4691
Can Deep Learning Reconstruction Allow Rapid Diffusion Weighted Imaging for Rectal Cancer?1Department of Radiology, Second Affiliated Hospital of Naval Medical University, Shanghai, China, 2Department of Radiology, Frist Affiliated Hospital of Naval Medical University, Shanghai, China, 3MR Research, GE Healthcare, Beijing, China
Synopsis
Keywords: AI/ML Image Reconstruction, Diffusion/other diffusion imaging techniques
Motivation: Diffusion-weighted imaging (DWI) has been widely reported for detection, staging, and treatment response prediction of rectal cancer. High number of excitations for sufficient SNR was normally used in DWI for rectal cancer but with lengthy acquisition.
Goal(s): Investigate the role of deep learning reconstruction (DLR) in rapid rectum DWI by comparing with standard protocol.
Approach: Forty primary rectal cancer patients were enrolled. Each patient was imaged with standard and rapid DWI. Image quality and diagnostic performance were compared.
Results: Rapid DWI with DLR reduced 1/2 scan time without sacrificing image quality and improved the diagnostic performance for distinguishing T1/T2 from T1/T4 patients.
Impact: The application of DLR would be beneficial for rectum DWI not only for scan time but also for tumor boundary delineation being important for staging.
Introduction
According to the global cancer statistics in 2022, colorectum cancer was the third cause of cancer-related mortality in both male and female [1]. In clinic, rectal cancer patients are treated with surgery only or the combination of surgery and CRT depending on preoperative staging. MRI has been proven the most accurate non-invasive imaging modality for rectal cancer staging [2].Diffusion-weighted imaging (DWI), probing the microstructure of tissue by measuring the diffusion process of water molecules, has been validated for rectal cancer detection, staging and restaging, and treatment response prediction [2]. However, for high SNR, rectum DWI normally uses large number of excitations, prolonging the scanning time and thus increasing the motion sensitivity [3].
Recently, a deep learning reconstruction algorithm (DLR; AIRTM Recon DL, GE Healthcare) has become commercially available which can dramatically increase the SNR compared with conventional reconstruction (ConR) [4]. Previous studies have reported DLRecon can simultaneously reduce scan time and improve the image quality of DWI for prostate and liver [5-6]. With these promising results, this study aimed at investigating the feasibility of rapid rectum DWI with DLRecon for cancer staging.
Methods and Materials
PatientsForty primary rectal cancer patients were enrolled in this study.
MRI Acquisition
All MRI examinations were scanned at a 3.0T scanner (SIGNA Premier; GE Healthcare, CA, USA) with dedicated 21-channel AIRTM flexible coil (GE Healthcare). FOCUS MUSE DWI, alleviating the intestinal gas induced susceptibility distortions, was employed for rectal cancer measurement. For standard DWI protocol, the imaging parameters were as follow: TR/TE=4500ms/48ms, FOV=250mm×156mm, matrix size=160×96, slice thickness=3mm, number of slices=32, b values=0/1000 s/mm2, NEX=2/12. For the rapid DWI protocol, the scan parameters were identical except for halving NEX for both b values. The scan time of standard and rapid protocol was 2min15s and 1min8s, respectively. ConRecon was used to reconstruct standard DWI (sDWI_ConR), and the rapid DWI was reconstructed using ConRecon (rDWI_ConR) and DLR (rDWI_DLR), separately.
Image Analysis
Signal-to-noise ratio (SNR) and contrast-to-noise ratio (CNR) of lesion were used to assess the image quality. The SNR, CNR, and DWI derived apparent diffusion coefficient (ADC) of tumor were compared among sDWI_ConR, rDWI_ConR and rDWI_DLR, separately. T-staging was evaluated by two radiologists using the DWI images.
Statistical Analysis
Objective quantitative data were compared using paired non-parametric Friedman test. Post hoc test was further performed with Bonferroni correction for multiple comparisons. The accuracy, sensitivity, and specificity of T-staging were calculated using a confusion matrix. P<0.05 was considered significant.
Result
With pathological results, 18 patients were staged as T1 or T2 and the other 22 patients were confirmed to be T3 or T4 stage.As presented in Figure 1 and Table 1, the SNRs of rDWI_DLR and sDWI_ConR were similar and were significantly higher than that of rDWI_ConR (all P<0.05; Figure 1 and Table 1). The CNR of lesion was significantly higher for sDWI_ConR than rDWI_ConR. No significant difference of CNR was observed between rDWI_DLR and sDWI_ConR. The ADCs of lesion were comparable between rDWI_ConR and rDWI_DLR, but lower ADC of lesion was found in sDWI_ConR.
As shown in Figure 2, both T2WI and rDWI_DLR can accurately diagnose patients with T2 stage. However, the tumor boundary was blurred in sDWI_ConR and noisy in rDWI_ConR (Figure 2). Therefore, patients may be misdiagnosed as T3 stage.
As demonstrated in Figure 3, both T2WI and rDWI_DLR can clearly show the invasion of lesion into mesorectal fascia and uterus in patients with T4 stage. However, it’s difficult to diagnose patients as T4 stage based on sDWI_ConR and rDWI_ConR.
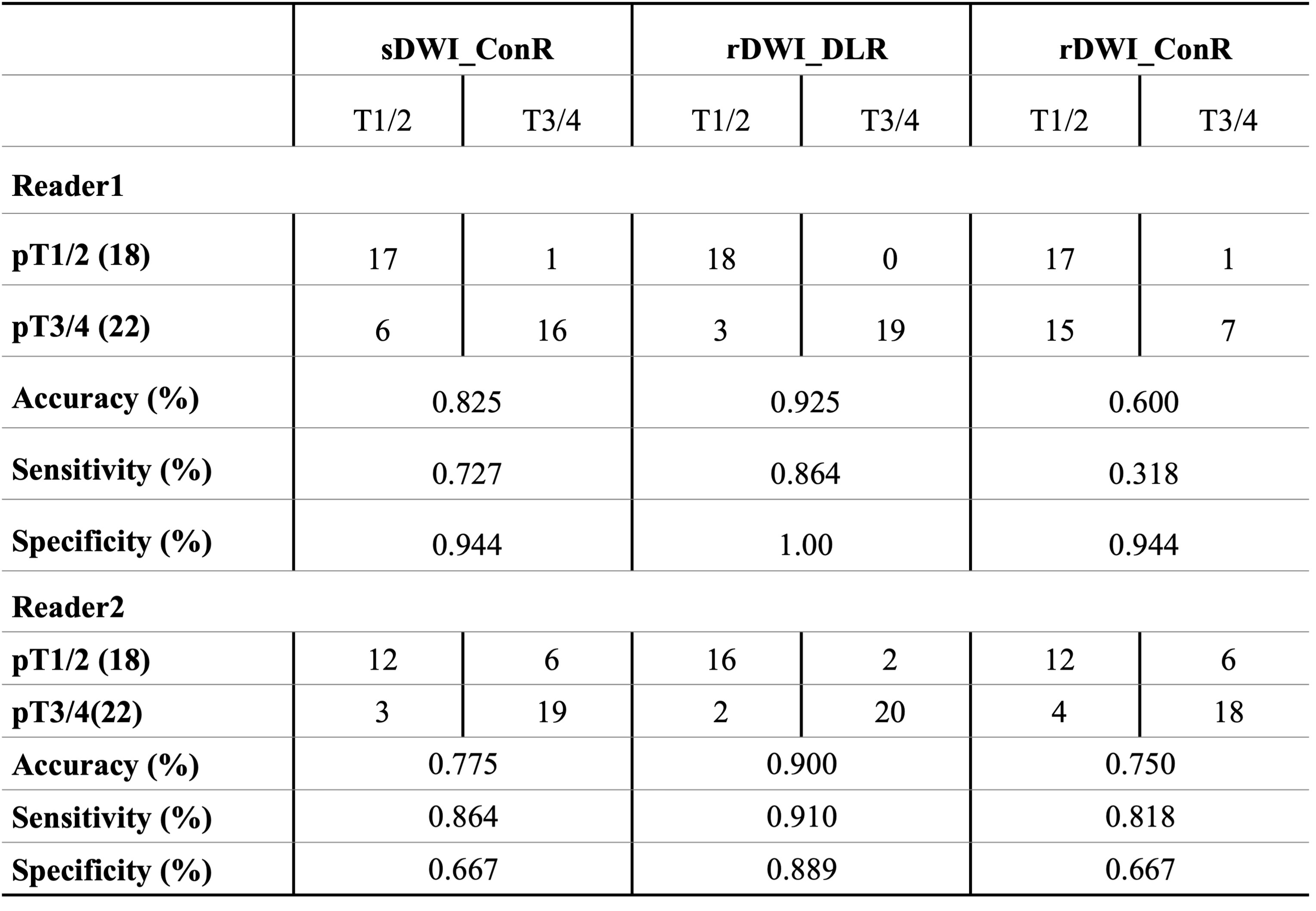
Table 2 showed rDWI_DLR can significantly improve the diagnostic accuracy of T1/T2 and T3/T4 stage in comparison with sDWI_ConR and rDWI_ConR.
Discussion and Conclusion
In this study, we investigated the role of DLR in rapid DWI of rectal cancer. Our results showed DLR enabled the reduction of scan time to 1/2 of standard protocol without sacrificing image quality. rDWI_DLR allowed for accurately depicting the boundary between tumor and adjacent structures, being essential for rectal cancer T-staging. This is possibly because the shortened scan time is prone to being less sensitive to intestinal peristalsis. As a result, rDWI_DLR improved the accuracy of primary rectal cancer T-staging.In conclusion, DLR would be beneficial for rectum DWI, not only for reducing scan time but also for differentiating T1/T2 from T3/T4 being essential for treatment selection.
Acknowledgements
No.References
[1] Bhupender S. Chhikara, Keykavous Parang. Global Cancer Statistics 2022: the trends projection analysis. Chem Biol Lett. 2023;10(1):451.
[2] Beets-Tan RGH, Lambregts DMJ, Maas M, et al. Magnetic Resonance Imaging for Clinical Management of Rectal Cancer: Updated Recommendations From the 2016 European Society of Gastrointestinal and Abdominal Radiology (Esgar) Consensus Meeting. Eur Radiol (2018) 28(4):1465–75.
[3] Yihan Xia, Lan Wang, Zhiyuan We, et al. Comparison of Computed and Acquired DWI in the Assessment of Rectal Cancer: Image Quality and Preoperative Staging. Front Oncol. 2022; 12:788731.
[4] Lebel RM. Performance characterization of a novel deep learning-based MR image reconstruction pipeline. arxiv.org/abs/2008.06559.
[5] Kang-Lung Lee, Dimitri A Kessler, Simon Dezonie, et al. Assessment of deep learning-based reconstruction on T2-weighted and diffusion-weighted prostate MRI image quality. Eur J Radiol. 2023; 166:111017.
[6] Marta Zerunian, Francesco Paucciarelli, Damiano Caruso, et al. Artificial intelligence-based image quality enhancement in liver MRI: a quantitative and qualitative evaluation. Radiol Med. 2022; 127(10):1098-1105.
Figures
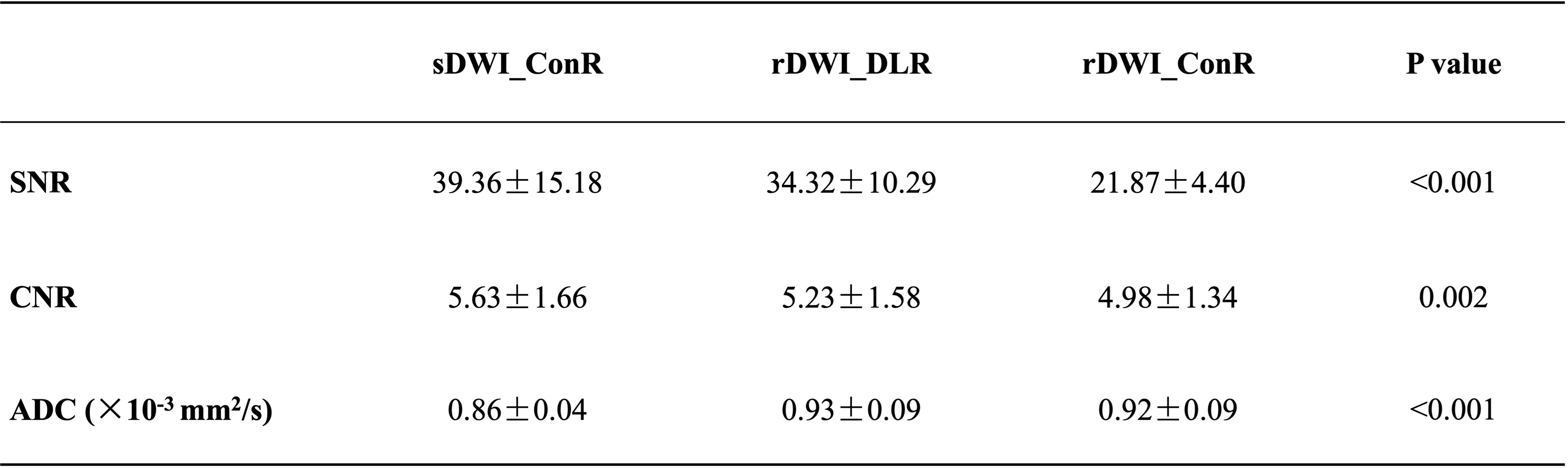
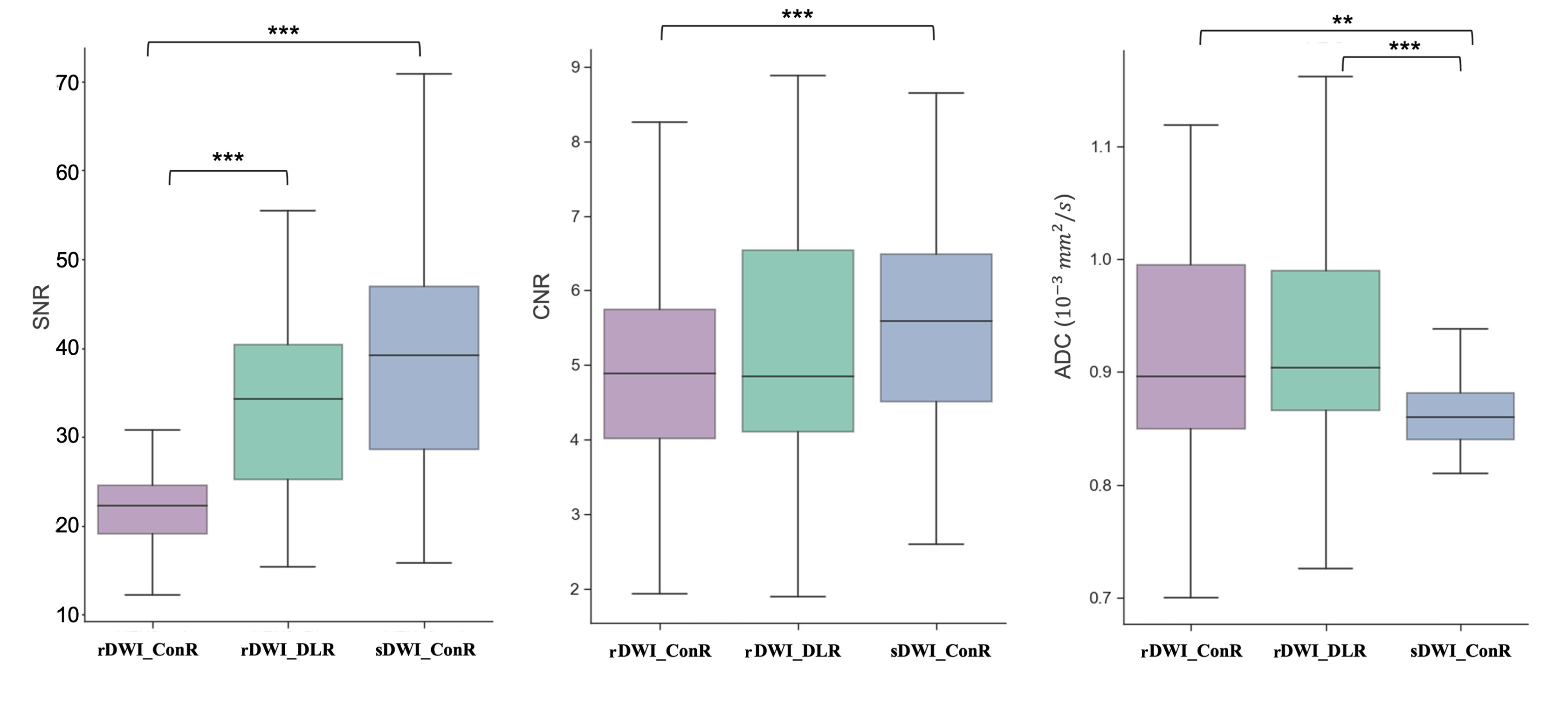
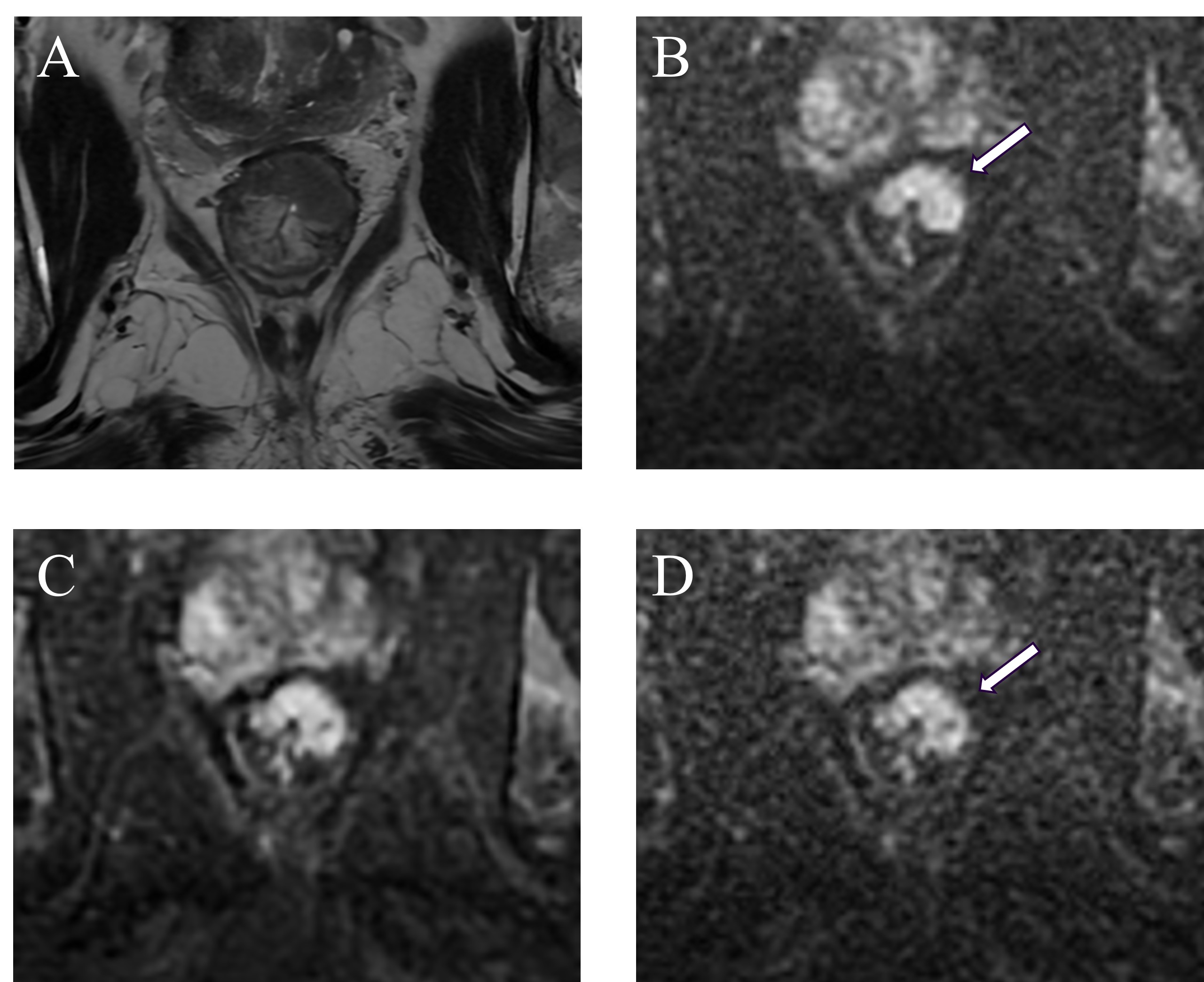
Figure 2. A 73 years old male staged as T2N0Mx according to pathological examination. A, High resolution T2-weighted image; B, sDWI_ConR; C, rDWI_DLR; D, rDWI_ConR. DWI, diffusion-weighted image; rDWI, rapid DWI; sDWI, standard DWI; ConR, conventional reconstruction; DLR, deep learning reconstruction.
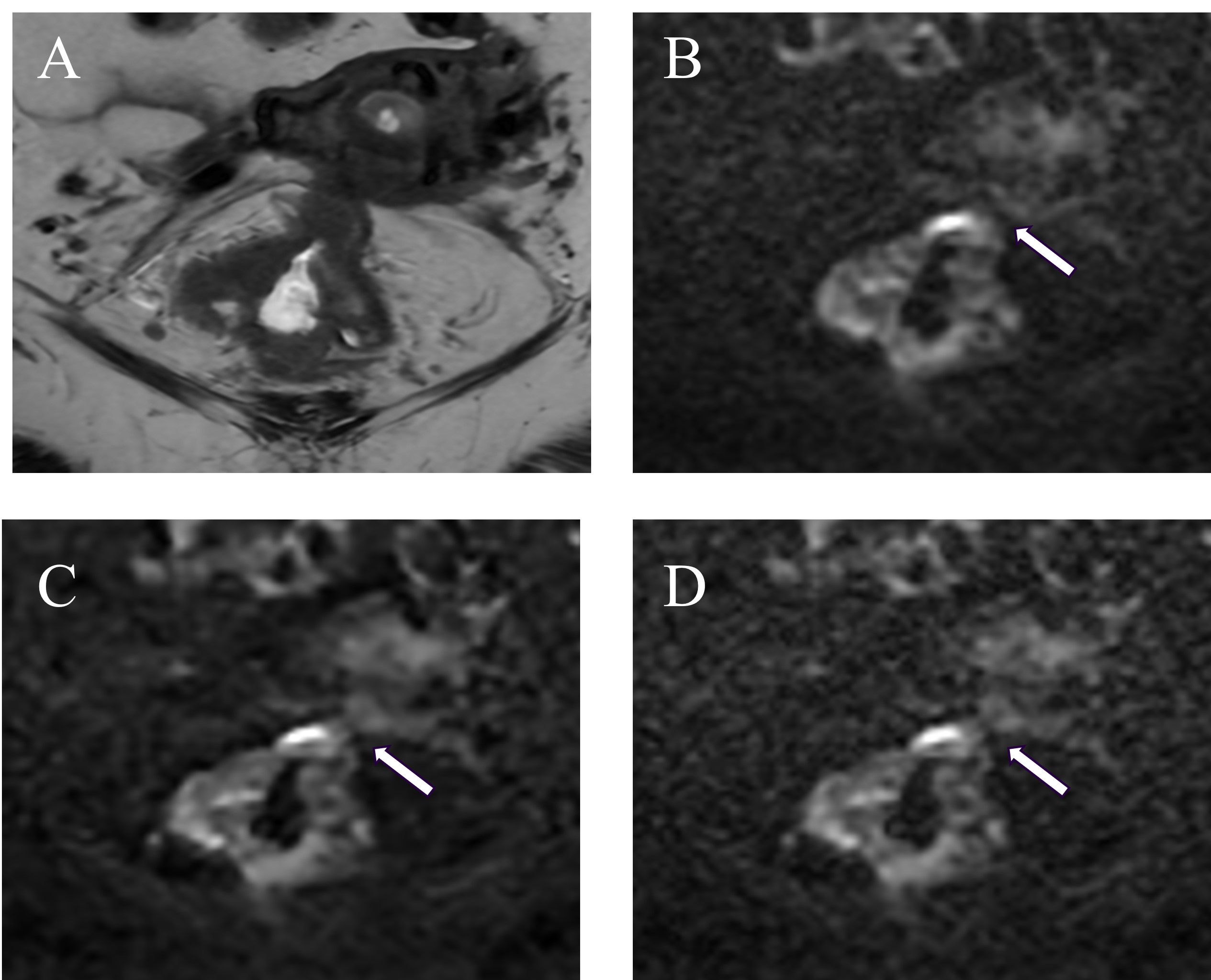
Figure 3. A 76 years old female staged as T4N2aMx according to pathological examination. A, High resolution T2-weighted image; B, sDWI_ConR; C, rDWI_DLR; D, rDWI_ConR. . DWI, diffusion-weighted image; rDWI, rapid DWI; sDWI, standard DWI; ConR, conventional reconstruction; DLR, deep learning reconstruction. The white arrows directed the interface between tumor and uterus