4668
Deep Learning Reconstruction algorithm for T2-weighted Turbo Spin Echo Renal MRI1Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China, 2MR Research Collaboration Team, Siemens Healthineers Ltd., Wuhan, China
Synopsis
Keywords: AI/ML Image Reconstruction, Cancer
Motivation: MRI is a powerful diagnosis tool for renal tumors with a long acquisition time. How to improve image quality while shortening acquisition time is a major research focus.
Goal(s): To use a deep learning (DL) algorithm to reconstruct low-resolution T2-weighted turbo spin-echo (TSE) renal MRI scans and compare with standard-resolution T2-weighted TSE sequence.
Approach: A total of 14 patients with clinically suspected renal tumors who underwent renal low-resolution DL-reconstructed T2-weighted TSE sequence(T2DL) and standard-resolution T2-weighted TSE sequence (T2S) were included.
Results: T2DL reduced acquisition time by 32% and improved overall image quality compared with T2S.
Impact: A DL reconstruction method for low-resolution renal T2-weighted TSE sequence has the potential to reduce acquisition time and improve image quality compared with standard acquisition method, which may help detect renal lesions early and improve the survival rates of patients.
Introduction
Renal tumors are one of the most common malignant tumors in the urinary system, accounting for 3% of all cancers[1]. Renal MRI, especially the T2-weighted turbo spin echo (TSE) sequence, is a non-invasive imaging method that can help detect renal tumors early. However, the image quality of T2-weighted TSE sequences is affected by multiple factors, including acquisition time, motion, and respiratory artifacts. In recent years, deep learning (DL) reconstruction algorithms combined with compressed sensing technology can reconstruct high-quality images from under-sampled data and reduce acquisition time by utilizing neural network models[2, 3]. Therefore, this study aimed to use a DL algorithm to reconstruct a low-resolution T2-weighted TSE renal MRI sequence acquired with low spatial resolution and compare it qualitatively and quantitatively with standard-resolution T2-weighted TSE sequence.Methods
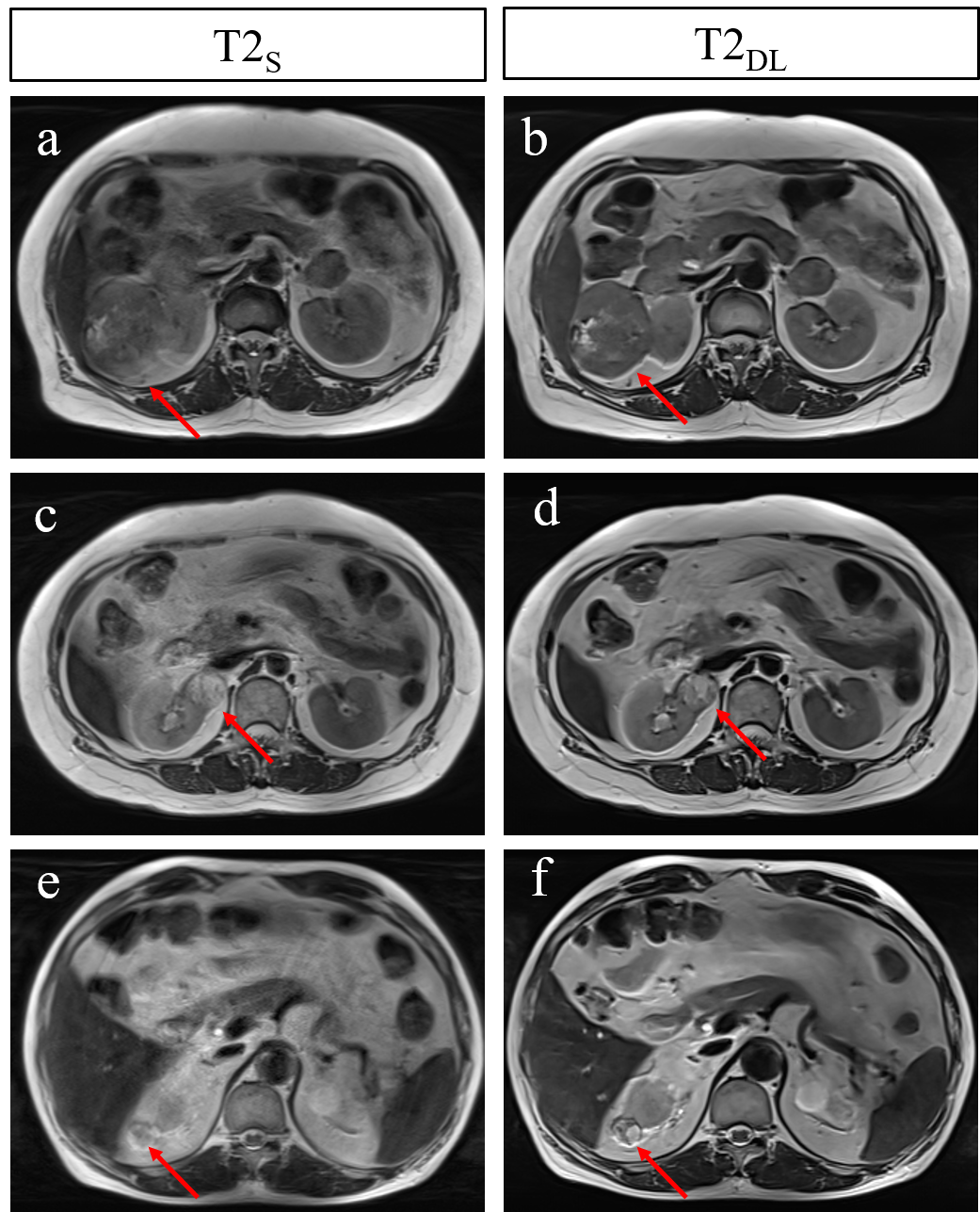
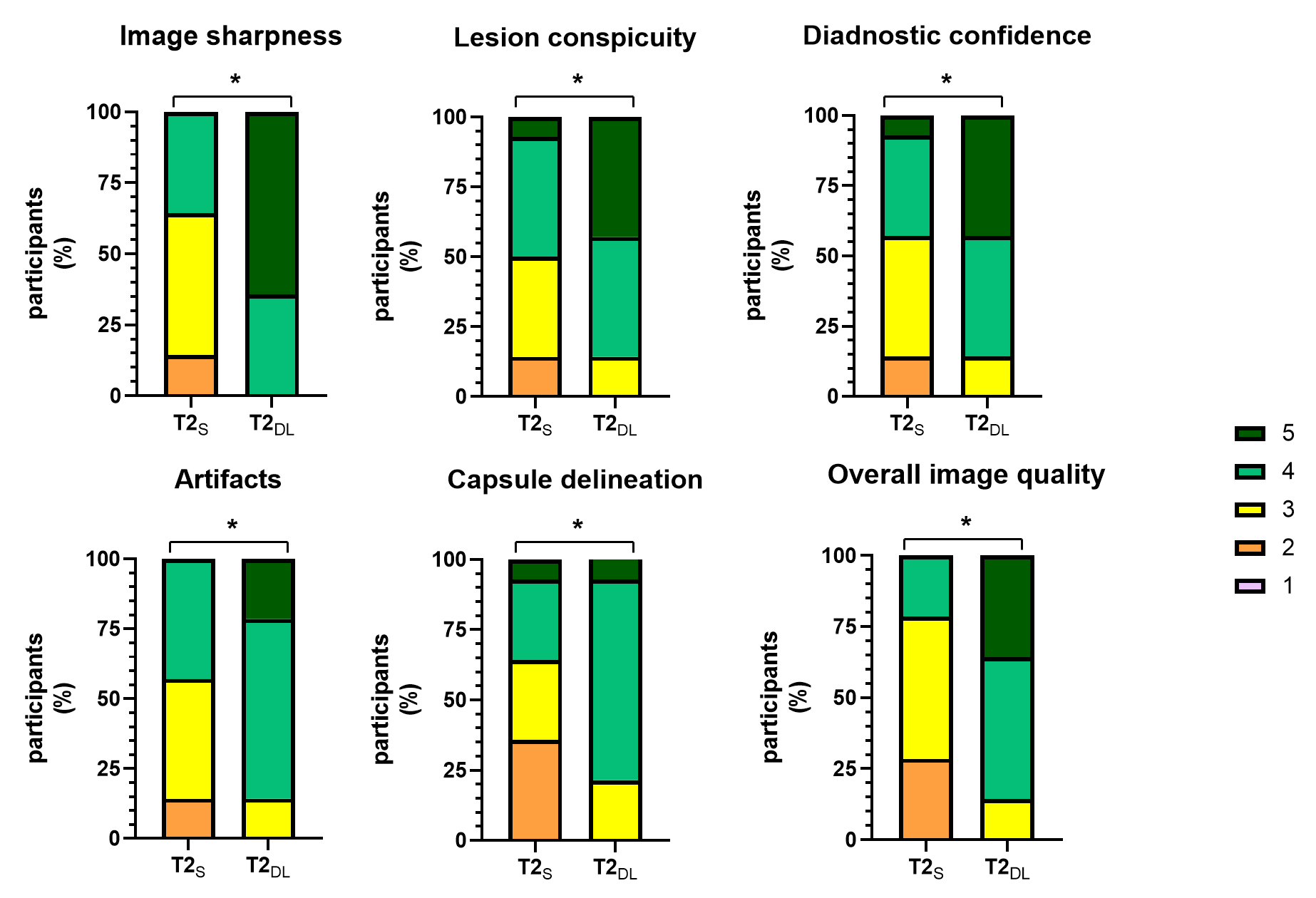
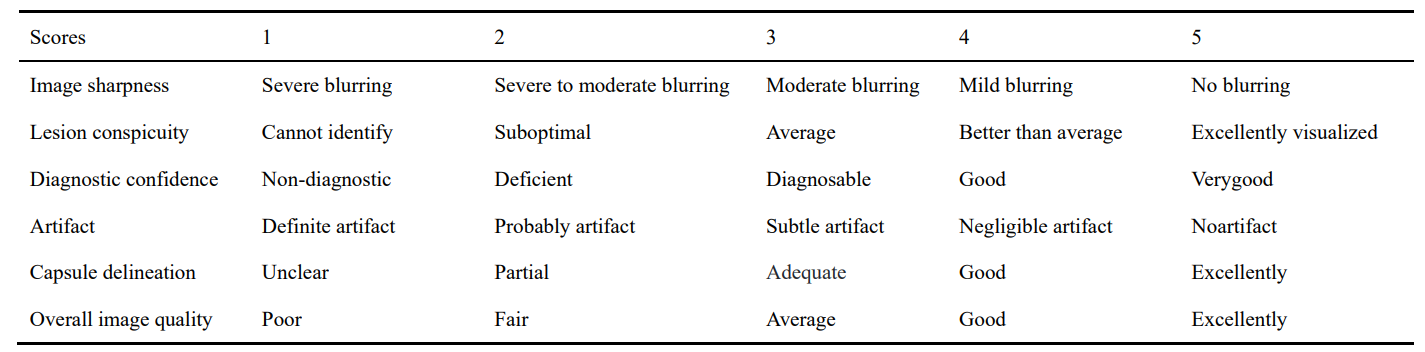
This study prospectively included 14 patients with clinically suspected renal tumors who underwent renal MRI including standard-resolution T2-weighted TSE sequence(T2S) and low-resolution DL reconstructed T2-weighted TSE sequence(T2DL) before surgery on a 3T MR scanner (MAGNETOM Skyra, Siemens Healthcare, Erlangen, Germany) with use of a 18-channel abdominal coil. Patients with general contraindications to MRI, or severe claustrophobia were excluded from the study. The T2S parameters were: TR/TE=3690/65ms; FOV=380x380mm; voxel size=1.0mmx1.0mmx3.0mm; acquisition time=3:32s. The T2DL parameters were: TR/TE=3690/65ms; FOV=380x380mm; voxel size=1.0mmx1.0mmx3.0mm; acquisition time=2:25s. Image quality of the T2S and T2DL were qualitatively assessed by two radiologists using a five-point Likert scale(Table 1). The categories evaluated included image sharpness, lesion conspicuity, diagnostic confidence, artifacts, capsule delineation, and overall image quality. Quantitative analysis was conducted by calculating the signal intensity, noise, signal-to-noise ratio (SNR) and contrast-to-noise ratio (CNR) for the renal parenchyma, renal lesions, subcutaneous adipose tissue, and psoas muscle. Continuous variables for quantitative measurements are reported as mean ± SDs, while discrete variables for the qualitative assessment are reported as median with IQRs. Groups comparison between T2S and T2DL were performed with independent t-test for continuous variables and nonparametric rank sum test for discrete variables.Results
Comparison of Qualitative Image Evaluations For the qualitative assessment of Image sharpness, T2DL more frequently achieved the score 4 or higher(100%[14 of 14 participants]) compared with T2S(36%[5 of 14])(p<0.01).Compared with T2S, T2DL also more frequently achieved the score 4 or higher for lesion conspicuity (50%[7 of 14] vs 86%[12 of 14]), diagnostic confidence (64%[9 of 14] vs 86%[12 of 14]), artifacts (43%[6 of 14] vs 86%[12 of 14]), capsule delineation (36%[5 of 14] vs 79%[11 of 14]), and overall image quality (21%[3 of 14] vs 86%[12 of 14]) (p<0.01)(Figure 2). Comparison of Quantitative Image Evaluations The mean noise for the renal parenchyma and psoas muscle of the T2DL were 19.80±6.72 and 20.39±8.48, which were significantly lower than those of T2S (25.21±7.03 and 28.35±5.07, p<0.05). The mean noise for the lesions and subcutaneous adipose tissue of the T2DL were also lower than those of T2S, but showed no evidence of differences. Similarly, the SNR for the renal parenchyma and psoas muscle of the T2DL (24.51±7.01 and 16.88±11.95) were higher compared with those of T2S (18.84±6.99 and 9.86±2.90), but there was no evidence of differences for the lesions and subcutaneous adipose tissue between T2S and T2DL. An increasing trend of the mean CNR for T2DL compared to T2S, though there were no significant differences for the renal parenchyma, renal lesions, subcutaneous adipose tissue.Discussion
This prospective study used a DL reconstruction technique for T2-weighted turbo spin echo (TSE) in multiparametric MRI of the renal and compared it qualitatively and quantitatively with standard- resolution T2-weighted TSE sequence. Compared with standard-resolution T2-weighted TSE sequence, we found the DL reconstruction to reduce acquisition time by 32%, while improving overall image quality (median score, 4 [IQR, 4–5] for DL reconstruction vs 3 [IQR, 3–3.25; P < .001] for the standard T2-weighted TSE sequence. Compared to the standard-resolution T2-weighted TSE sequence, we observed that DL reconstruction showed a trend of reducing noise and improving the SNR and CNR of the images.Conclusion
In conclusion, we used a deep learning reconstruction method for low-resolution T2-weight TSE sequences that improved image quality and reduced acquisition time compared with standard-resolution T2-weight TSE sequence. Due to the improved image quality, this method may help detect renal lesions early and improve the survival rates of the patients.Acknowledgements
No acknowledgements found.References
1 Wong M C S, Goggins W B, Yip B H K, et al. Incidence and mortality of kidney cancer: temporal patterns and global trends in 39 countries [J]. Scientific reports, 2017, 7(1): 15698.
2 Johnson P M, Lin D J, Zbontar J, et al. Deep Learning Reconstruction Enables Prospectively Accelerated Clinical Knee MRI [J]. Radiology, 2023, 307(2): e220425.
3 Bischoff L M, Peeters J M, Weinhold L, et al. Deep Learning Super-Resolution Reconstruction for Fast and Motion-Robust T2-weighted Prostate MRI [J]. Radiology, 2No023, 308(3): e230427.
Figures