4667
Deep learning image formation for fast and high-resolution brain MRI at 0.055 tesla1Laboratory of Biomedical Imaging and Signal Processing, The University of Hong Kong, Hong Kong SAR, China, 2Department of Electrical and Electronic Engineering, The University of Hong Kong, Hong Kong SAR, China
Synopsis
Keywords: AI/ML Image Reconstruction, Low-Field MRI, Brain
Motivation: High, isotropic resolution (e.g., 1mm) is desirable for lesion detection and biomarkers extraction for cognitive disorders. However, ultra-low-field (ULF) MRI severely suffers from low spatial resolution and signal-to-noise ratio.
Goal(s): To investigate the potential of 3D deep learning in generating <=1mm isotropic resolution results from 2D partial Fourier-sampled, low-resolution noisy brain images acquired from our custom-made 0.055T scanner.
Approach: We advanced 3D deep learning partial Fourier reconstruction and super-resolution method (PF-SR) to achieve 3x/4x super-resolution factors.
Results: Preliminary results indicate possibility of PF-SR with higher super-resolution factors on reconstructing experimental ULF T1w/T2w data to 1/0.75mm3 with reduced artefacts and noise.
Impact: Enhancing image resolution and fidelity for fast ultra-low-field brain imaging at 0.055T using data-driven 3D deep learning approach to <=1mm3 resolution potentially enables image-guided therapies and valuable neuroimaging analysis for assessing aging and cognitive conditions.
Introduction
Low-cost, ultra-low-field (ULF) MRI suffers from significantly lower SNR1-3 which limits spatial resolution, and multiple acquisitions are often needed to boost SNR, hindering its clinical value and adoption. Deep learning (DL) approaches have shown promising results in improving image quality of ULF images4,5. Recently, we developed a 3D DL method (PF-SR)6 for simultaneous partial Fourier (PF) reconstruction, denoising and super-resolution (SR) for 2D PF-sampled, noisy, low-resolution 3D isotropic brain images acquired from our custom-built 0.055T MRI scanner7. PF-SR demonstrated the potential of achieving high 3D image fidelity for fast ULF MRI with 3-min scan time. Yet, it was limited with a SR factor of 2x, giving only 1.5mm3 isotropic resolution results. High and isotropic resolution such as 1mm3 is more compelling and desirable as insufficient resolution can impede identification of tiny lesions and valuable downstream analysis of such structural neuroimaging data.Unlike traditional interpolation methods or SR with multiple shifted images8,9, supervised deep learning approaches can leverage priors extracted from the training process using large-scale, high quality MRI dataset to recover loss of information. This presents a unique opportunity of tackling the ill-posed single image formation (reconstruction and restoration) problem with high SR factors. In this study, we explored the feasibility and potential of PF-SR to address the considerably more ill-posed and important problem of achieving 1mm3 and sub-millimetre (0.75mm3) isotropic resolution with 3x and 4x super-resolution factor respectively.
Methods
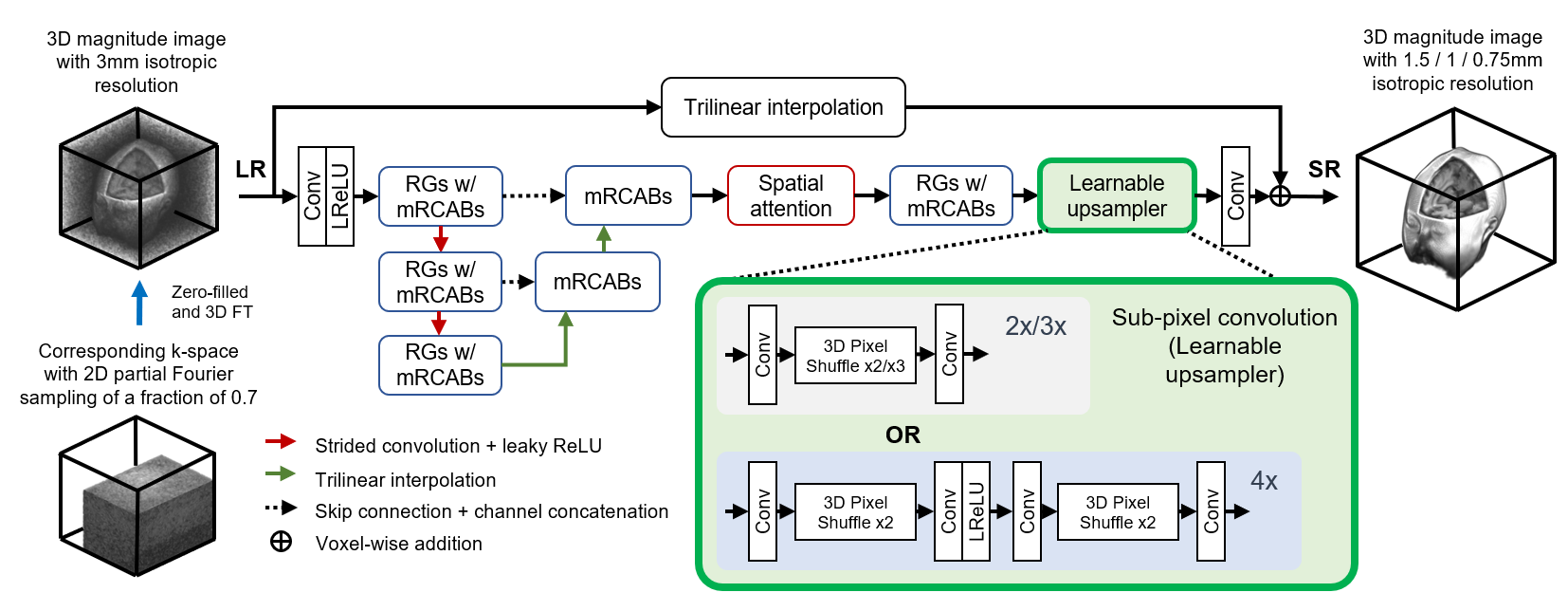
We adopted the basic PF-SR architecture we recently implemented6. We modified it for 3x and 4x SR factors while maintaining similar model complexity (Figure 1): (i) 3x PF-SR shared the same learnable upsampler as 2x model, but channel size of first convolution layer was increased to 1728, allowing upsampling factor of 3 after 3D pixel shuffle. (ii) For 4x PF-SR, two consecutive sub-pixel convolutions were employed, each with upsampling factor 2.T1w and T2w models of different SR scales were trained from scratch and separately with 1248 T1w and 1182 T2w brain data, respectively, synthesised from HCP S1200 dataset10. Data were resampled to 1.5/1/0.75mm3 resolution as training targets for 2x/3x/4x SR factor respectively. Corresponding training inputs of 3mm3 resolution were generated via k-space cropping and retrospective 2D PF sampling of fraction=0.7 in both phase-encoding (PE) directions. We added Rician noise of level comparable to experimental data acquired by our 0.055T head scanner.
We used AdamW optimiser with weight decay=1e-2, batch size=8 on 4 Nvidia A100 GPUs. Random cropping with training patch size=32x32x32 and horizontal flipping were performed. All models were trained for 350 epochs using L1 loss with initial learning rate=1e-4 following a decay by factor of 2 every 50 epochs. We tested the models on both synthetic and experimental ULF data and compare the results with 3T high-resolution references. Experimental ULF data were previously acquired using our 0.055T head scanner7 with single NEX and prospective PF-sampling of fraction=0.7 along two PE directions following the parameters described in paper6.
Results
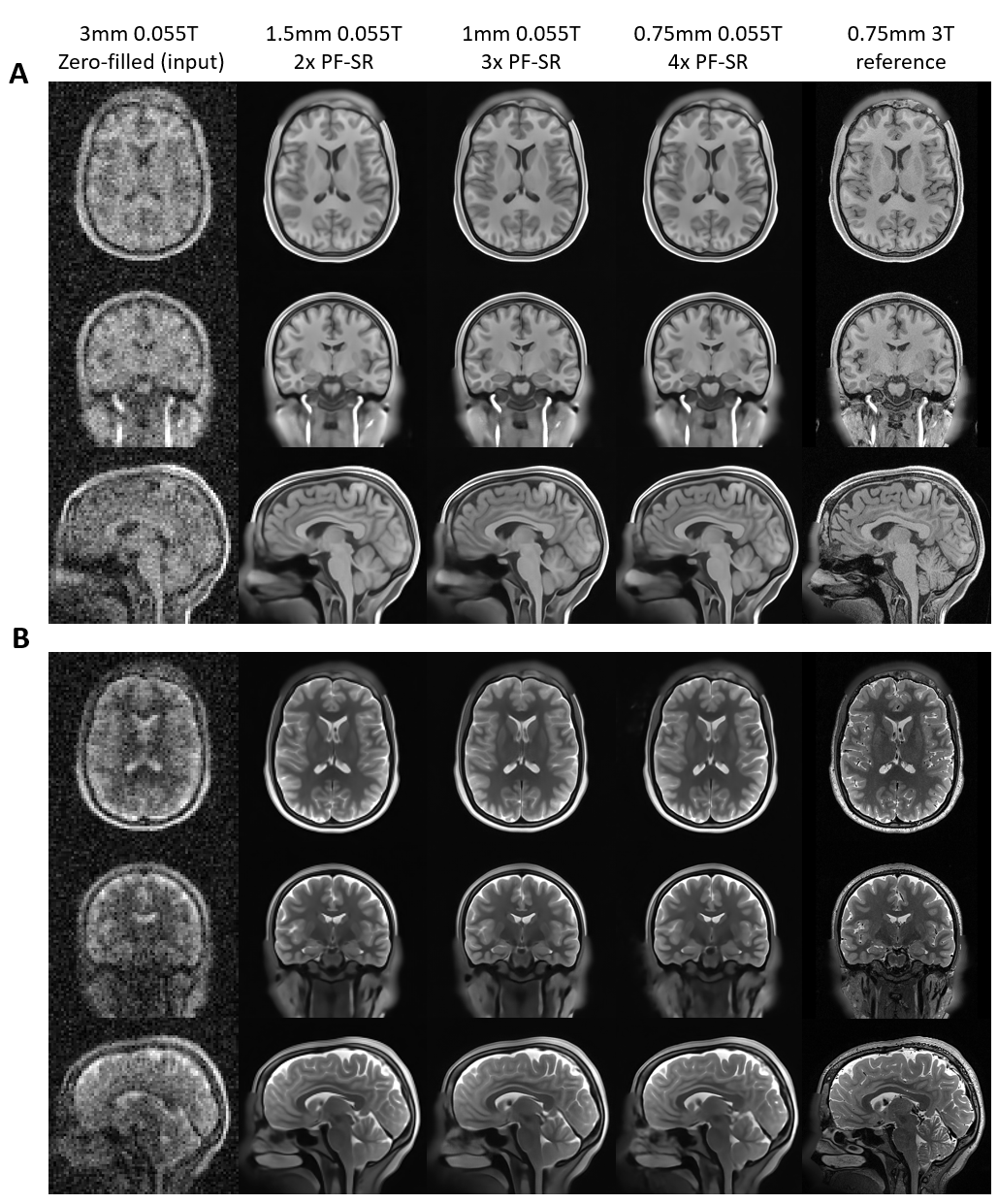
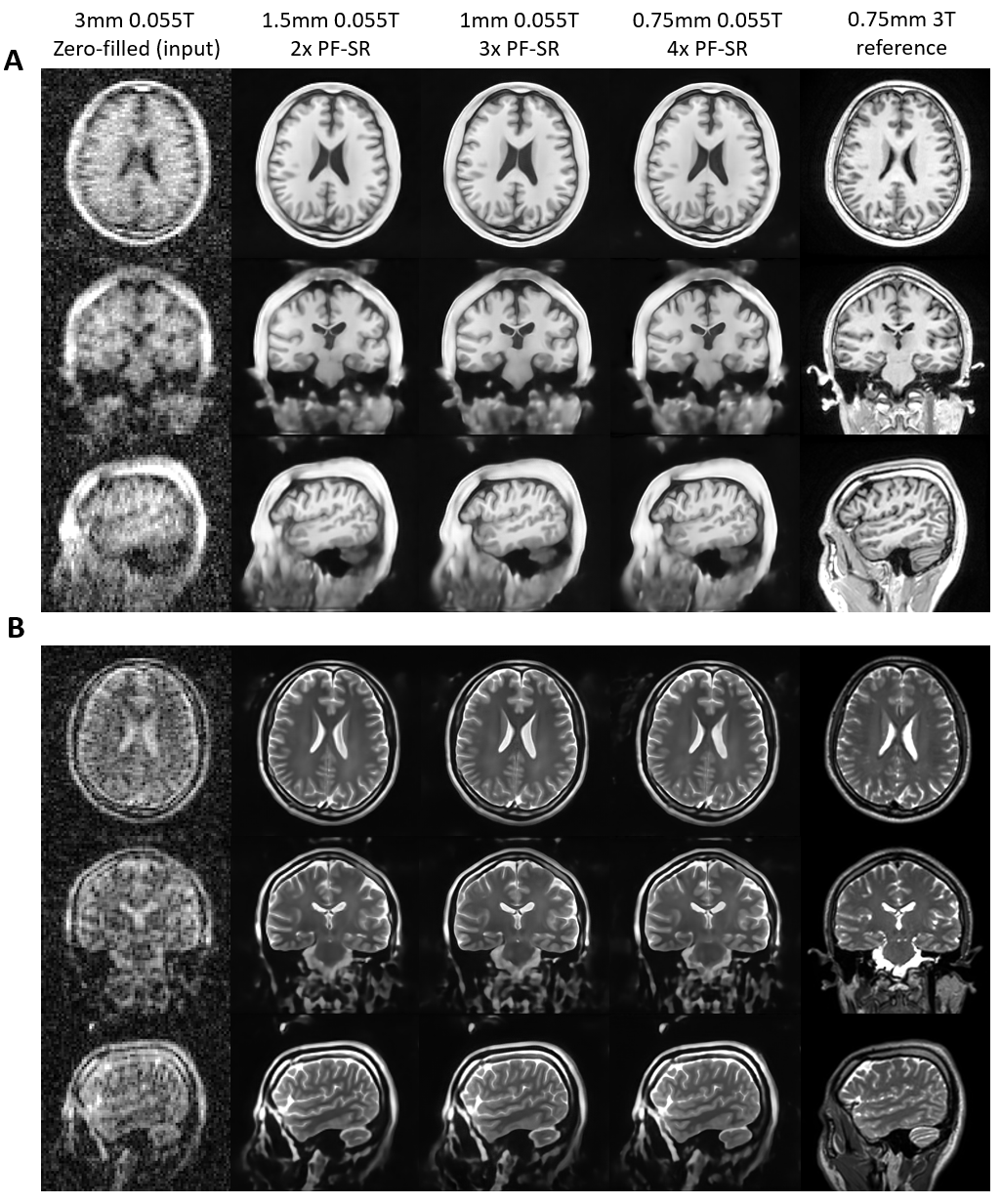
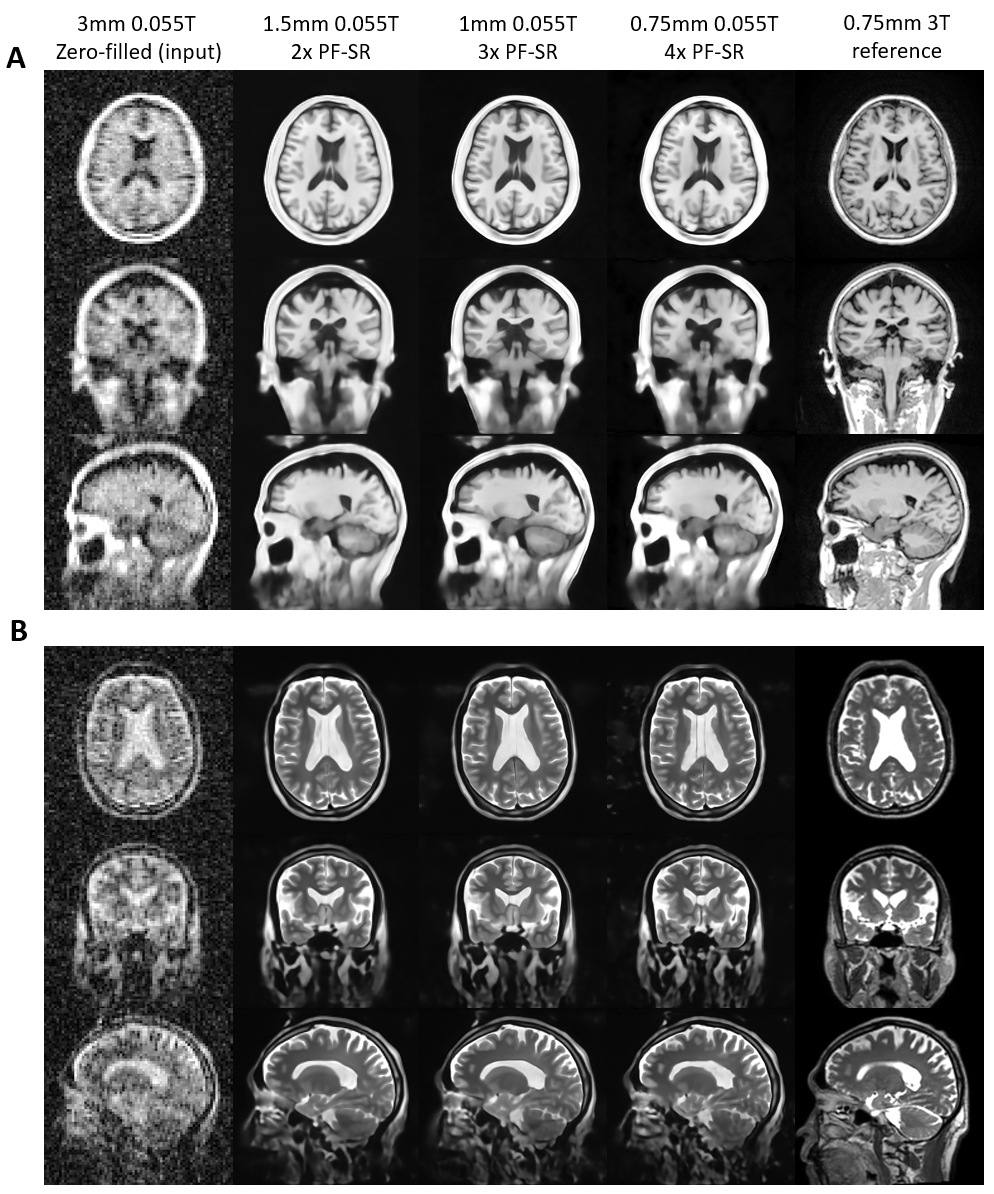
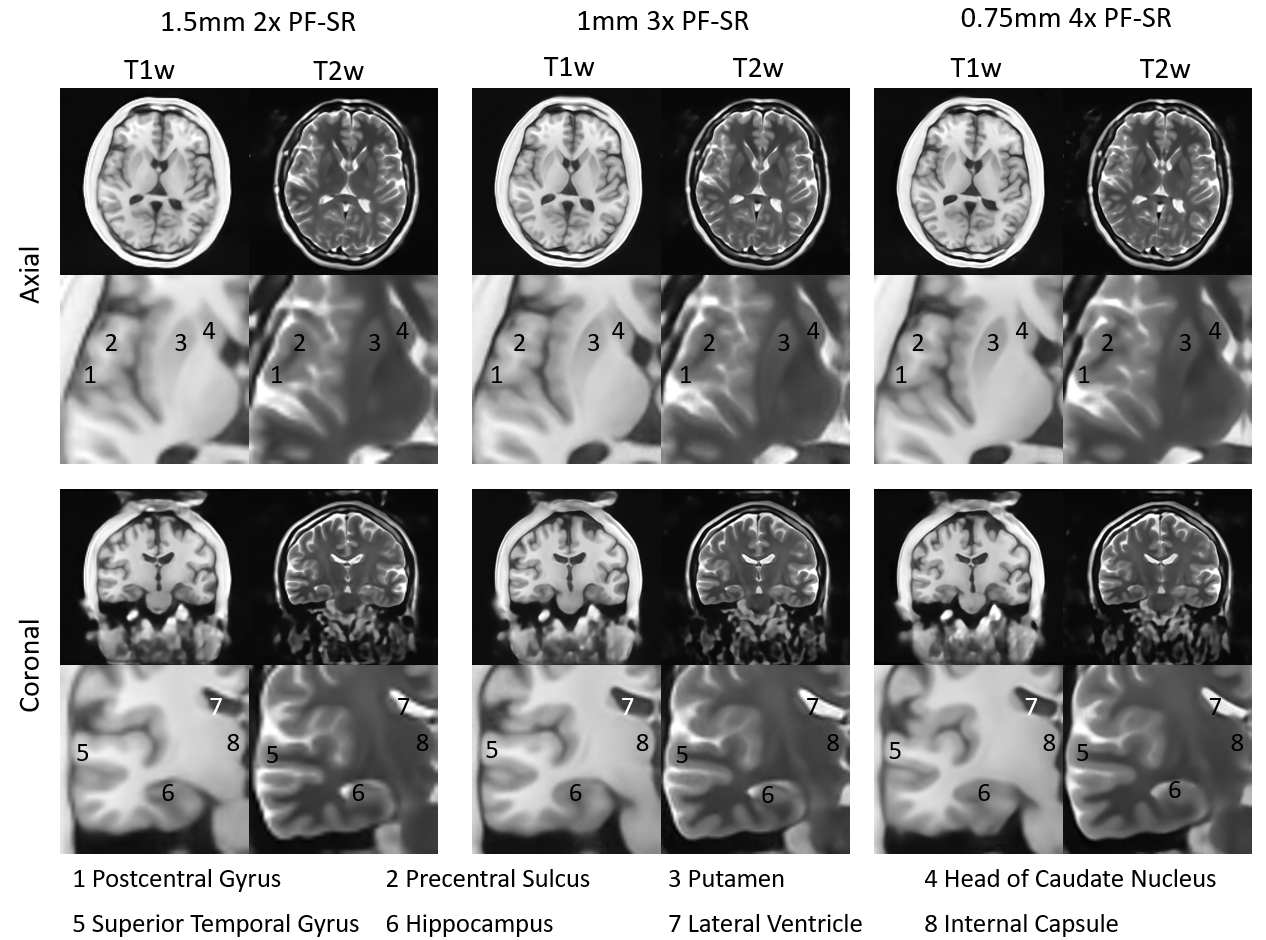
Figure 2 presents the typical reconstruction results of synthetic ULF data for different super-resolution factors. Figure 3 and 4 show the reconstruction results of experimental ULF T1w and T2w data from one young and two elderly subjects, respectively. Similar to results from 2x PF-SR, PF-SR with 3x/4x SR factor effectively reduced Gibbs-ringing artefacts, noise and recovered structures of both synthetic and experimental data but with improved clarity. However, 4x PF-SR is more prone to mistaken noise and/or artefacts as structure. The contrast consistency experiment among T1w and T2w images (Figure 5) revealed the consistency and complementarity of appearance of structural details produced by 3x and 4x PF-SR even if T1w and T2w models were trained separately, indicating PF-SR’s ability in reconstructing anatomical details.Discussion and Conclusion
In this study, we demonstrated the potential of advancing PF-SR to 4x SR factors. PF-SR of higher SR factors give sharper results with similar artefacts and noise suppression in both synthetic and experimental ULF T1w and T2w data.Fast ULF MRI for 3D T1w and T2w images with 1/0.75mm3 isotropic resolution potentially allows for structural volumetric quantification for assessing brain aging and neurodegenerative diseases. Potential biomarkers such as hippocampal and putamen volume associated with cognitive decline and disorders like Alzheimer’s11,12 and Huntington’s disease13 require (sub-)millimetre resolution for optimal segmentation and volumetric measurements. Precious information on brain development14 and aging process15,16 may also be obtained via measuring white and grey matter volume changes. The high resolution may also enable image-guided therapies17-20. However, more careful examinations including quantitative analysis, testing on patient data with robust radiological assessment are required in future studies.
Acknowledgements
This work was supported in part by Hong Kong Research Grant Council (R7003-19F, HKU17112120, HKU17127121, HKU17127022 and HKU17127523 to E.X.W).References
1. Hoult DI, Richards R. The signal-to-noise ratio of the nuclear magnetic resonance experiment. Journal of Magnetic Resonance (1969) 1976;24(1):71-85.Figures