4690
Accelerating low-distortion diffusion MRI of the head and neck with transfer learning from a different organ, acquisition and scanner1Department of Medical Physics, Memorial Sloan Kettering Cancer Center, New York, NY, United States, 2Department of Radiology, Memorial Sloan Kettering Cancer Center, New York, NY, United States
Synopsis
Keywords: AI/ML Image Reconstruction, Machine Learning/Artificial Intelligence, Transfer learning, Head and neck
Motivation: Propeller and multi shot EPI sequences offer DWI head and neck images with reduced distortions, but suffer from longer scanning time and reduced SNR.
Goal(s): Shorten the scan time while improving SNR and without impacting ADC values.
Approach: Apply transfer learning to retrain denoising deep learning algorithm pretrained on different anatomy and vendor scanner, and using limited amount of data.
Results: Retraining has improved quantitative metrics, resulting in higher quality denoised images using a limited dataset of 5 cases.
Impact: Offsett extra time needed by distortion-reducing protocols to enhance the efficiency of MRI for cancer applications.
Introduction:
Single-shot echo planar imaging (EPI) is the standard readout for diffusion weighted imaging (DWI) acquisitions, but is prone to substantial geometric distortions in the head and neck [1]. Alternative strategies such as multi-shot EPI (msEPI) [2] and periodically rotated overlapping parallel lines with enhanced reconstruction (PROPELLER) [3] can significantly reduce distortions, but require substantially longer scan times than conventional EPI. One approach for offsetting this increase in scan time is to use deep learning image denoising to reduce the number of repetitions without decreasing SNR [4,5]. However, the network needs to be trained with significant amount of data for each anatomical site and acquisition technique. This study used a denoising convolutional neural network (dnCNN) to accelerate msEPI and PROPELLER DWI of the head and neck using a network that was previously trained on single-shot DWI data acquired on the pelvis and a different scanner, and updated the anatomy using transfer learning. The impact of dnCNN on SNR efficiency and apparent diffusion coefficient (ADC) accuracy was computed with and without transfer learning from a different organ, pulse sequences and vendor.Methods:
Healthy volunteers (N=10) and patients with oropharyngeal cancer (N=5) were scanned on a 3T scanner (Ingenia Elition, Philips Healthcare) using an IRB-approved study. 3-shot msEPI and PROPELLER DWI were acquired with 220x220mm field-of-view, 20 slices, 2x2x5mm voxels, and b=0, 200, 800s/mm2. The number of signal averages (NSA) acquired was 5 for msEPI (total scan time = 6:47), and 3 for PROPELLER (total scan time = 13:23). Parotid glands and gross tumor volumes (GTV, patients only) were segmented on each DWI scan using the b=0 reference scans (performed separately for msEPI and PROPELLER).Pre-trained network: A previously described 2D patch-based residual denoising CNN (dnCNN) was implemented. This model was previously trained to denoise noisy high b-value images based on matched high-SNR images and using a low b-value image for anatomical reference [4,5]. The initial training dataset consisted of single-shot EPI DWI data (b=0, 800s/mm2) from 109 rectal cancer patients who were scanned on 3T scanners (GE Healthcare), resulting in 749,744 training patches.
Network retraining: The dnCNN was re-trained for each sequence (msEPI/PROPELLER) and b-value (b=200/800 s/mm2) by freezing all the layers except the last 3 blocks and output layer. Data were divided into training (5 volunteers) and test sets (5 patients + 5 voluteers). Training data were preprocessed into patches as in pretraining and augmented using random transformations. Head and neck DWI (b=200 and 800 s/mm2) in the test set were denoised using both pretrained and retrained models. Denoising was performed separately for each repetition. ADC maps were generated from noisy, denoised, and averaged images using a monoexponential model.
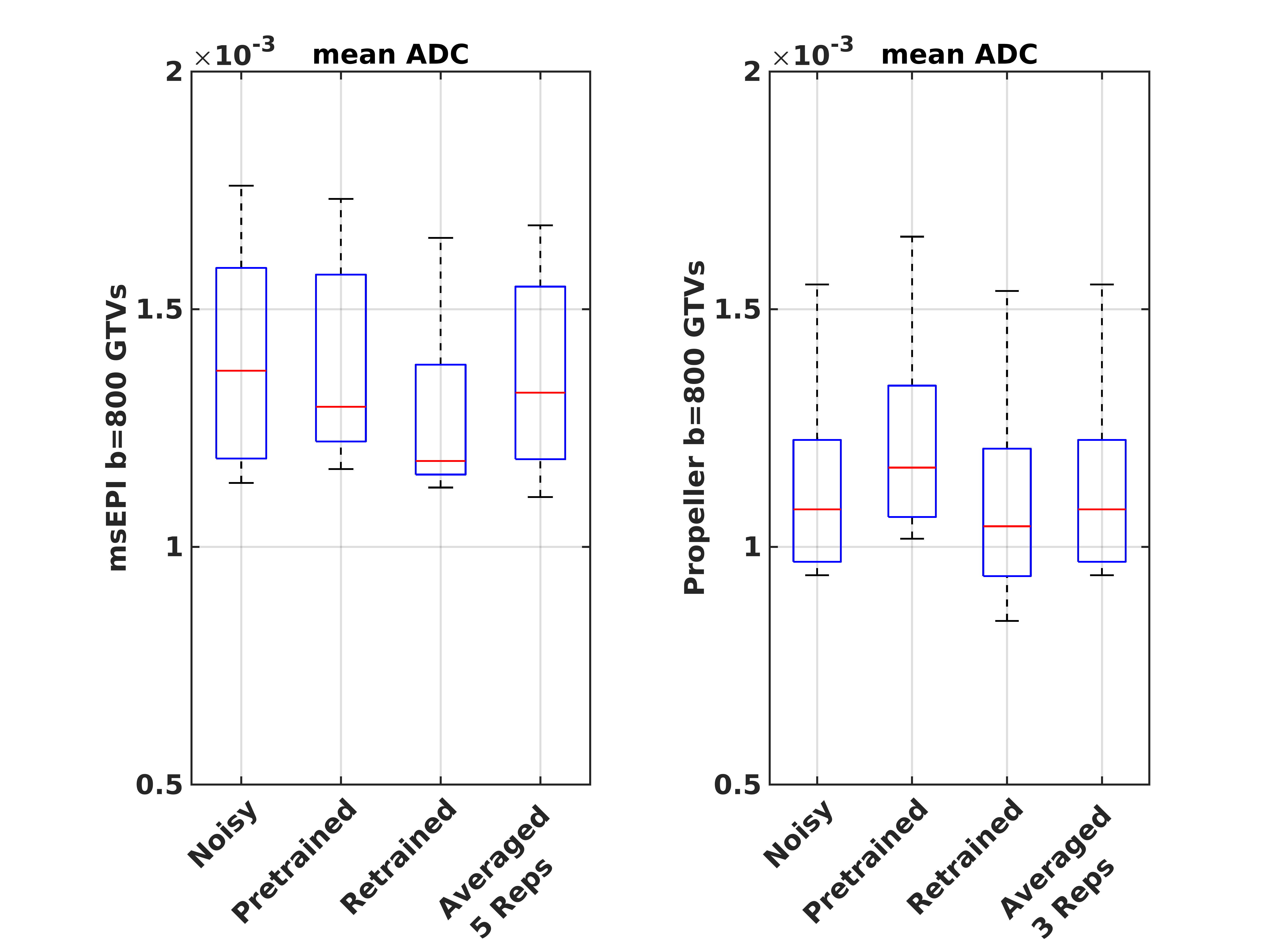
Analysis: SNR maps were generated for each acquisition by computing the mean and standard deviations (SD) across repetitions at each voxel (SNR=mean/SD). Mean SNR values were then computed within parotid gland delineations. ADC variability (ADC SD) maps were also generated by computing ADC maps from each repetition and computing the SD of the resulting ADC values at each voxel. SNR and ADC SD maps were generated for both raw and denoised data. SNR values were extrapolated to account for signal averaging (SNRAvg) by multiplying by $$$\sqrt{NSA}$$$ . Peak SNR (PSNR) and structural similarity index (SSIM) were calculated over entire 2D images [5] for each slice, subject, repetition, b-value, sequence, and denoising method. All parameters were compared between noisy, denoised, and averaged images using a paired t-test. Mean ADC values from each reconstruction were additionally correlated with the averaged maps (Pearson correlations) to test for systematic biases.
Results:
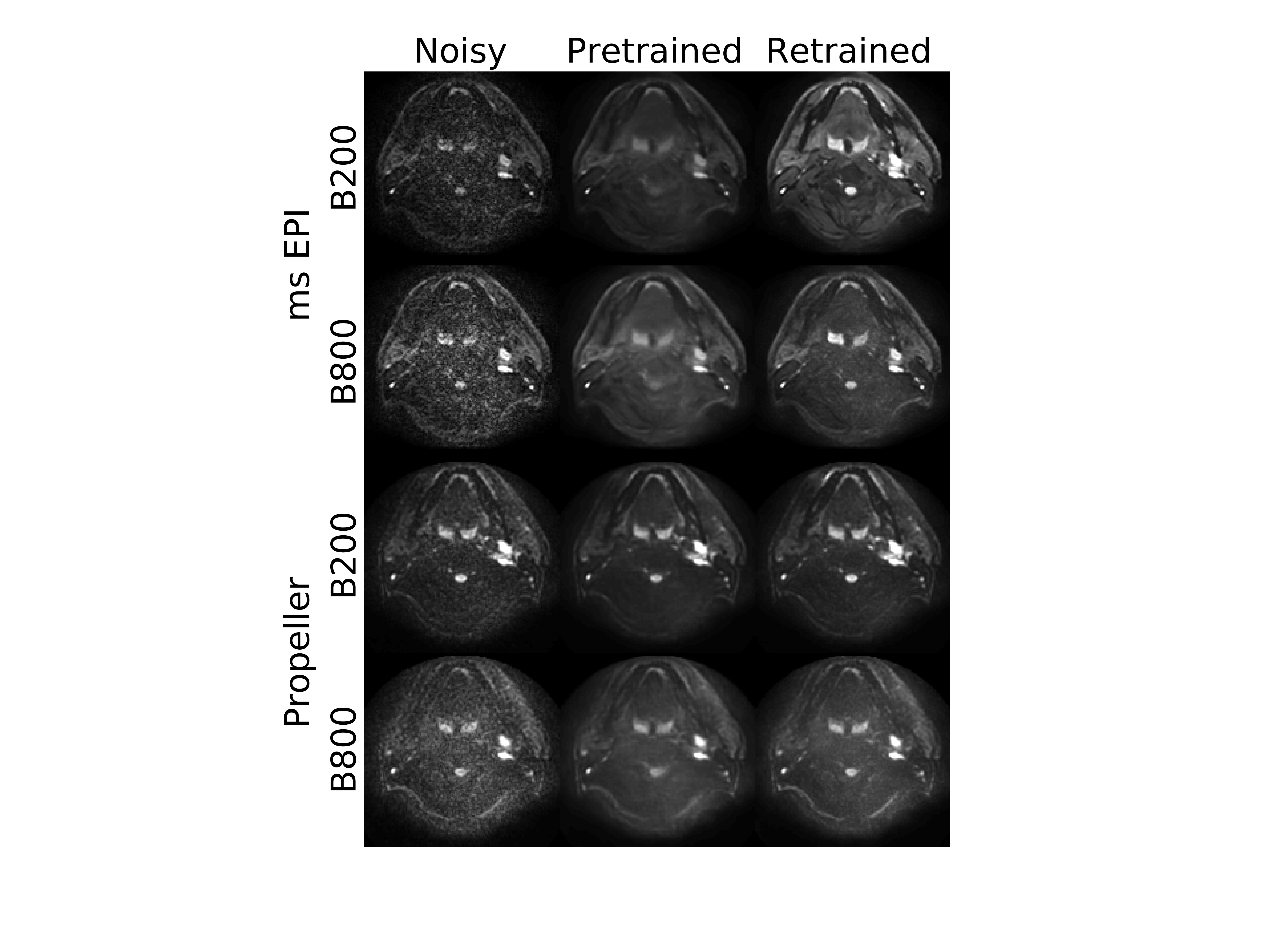
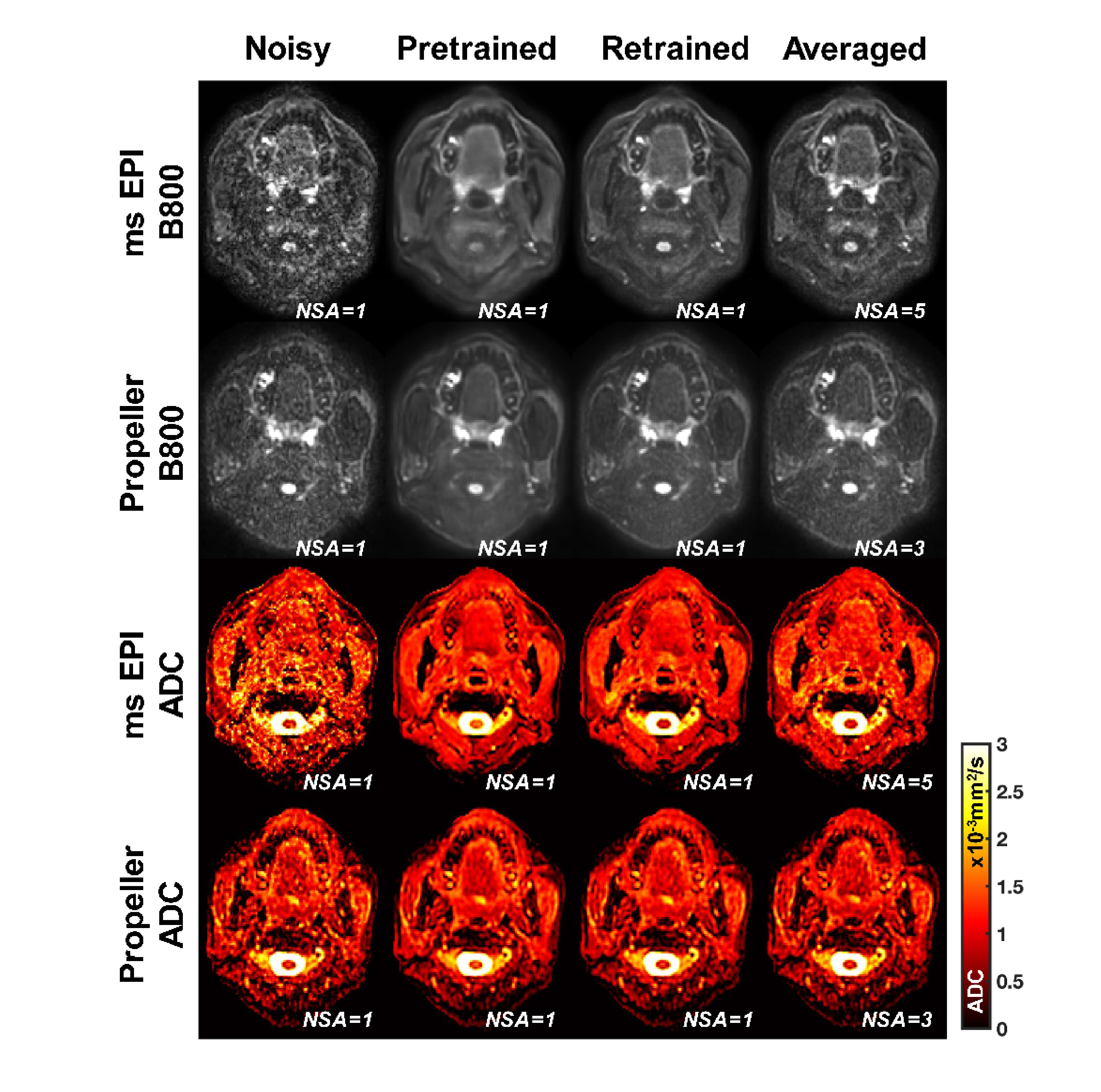
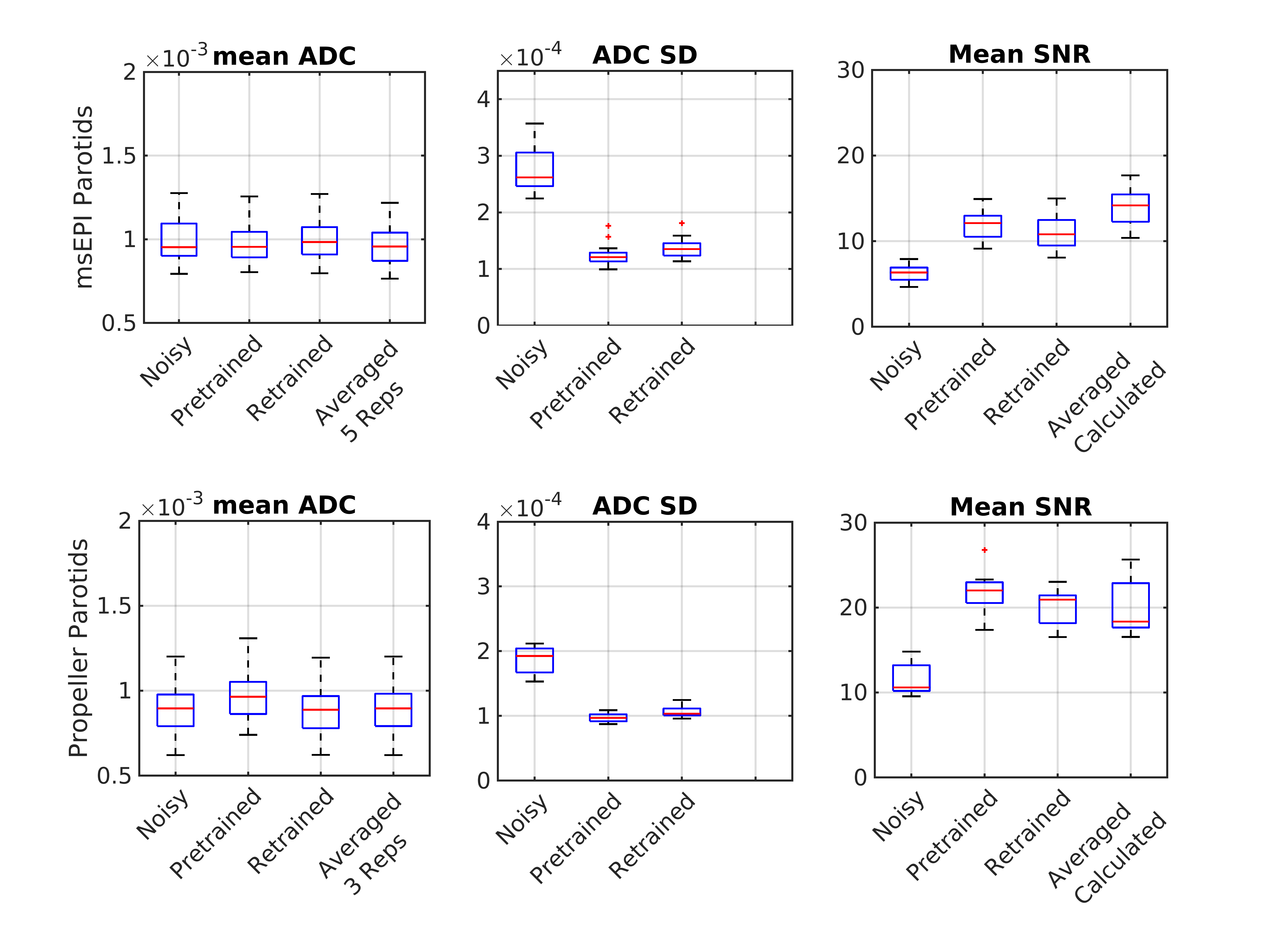
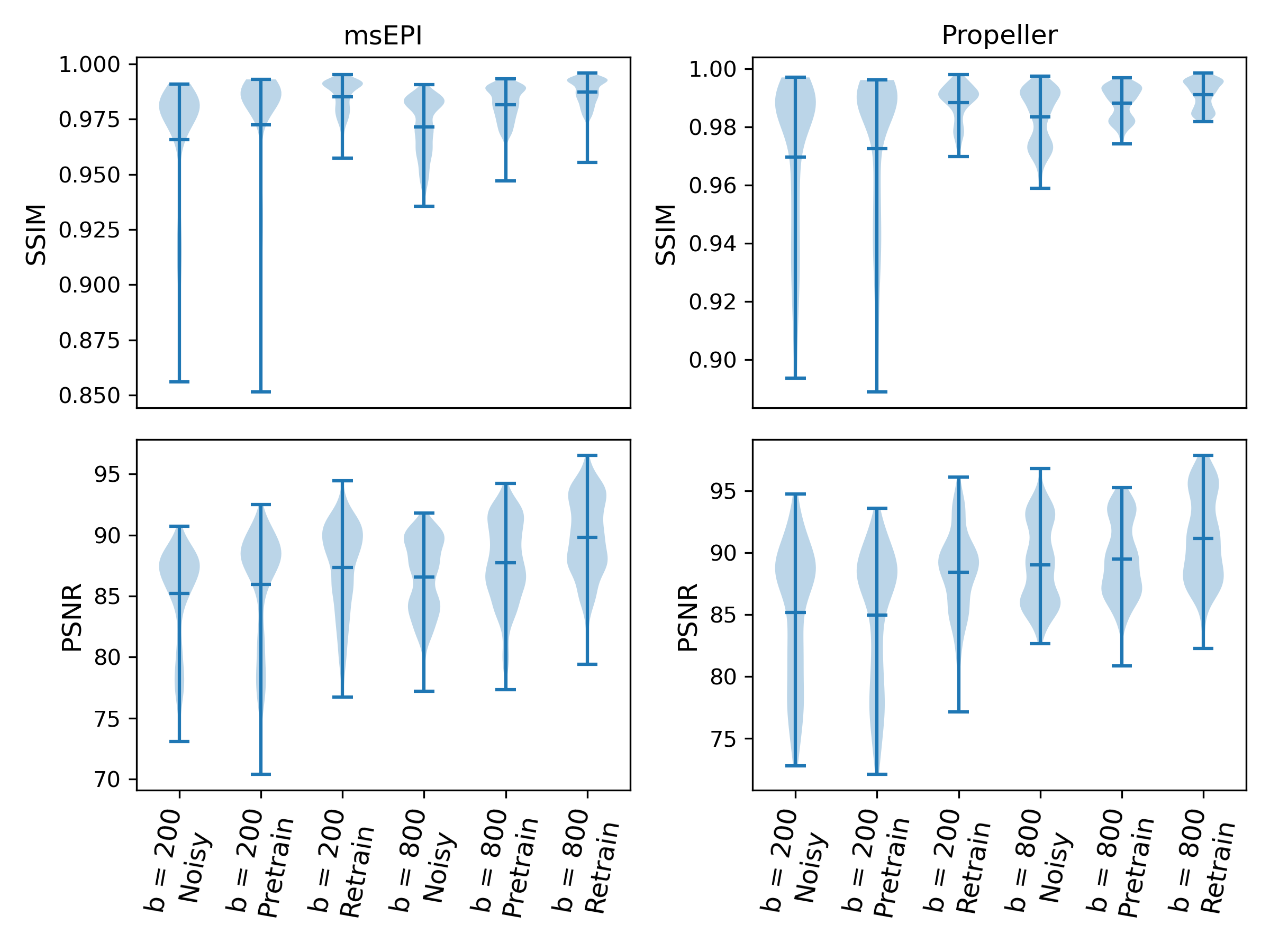
Retraining the network with transfer learning significantly reduced blurring from the results using the pre-trained network (Figures 1 and 2). Denoised SNR values were similar to what is achieved with signal averaging, $$$SNR_{avg}= SNR_{noisy}\times\sqrt{NSA}$$$ with the advantage of reducing scan time (Figure 3). Increased SNR (P<0.001, Figure 3), PSNR and SSIM (P<0.001, Figure 4), and decreased ADC SD (P<0.001) were observed for denoised vs. noisy DWI. The improvement in the retrained network was also observed in the SSIM values. While some differences in ADC values were observed between techniques (Figure 4, 5), all were strongly correlated with values reconstructed from averaged scans (R>0.9).Conclusions:
This work demonstrated the use of deep learning to improve efficiency of low-distortion diffusion MRI techniques and the application of transfer learning to efficiently adapt pre-trained networks to different anatomical sites, acquisition technique and scanner. The use of transfer learning limited the number of additional cases needed to only 5. This development can improve efficiency and quality of diffusion MRI for cancer applications.Acknowledgements
NIH grant R01‐CA244532.References
- Deng, J., Omary, R.A. and Larson, A.C., 2008. Multishot diffusion‐weighted SPLICE PROPELLER MRI of the abdomen. Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine, 59(5), pp.947-953.
- Porter, D.A. and Heidemann, R.M., 2009. High resolution diffusion‐weighted imaging using readout‐segmented echo‐planar imaging, parallel imaging and a two‐dimensional navigator‐based reacquisition. Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine, 62(2), pp.468-4753)
- Schakel, T., Hoogduin, J.M., Terhaard, C.H. and Philippens, M.E., 2013. Diffusion weighted MRI in head-and-neck cancer: geometrical accuracy. Radiotherapy and Oncology, 109(3), pp.394-397.
- Kaye, E.A., Aherne, E.A., Duzgol, C., Häggström, I., Kobler, E., Mazaheri, Y., Fung, M.M., Zhang, Z., Otazo, R., Vargas, H.A. and Akin, O., 2020. Accelerating prostate diffusion-weighted MRI using a guided denoising convolutional neural network: retrospective feasibility study. Radiology: Artificial Intelligence, 2(5).
- Mohammadi, M., Kaye, E.A., Alus, O., Kee, Y., Golia Pernicka, J.S., El Homsi, M., Petkovska, I. and Otazo, R., 2023. Accelerated Diffusion-Weighted MRI of Rectal Cancer Using a Residual Convolutional Network. Bioengineering, 10(3), p.359
Figures