4666
Deep Learning Reconstruction-based Accelerated Rectal MRI: Image Quality, Diagnostic Performance, and Reading Efficiency Assessment1Department of Radiology, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy, Beijing, China, 2GE Healthcare China, Beijing, China
Synopsis
Keywords: AI/ML Image Reconstruction, Tumor, Rectal adenocarcinoma, Imaging quality, Diagnostic performance
Motivation: Accelerated MRI is an imminent need clinically to satisfy the growing disease burden of rectal cancer.
Goal(s): This study aims to conduct clinical assessment of DLR-based accelerated rectal MRI, encompassing image acquisition, image quality, diagnostic performance, and reding efficiency.
Approach: Two sets of T2WI using standard fast spin-echo (FSEstandard) and DLR-based accelerated FSE (FSEDL) were prospectively compared.
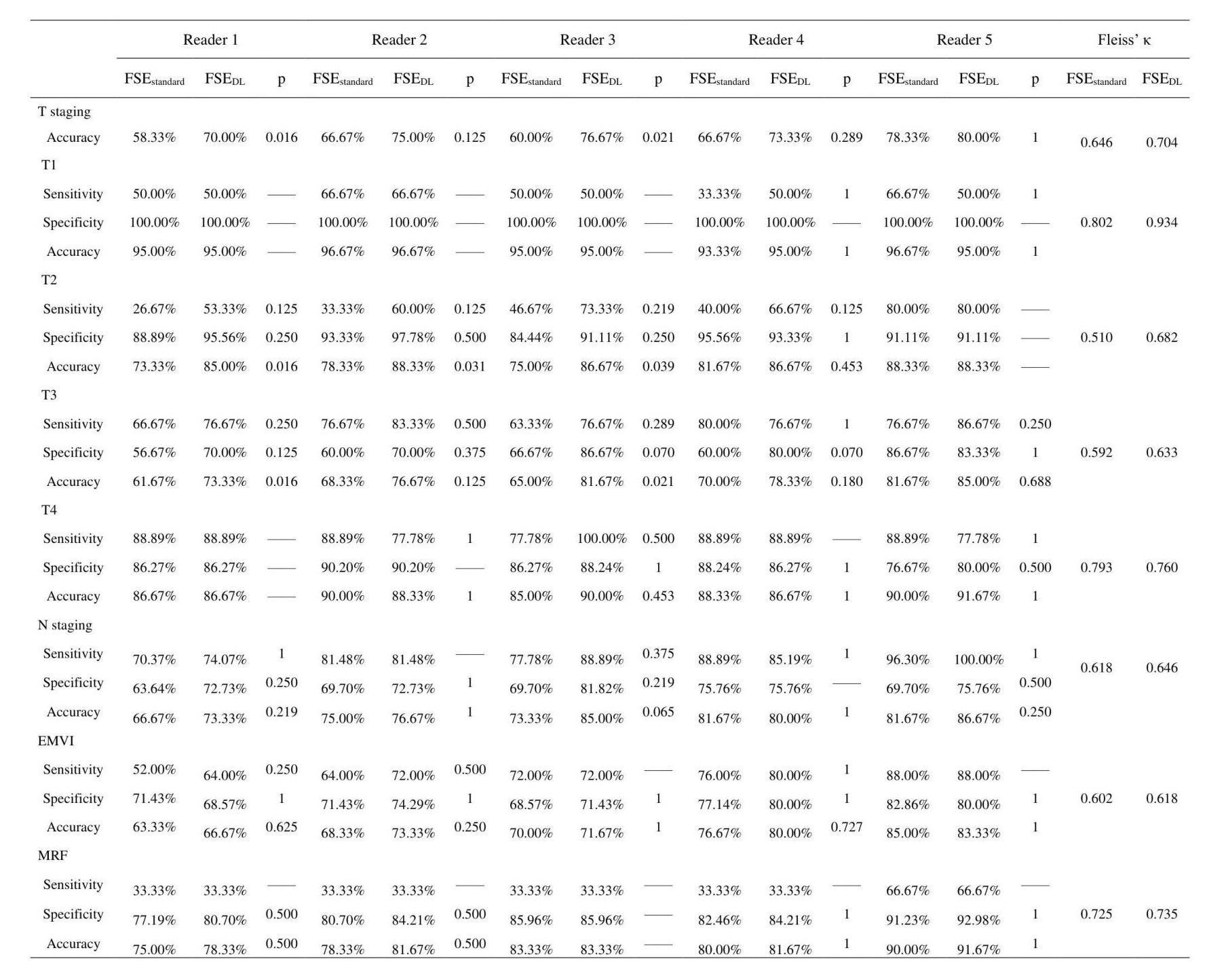
Results: FSEDL showed superior image quality and reading efficiency than FSEstandard, with a 65% reduction in acquisition time. DLR could assist to enhance the accuracy of T-staging for junior radiologists, preserving equivalent diagnostic performance in N staging, EMVI, and MRF.
Impact: This study offered a comprehensive and viable perspective on the application of DLR in rectal MRI, which facilitated improved image quality and reading efficiency, while reducing acquisition time. Moreover, it enhanced the accuracy of T-staging for junior radiologists.
Introduction
Colorectal cancer is the third most prevalent cancer worldwide, with rectal cancer constituting approximately one-third of these cases 1. Alarmingly, this proportion continues to rise 2, exacerbating the disease burden of rectal cancer globally. Magnetic Resonance Imaging (MRI) serves as the preferred and standard imaging modality for rectal cancer assessment. Acquiring superior image quality in shorter time, without compromising data integrity has become an imminent issue in need of resolution to satisfy the growing disease burden of rectal cancer. Deep learning reconstruction (DLR) has demonstrated its ability to enhance the image quality of accelerated MRI in multiple organs 3,4. However, its application to rectal MRI remained rarely reported. The rectum, characterized as a hollow organ, features a unique anatomical structure, which makes its image susceptible to the functional peristalsis and dynamics contraction and relaxation of the intestinal wall. Therefore, assessing the applicability of DLR for rectal MRI in real clinical scenarios is imperative.This study aimed to provide comprehensive perspective on the practical application of DLR-based rectal MRI in comparison to standard MRI, encompassing image acquisition time, image quality, in particular, diagnostic performance and reding efficiency.
Methods
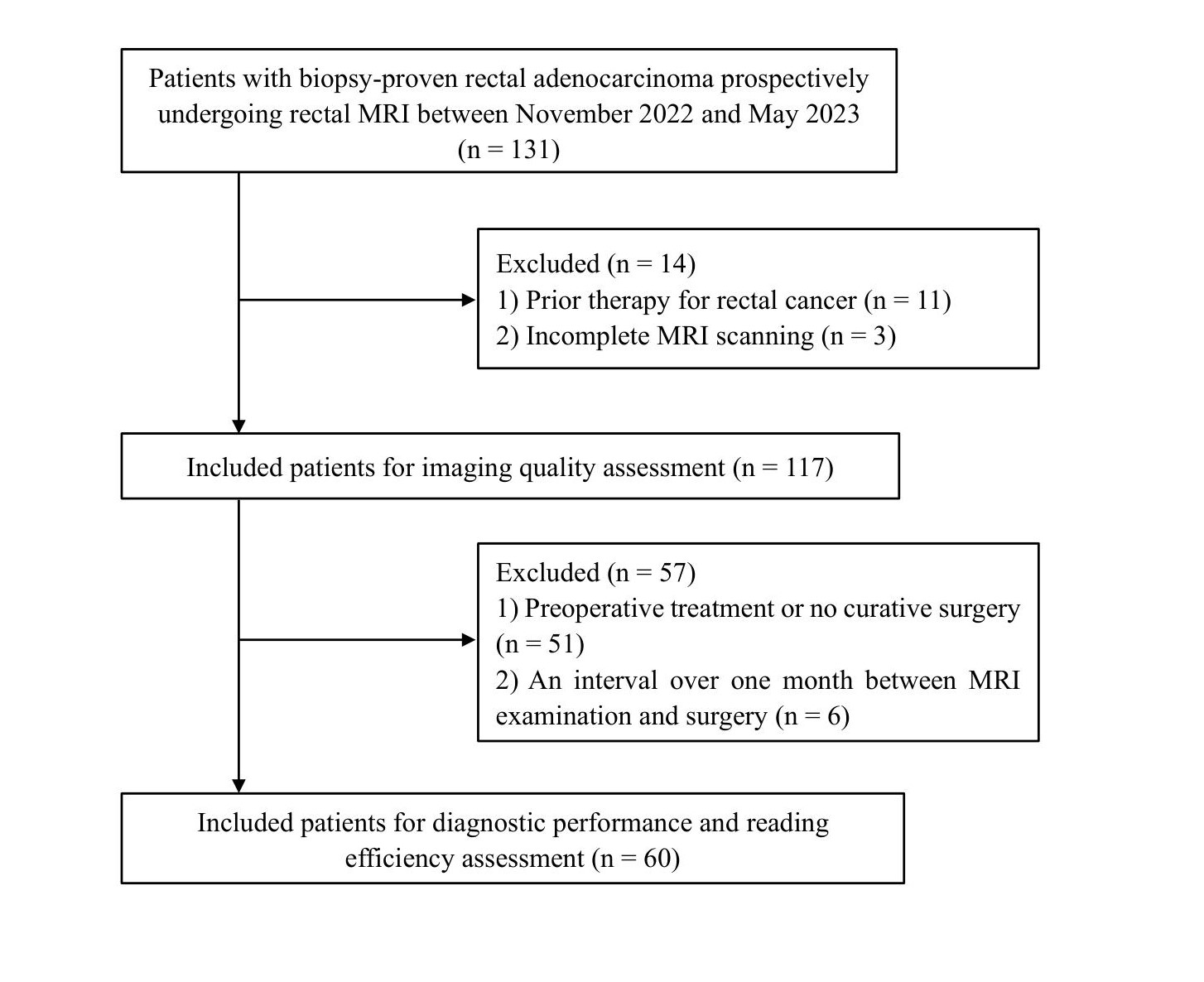
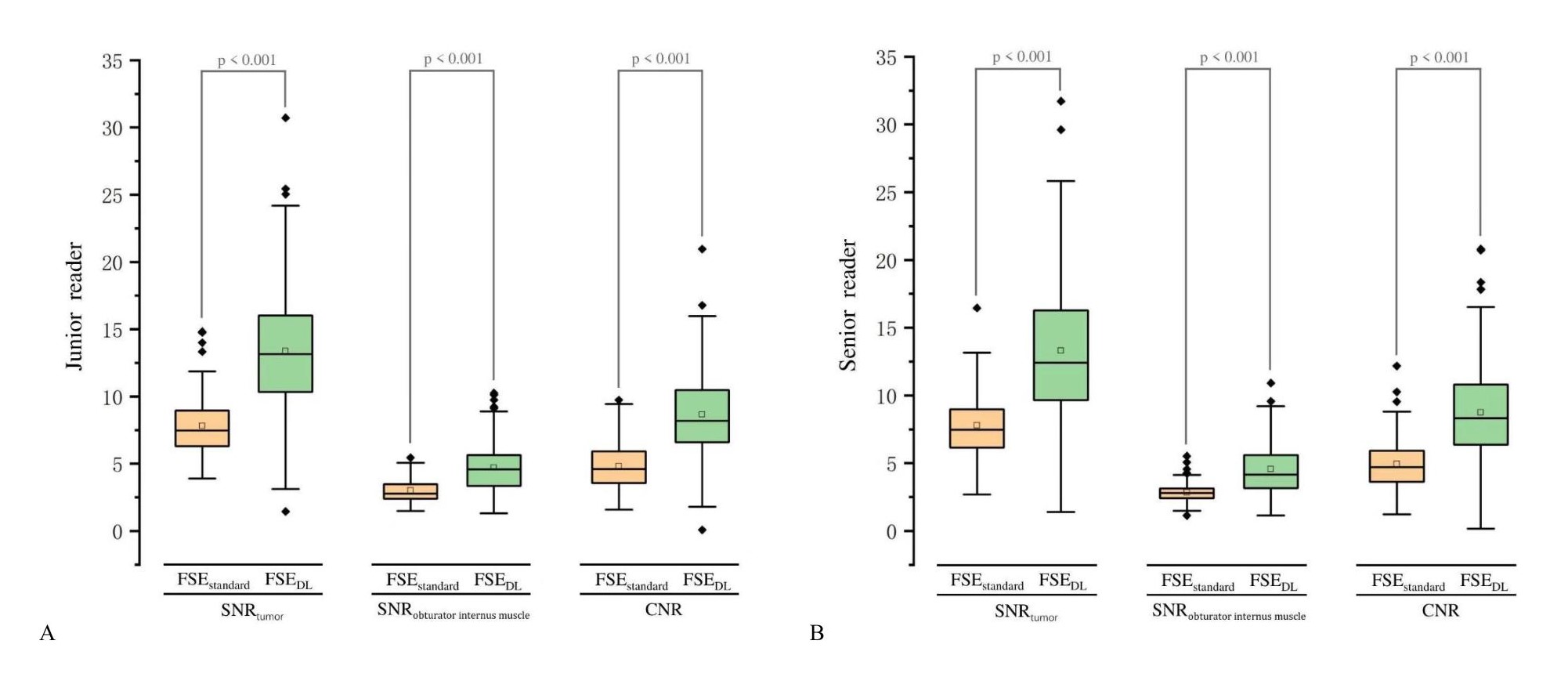
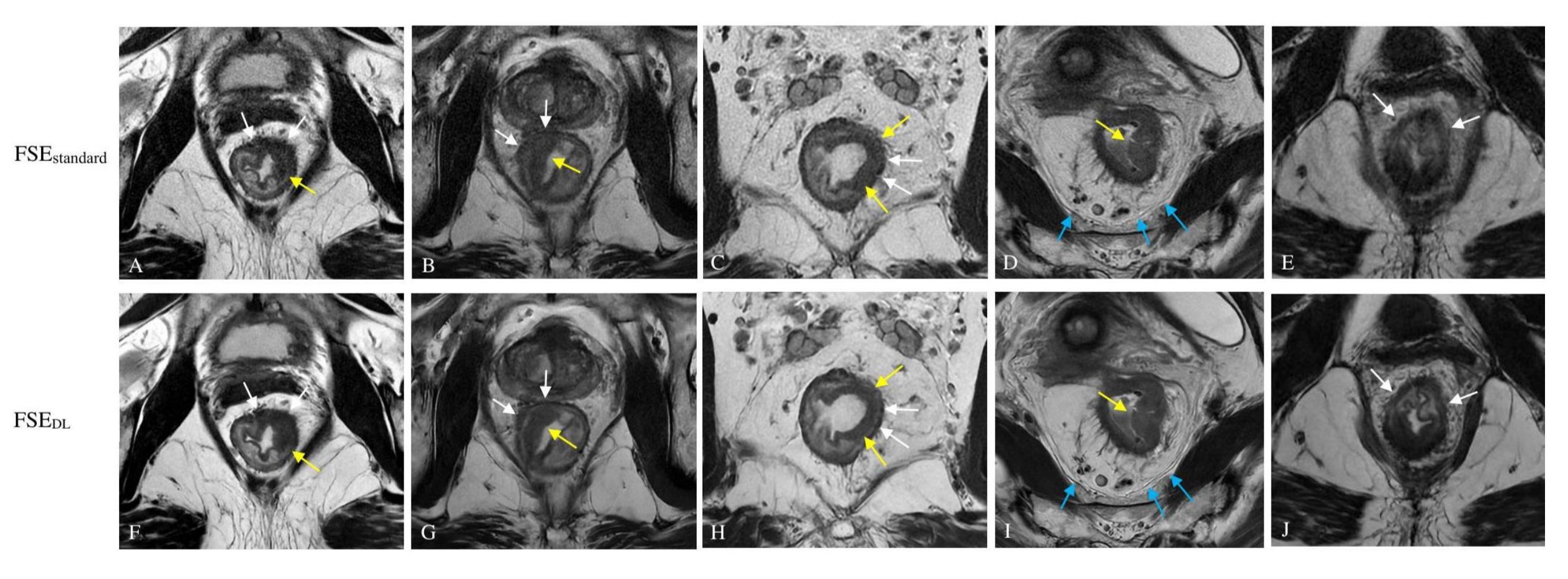
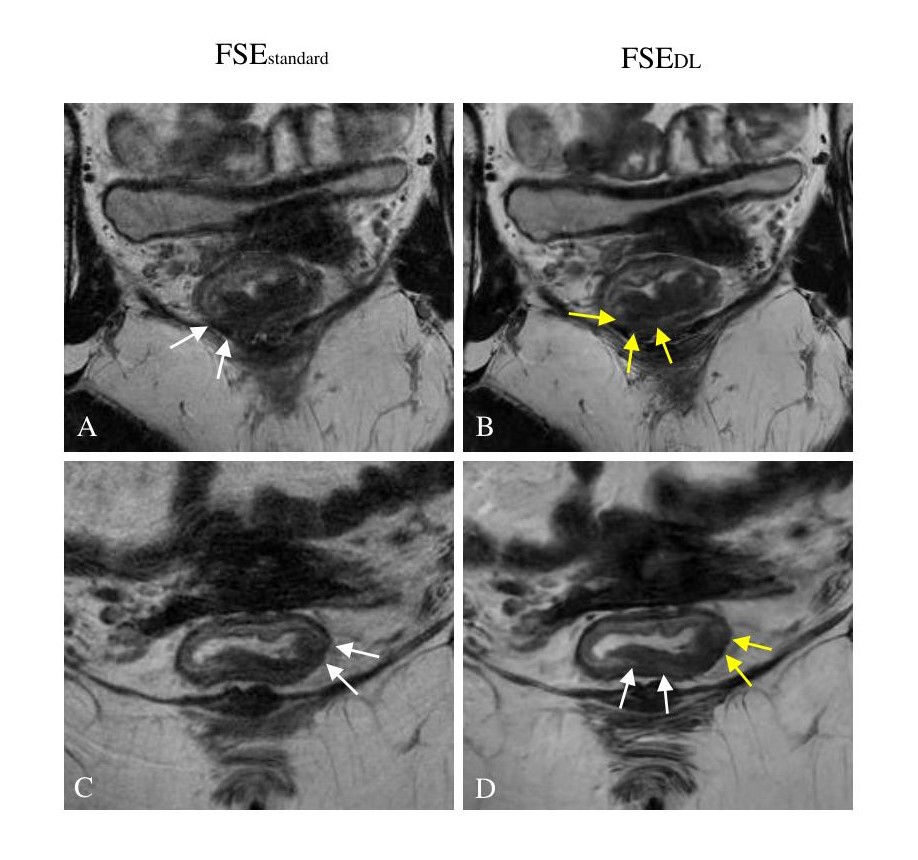
Patients: With approval from the institutional review board, consecutive patients with biopsy-proven primary rectal adenocarcinoma between November/2022 and May/2023 were prospectively included. Imaging: Two key sets of oblique axial T2WI using standard FSE (FSEstandard) and DLR-based accelerated FSE (FSEDL) performed using a 3.0-T MRI system (AIR™ Architect; GE Healthcare, Milwaukee, Wis) were obtained for comparative analysis. Evaluation methods: Imaging quality assessment was conducted using quantitative and qualitative methods and evaluated separately for two protocols. Quantitative image quality assessment was based on region-of-interest measurements. Three parameters including signal-noise ratio (SNR) of the tumor (SNRtumor), SNR of the internal obturator muscle (SNRinternal obturator muscle), and contrast-noise ratio (CNR) between the tumor and internal obturator muscle were calculated respectively for two sequences. Qualitative image quality metrics regarding artifacts, noise, tumor margin clarity, visualization of bowel wall layering, visualization of mesorectal fascia, overall image quality, and diagnostic confidence were assessed based on a five-point Likert scale, whereby larger scores indicate better: 1 – non-diagnostic; 2 – poor but still interpretable; 3 – acceptable; 4 – good; 5 – excellent. Patients undergoing curative surgery without preoperative treatment were re-selected for diagnostic performance and reading efficiency evaluation. Diagnostic assessment included T-staging, N-staging, extramural vascular invasion (EMVI), and mesorectal fascia (MRF) involvement, which was conducted by five radiologists with different levels of experience, as compared with surgical pathology results. To mitigate subjective recall bias, the FSEstandard and FSEDL imaging was analyzed separately in a random and mixed order, with at least three weeks of washout period between two reviews. Each consuming time of four diagnostic metrics (mrT staging, mrN staging, mrEMVI, and mrMRF) and total time summing up the four metrics in two sequences (FSEstandard and FSEDL) was recorded for five readers for reading efficiency analysis. Data processing: Comparison of the imaging quality and diagnostic time between FSEstandard and FSEDL was conducted using paired-sample t-test or Wilcoxon signed-rank test. The diagnostic efficiency was compared by McNemar's test. Intra- and inter-reader agreement was assessed by intraclass correlation coefficient, Cohen’ s κ and Fleiss’ κ.Results
Totally, 117 patients (77 males; age range 21 – 77 years) were enrolled, with 60 patients (36 males; age range 32 – 77 years) undergoing radical surgery. DLR reduced acquisition time by 65% than standard MRI. Moderate to excellent intra- and inter-reader agreement was achieved for all assessment metrics. FSEDL exhibited higher SNRtumor, SNRinternal obturator muscle, CNR, and subjective scores related to noise, tumor margin clarity, visualization of bowel wall layering and mesorectal fascia, overall image quality, and diagnostic confidence than FSEstandard (p < 0.001). Reduced artifacts were observed in FSEDL compared to FSEstandard for patients without spasmolytics (p < 0.05). FSEDL was rated higher accuracy of T-staging than FSEstandard by junior readers (reader 1, 58% vs. 70%, p = 0.016; reader 3, 60% vs.76%, p = 0.021), with comparable performance in evaluating N-staging, EMVI, and MRF. No significant difference was found concerning all the diagnostic performance by senior readers (p > 0.05). FSEDL exhibited shorter diagnostic time in T-staging and overall evaluation by all readers, as well as in EMVI and MRF by junior readers (p < 0.05).Discussion and Conclusions
FSEDL was clinically viable for rectal MRI, which could facilitate substantial improvements in image quality and reading efficiency than FSEstandard, with a 65% reduction in acquisition time. Moreover, it had the potential to assist junior radiologists in enhancing the diagnostic accuracy of T-staging.Acknowledgements
Funding: This work was supported by CAMS Innovation Fund for Medical Sciences (CIFMS) [grant number 2021-I2M-C&T-A-017]; Capital’s Funds for Health Improvement and Research (CFH) [grant number 2022-2-4024]; the National Natural Science Foundation of China [grant number 81971589]; 2020 SKY Imaging Research Fund [grant number Z-2014-07-2003-01]; and CAMS Innovation Fund for Medical Sciences (CIFMS) [grant number 2022-I2M-C&T-B-077].
References
1. Siegel, R. L., Miller, K. D., Wagle, N. S., & Jemal, A. (2023). Cancer statistics. CA: a cancer journal for clinicians. 2023;73(1):17–48.
2. Siegel, R. L., Wagle, N. S., Cercek, A., Smith, R. A., & Jemal, A. (2023). Colorectal cancer statistics. CA: a cancer journal for clinicians. 2023;73(3):233–254.
3. Ueda T, Ohno Y, Yamamoto K, et al. Deep Learning Reconstruction of Diffusion-weighted MRI Improves Image Quality for Prostatic Imaging. Radiology. 2022;303(2):373-381.
4. Johnson PM, Lin DJ, Zbontar J, et al. Deep Learning Reconstruction Enables Prospectively Accelerated Clinical Knee MRI. Radiology. 202;307(2):e220425.
Figures