IQ were higher for DLR-rDWI than noDLR- rDWI (P<0.01) (Figure 4). There was no significant difference in lesion conspicuity (P=0.157). Detailed results are listed in Figure 2. The ADC value of lesions was significantly lower than normal rectal wall in each DWI sequence (DLR-rDWI: 0.97±0.21 vs. 1.79±0.47, P<0.001; noDLR-rDWI: 0.99±0.23 vs. 1.77±0.42, P<0.001). There was no significant difference between two DWI sequences in ADCnormal rectal wall (P=0.517) or ADClesion (P=0.087) (Figure 5).Discussion
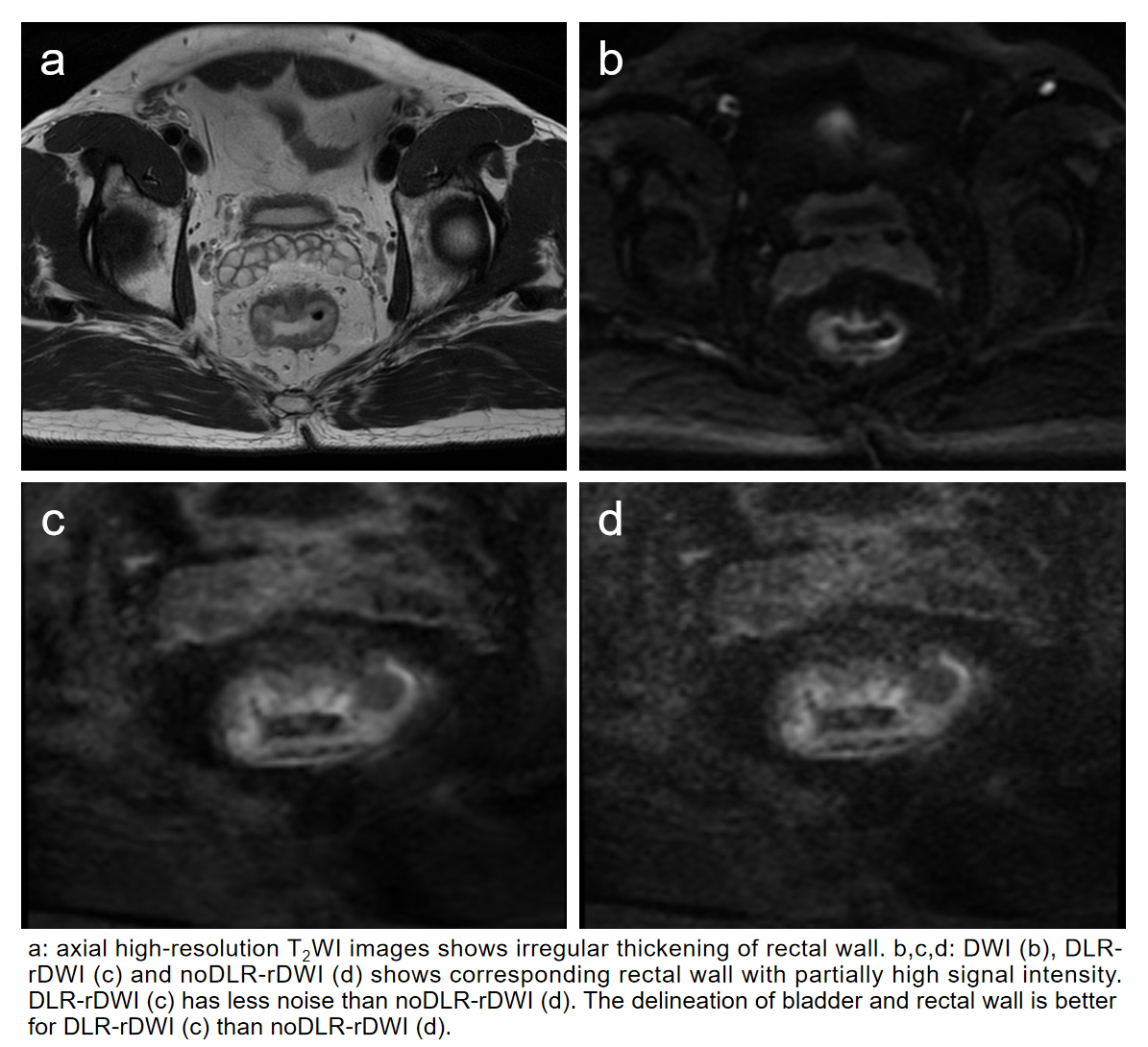
Our study demonstrated that ARDL could significantly reduce noise and improve IQ. Besides, the utilization of ARDL would not affect ADC measurements. However, no significant difference was found in lesion conspicuity, which could be attributed to the large lesion size of all the included patients.Conclusion
DLR-rDWI had better IQ compared to conventional rDWI and the utilization of ARDL had no impact on ADC measurement. Therefore, DLR-rDWI could be considered for inclusion in routine rectal MRI protocols.Acknowledgements
NoneReferences
1. Padhani AR, Liu G, Koh DM, et al. Diffusion-weighted magnetic resonance imaging as a cancer biomarker: consensus and recommendations. Neoplasia. 2009;11(2):102-125.
2. Lambregts DMJ, Rao SX, Sassen S, et al. MRI and Diffusion-weighted MRI Volumetry for Identification of Complete Tumor Responders After Preoperative Chemoradiotherapy in Patients With Rectal Cancer: A Bi-institutional Validation Study. Ann Surg. 2015;262(6):1034-1039.
3. Yang L, Qiu M, Xia C, et al. Value of High-Resolution DWI in Combination With Texture Analysis for the Evaluation of Tumor Response After Preoperative Chemoradiotherapy for Locally Advanced Rectal Cancer. AJR Am J Roentgenol. 2019;212(6):1279-1286.
4. Bonifacio C, Viganò L, Felisaz P, et al. Diffusion-weighted imaging and loco-regional N staging of patients with colorectal liver metastases. Eur J Surg Oncol. 2019;45(3):347-352.
5. Fusco R, Sansone M, Granata V, et al. Diffusion and perfusion MR parameters to assess preoperative short-course radiotherapy response in locally advanced rectal cancer: a comparative explorative study among Standardized Index of Shape by DCE-MRI, intravoxel incoherent motion- and diffusion kurtosis imaging-derived parameters. Abdom Radiol (NY). 2019;44(11):3683-3700.
6. Ahn JH, Kim SH, Son JH, Jo SJ. Added value of diffusion-weighted imaging for evaluation of extramural venous invasion in patients with primary rectal cancer. Br J Radiol. 2019;92(1096):20180821.
7. Peng Y, Li Z, Tang H, et al. Comparison of reduced field-of-view diffusion-weighted imaging (DWI) and conventional DWI techniques in the assessment of rectal carcinoma at 3.0T: Image quality and histological T staging. J Magn Reson Imaging. 2018;47(4):967-975.
8. Jang S, Lee JM, Yoon JH, Bae JS. Reduced field-of-view versus full field-of-view diffusion-weighted imaging for the evaluation of complete response to neoadjuvant chemoradiotherapy in patients with locally advanced rectal cancer. Abdom Radiol (NY). 2021;46(4):1468-1477.
9. Kim E, Cho HH, Cho SH, et al. Accelerated Synthetic MRI with Deep Learning–Based Reconstruction for Pediatric Neuroimaging. Am J Neuroradiol. Published online September 29, 2022:ajnr;ajnr.A7664v1.
10. Zerunian M, Pucciarelli F, Caruso D, et al. Artificial intelligence based image quality enhancement in liver MRI: a quantitative and qualitative evaluation. Radiol med. Published online September 7, 2022.
11. Kim SH, Choi YH, Lee JS, et al. Deep learning reconstruction in pediatric brain MRI: comparison of image quality with conventional T2-weighted MRI. Neuroradiology. 2023;65(1):207-214.
12. Ueda T, Ohno Y, Yamamoto K, et al. Deep Learning Reconstruction of Diffusion-weighted MRI Improves Image Quality for Prostatic Imaging. Radiology. 2022;303(2):373-381.
13. Muscogiuri G, Martini C, Gatti M, et al. Feasibility of late gadolinium enhancement (LGE) in ischemic cardiomyopathy using 2D-multisegment LGE combined with artificial intelligence reconstruction deep learning noise reduction algorithm. Int J Cardiol. 2021;343:164-170.
14. Hahn S, Yi J, Lee HJ, et al. Image Quality and Diagnostic Performance of Accelerated Shoulder MRI With Deep Learning–Based Reconstruction. Am J Roentgenol. 2022;218(3):506-516.
15. Kim M, Kim HS, Kim HJ, et al. Thin-Slice Pituitary MRI with Deep Learning–based Reconstruction: Diagnostic Performance in a Postoperative Setting. Radiology. 2021;298(1):114-122.
Figures