4689
A novel neural network method predicts non-acquired brain diffusion MRI to promote HARDI in children1Neuroscience, University of Calgary, Calgary, AB, Canada, 2Software Engineering, University of Calgary, Calgary, AB, Canada, 3Radiology, University of Calgary, Calgary, AB, Canada, 4Clinical Neurosciences, University of Calgary, Calgary, AB, Canada
Synopsis
Keywords: AI/ML Image Reconstruction, Pediatric
Motivation: High angular resolution diffusion imaging has great potential but is time-consuming so is limited in pediatric clinical studies.
Goal(s): To assess the utility of novel deep learning techniques for predicting non-acquired brain diffusion MRI for equivalent HARDI analyses.
Approach: A multilayer perceptron (MLP) and convolutional neural network (CNN) were trained to predict b=2000s/mm2 data from b=750s/mm2 data. The neurite orientation dispersion and density index (NODDI) outcomes were computed with quality evaluated with PSNR and SSIM.
Results: Both deep learning methods achieved the goal but the CNN outperformed the MLP.
Impact: By applying a competitive neural network method, high angular resolution diffusion imaging can be made possible for the pediatric population in a typical clinical setting based only on half of the data typically required.
Introduction
High-angular resolution diffusion imaging (HARDI) can be a powerful tool for assessing tissue microstructural changes during brain development1,2. However, HARDI analyses typically require multi-shell acquisitions which are frequently hindered by limited scanning time and motion artifacts commonly seen in pediatric imaging. Recent developments demonstrate the possibility of addressing the time constrains in adults by predicting half of the data using deep learning methods3 but their utility in children is unclear. This study aims to implement similar approaches based on multilayer perceptron (MLP) and convolutional neural network (CNN) algorithms and assess how HARDI outcomes compare resulting from source versus predicted data in brain diffusion MRI of children.Methods
Full-brain diffusion-weighted MRI from >100 healthy children (2-8 years) were acquired. The parameters included b=750s/mm2 and/or b=2000s/mm2; each with 30 directions, 5 b0 interleaved. All parent/guardian consent and child assent were obtained. This study used 11 of the sample for algorithm development purposes. Image noises and artifacts were addressed during data preprocessing using Mrtrix3 and FSL software (Figure 1)4–9.Built on the published methods, the MLP and CNN were retrained using b=750s/mm2 instead of b=1000s/mm2 as input, and b=2000s/mm2 as output. Likewise, all experiments used a spherical harmonic representation (order of 8, 45 coefficients) with a voxel-wise approach in 3x3x3 volumetric patches derived from the input data3. Voxels from an individual were split at 70:15:15 percentages for training, validation and testing. Based on the original 30 directions, the diffusion orientation distribution function was calculated for the predicted output, and the function was employed to calculate the normalized mean squared error as the training loss10. The predicted and original data were combined into calculations of neurite orientation dispersion and density index (NODDI), where the orientation dispersion index (ODI) and neurite density index (NDI) were derived (Figure 2). Quality comparison of these indices between predicted and original acquisitions used 2 measures: peak signal-to-noise ratio (PSNR) and structural similarity index measure (SSIM), with p≤0.05 deemed significant.
Results
Based on training with one high-quality scan, both MLP and CNN were capable of predicting quality diffusion MRI as per qualitative and quantitative outcomes (Figure 3). The CNN-based NODDI indices outperformed the MLP-based (Figure 3). Further, CNN predictions based on training with different numbers of individuals showed a significantly better performance with 10 than other numbers, but between 1, 2, and 3 individuals, there was no clear trend in changing performance (Figure 4). Generally, ODI PSNR was higher than NDI PSNR while NDI SSIM was higher than ODI SSIM; the latter was the only measure suggesting a significant improvement in quality with training by more individuals than a single one (Figure 4). When the CNN was further applied to make prediction for 5 individuals, PSNR was still higher in ODI (26.55) than NDI (22.57) and SSIM higher in NDI (0.95) than ODI (0.93), although the relative quality of predictions between individuals appeared similar (Figure 5).Discussion
Both deep learning models here showed a great capacity to predict high b-value brain diffusion MRI data in a pediatric cohort as evidenced by NODDI PSNR and SSIM, consistent with previous findings in adults (PSNR=25; SSIM=0.97)3,11,12. In this research field, voxel-based training using a single subject is not uncommon, in contrast to other deep learning tasks requiring considerably large sample size. In experiments comparing the number of subjects used in training, there appeared a slight benefit by including multiple individuals. However, this result did not seem to be consistent because no significant differences were found between 1 and 10 individuals for most performance measures. It is worth noting that the individuals used in model training may have an impact on the quality measures. A greater variance in the training set resulting from inclusion of more individuals may improve performance, but the results could be strongly influenced by the consistency of input quality. Between models, the CNN outperformed the MLP suggesting that local spatial patterns from CNN may improve model performance, deserving further consideration in future model designs. Collectively, our findings suggest that populations who routinely experience scanning difficulties may benefit from deep learning algorithms to recover the power of advanced imaging without compromising scanning times. Future work seeks to explore large-scale predictions for children without multiple b-value data acquired and assess how HARDI-based measures evolve with brain development.Conclusion
Deep learning methods can help improve access to quality HARDI analysis by overcoming limitations in pediatric imaging. The developed CNN model can predict high b-value diffusion data with promising accuracy and may therefore promote HARDI applications in pediatric populations.Acknowledgements
We thank the graduate studentship funding support from the Alberta Graduate Education Scholarship. We also thank the funding support from the Natural Sciences and Engineering Council of Canada (NSERC), Canadian Institutes of Health Research (CIHR) and Alberta Innovates Health Solutions for this project.
References
1. Mah, A., Geeraert, B. & Lebel, C. Detailing neuroanatomical development in late childhood and early adolescence using NODDI. PLOS ONE 12, e0182340 (2017).
2. Lebel, C. & Deoni, S. The development of brain white matter microstructure. NeuroImage 182, 207–218 (2018).
3. Murray, C. et al. Neural network algorithms predict new diffusion MRI data for multi-compartmental analysis of brain microstructure in a clinical setting. Magnetic Resonance Imaging (2023) doi:10.1016/j.mri.2023.03.023.
4. Andersson, J. L. R. & Sotiropoulos, S. N. An integrated approach to correction for off-resonance effects and subject movement in diffusion MR imaging. NeuroImage 125, 1063–1078 (2016).
5. Andersson, J. L. R., Graham, M. S., Zsoldos, E. & Sotiropoulos, S. N. Incorporating outlier detection and replacement into a non-parametric framework for movement and distortion correction of diffusion MR images. NeuroImage 141, 556–572 (2016).
6. Andersson, J. L. R. et al. Towards a comprehensive framework for movement and distortion correction of diffusion MR images: Within volume movement. NeuroImage 152, 450–466 (2017).
7. Andersson, J. L. R., Graham, M. S., Drobnjak, I., Zhang, H. & Campbell, J. Susceptibility-induced distortion that varies due to motion: Correction in diffusion MR without acquiring additional data. NeuroImage 171, 277–295 (2018).
8. Kellner, E., Dhital, B., Kiselev, V. G. & Reisert, M. Gibbs-ringing artifact removal based on local subvoxel-shifts. Magnetic Resonance in Medicine 76, 1574–1581 (2016).
9. Tustison, N. J., Avants, B. B., Cook, P. A. & Gee, J. C. N4ITK: Improved N3 bias correction with robust B-spline approximation. in 2010 IEEE International Symposium on Biomedical Imaging: From Nano to Macro vol. 29 708–711 (IEEE, 2010).
10. Descoteaux, M., Angelino, E., Fitzgibbons, S. & Deriche, R. Regularized, fast, and robust analytical Q-ball imaging. Magnetic Resonance in Medicine 58, 497–510 (2007).
11. Chen, G., Hong, Y., Huynh, K. M. & Yap, P.-T. Deep learning prediction of diffusion MRI data with microstructure-sensitive loss functions. Medical Image Analysis 85, 102742 (2023).
12. Gibbons, E. K. et al. Simultaneous NODDI and GFA parameter map generation from subsampled q-space imaging using deep learning. Magnetic Resonance in Medicine 81, 2399–2411 (2019).Figures
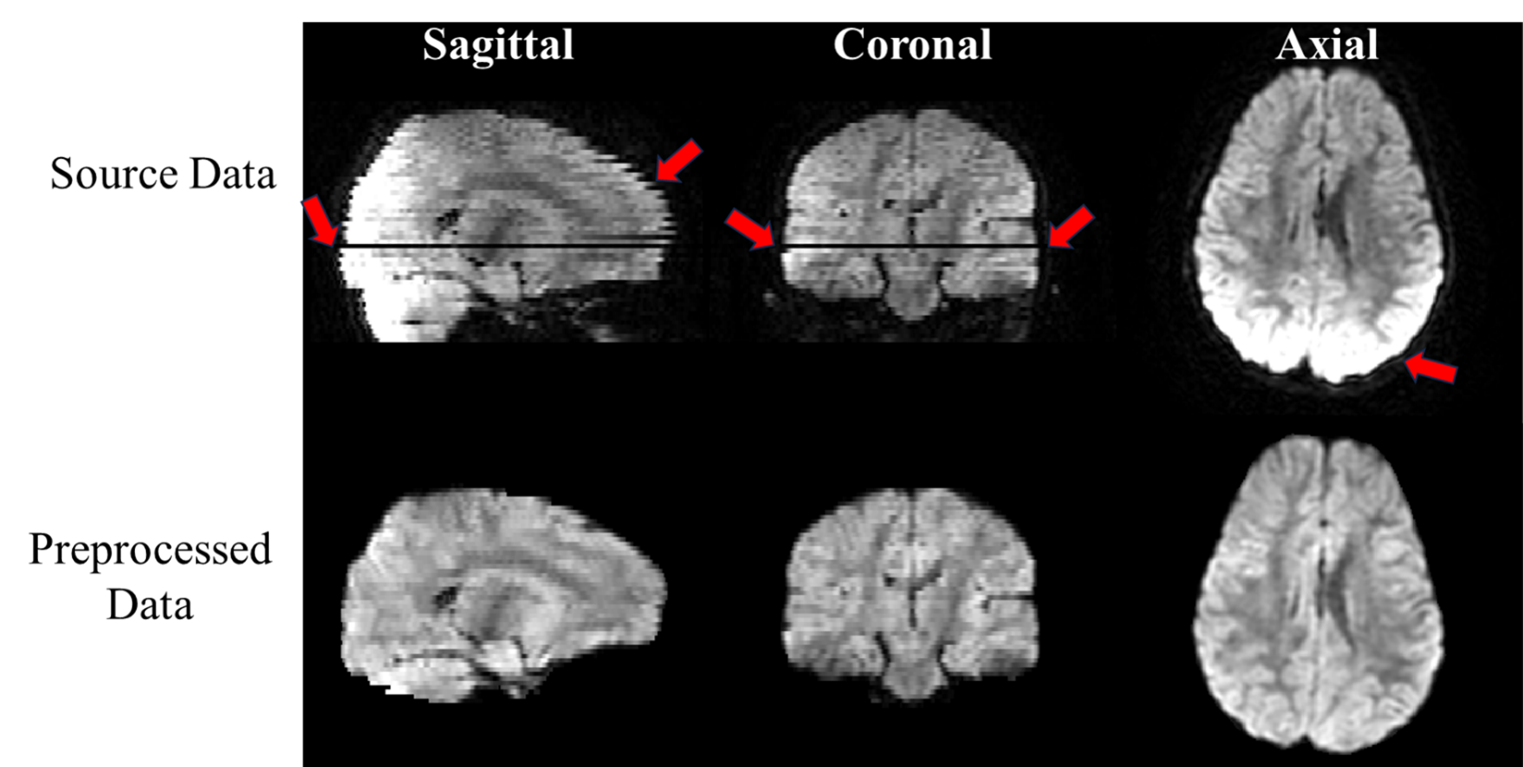
Figure 1: Examples of pediatric brain diffusion MRI with and without preprocessing. Original diffusion acquisitions (top) show the clear impact of motion on imaging sequences with the visibility of zig-zag artifacts. Following diffusion preprocessing (bottom), motion-based zig-zag artifacts are largely corrected.
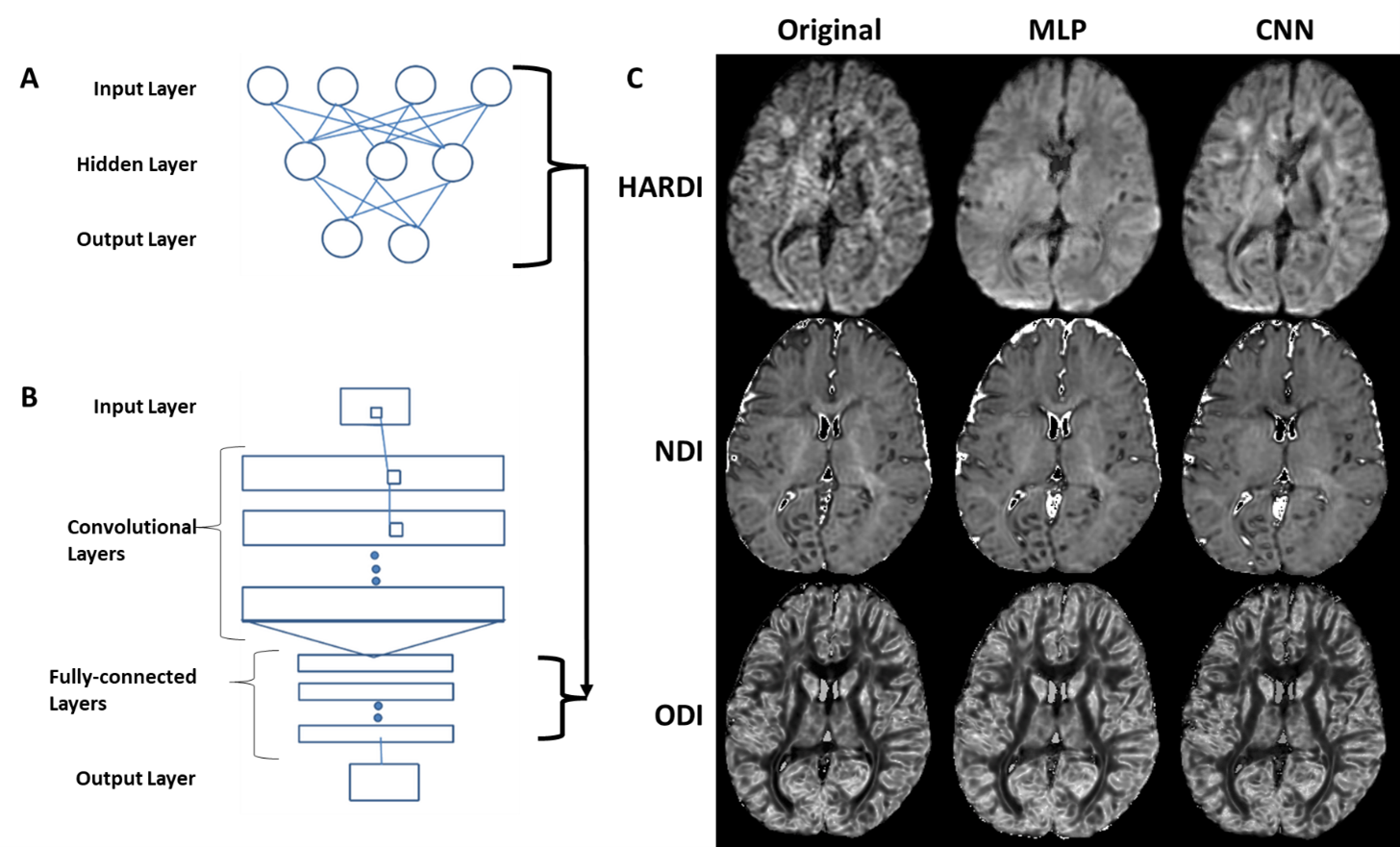
Figure 2: Model comparison between a multilayer perceptron (MLP) and convolutional neural network (CNN). Illustration of model architectures including a MLP (A) and a CNN (B) taking in diffusion MRI data in a spherical harmonic format from 3x3x3 patches. The same MLP architecture forms the basis of the fully connected layers of the CNN. A comparison of the HARDI NDI and ODI outcomes modelled from both the source (low b-value) and predicted (high b-value) diffusion data are shown (C).
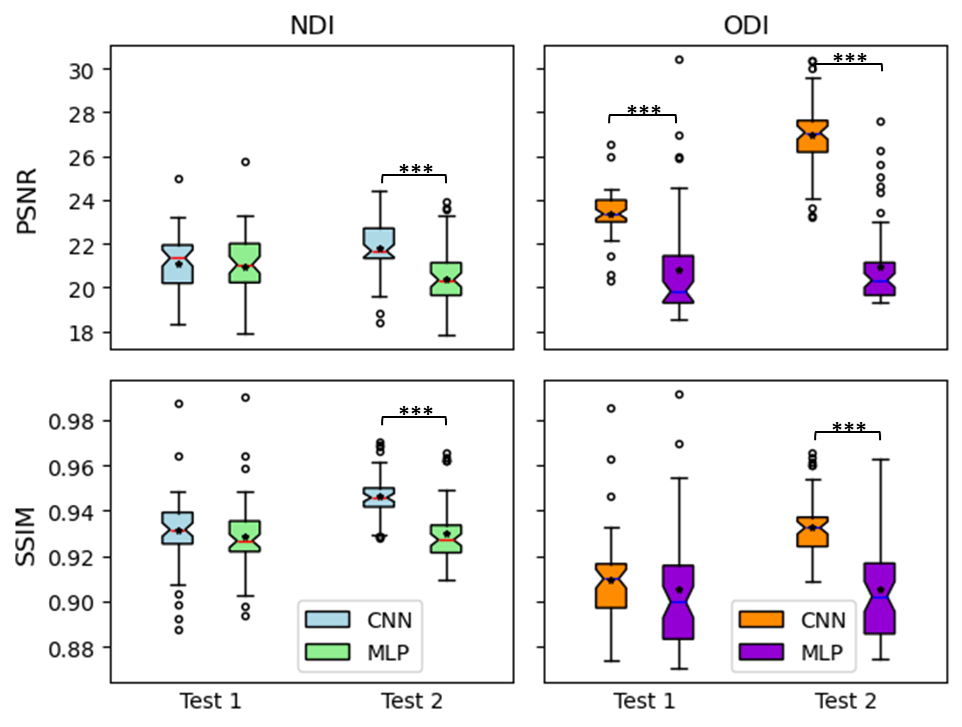
Figure 3. Quantitative comparison of NODDI outcomes based on diffusion MRI predictions from different deep learning architectures. A multilayer perceptron (MLP) and convolutional neural network (CNN) were trained on a single individuall and then used to predict another one (Test 1), while the experiments were repeated by flipping the training and prediction individuals (Test 2). Note: * for p < 0.05; ** for p < 0.01; and *** for p < 0.001.
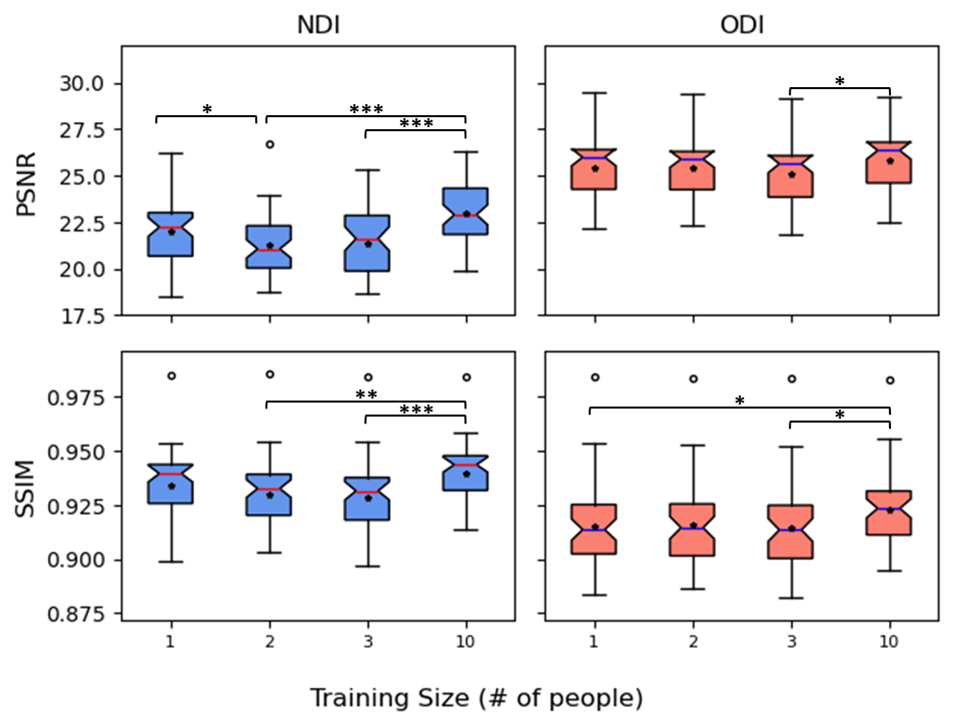
Figure 4: Quantitative comparison of NODDI outcomes based on models trained with different numbers of individuals. The results are computed using the original low b-value and predicted high b-value diffusion data. Note: * for p < 0.05; ** for p < 0.01; and *** for p < 0.001.
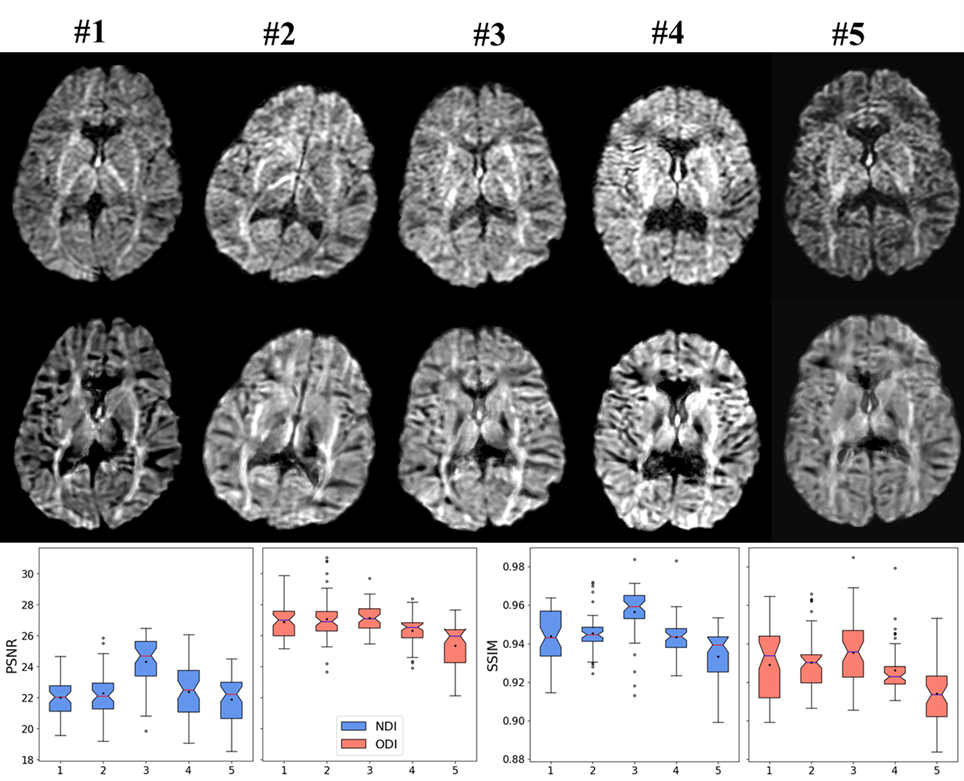
Figure 5: Prediction outcomes using CNN model trained with 1 patient input. The images show high b-value source (top) and predicted (bottom) diffusion MRI for 5 subjects. Quantitative comparison of NODDI outcomes computed using predicted data showing PSNR (bottom left) and SSIM (bottom right) for NDI (blue) and ODI (red).