4664
Deep learning-based image reconstruction for higher resolution cardiac T1 mapping1Medical Image and Data Analysis (MIDAS.lab), Department of Diagnostic and Interventional Radiology, University of Tuebingen, Tuebingen, Germany, 2Siemens Healthineers AG, Erlangen, Germany, 3Friedrich-Alexander-Universität Erlangen-Nürnberg, Erlangen, Germany, 4Diagnostikum, Berlin, Germany
Synopsis
Keywords: AI/ML Image Reconstruction, Quantitative Imaging, T1 mapping, Higher resolution, Deep learning-based Image reconstruction
Motivation: The MOLLI acquisition scheme is frequently used for T1 mapping of the heart. MOLLI restricts the spatial resolution of the resulting T1 maps due to acquiring the inversion recovery images in single-shot fashion.
Goal(s): To allow the acquisition of higher spatial resolution T1 maps.
Approach: Single-shot acquisitions are accelerated and image sets are reconstructed using a neural network. The deep learning-based reconstruction is integrated into an existing T1 mapping sequence.
Results: The proposed method produces higher spatial resolution T1 maps. The corresponding T1 values do not differ significantly from T1 values computed by the vendor sequence.
Impact: The acquisition of higher spatial resolution T1 maps is achieved. The proposed method may improve the detection of small focal lesions without increasing the required scan time or breath hold duration.
Introduction
A widely used quantitative imaging technique in cardiac MRI is T1 mapping, as it allows for non-invasive tissue characterization and the calculation of diagnostically relevant biomarkers1. The modified look-locker inversion recovery scheme (MOLLI) is frequently utilized for this2. While MOLLI allows for the acquisition of a sufficient number of inversion recovery samples required for T1 estimation during a single breath hold, it does pose constraints in terms of resolution and scan time, as inversion recovery images are acquired in single-shot fashion.Recent literature suggests multiple possible solutions to overcome these restrictions3,4,5. In this work, a variational network6 is implemented to reconstruct accelerated MOLLI acquisitions. The network is integrated into an existing T1 mapping reconstruction to allow for the acquisition of higher spatial resolution T1 maps.
Materials and Methods
A version of the end-to-end variational network was adapted. Given the entire MOLLI acquisition as input, the network uses a 2D+t convolution scheme allowing to incorporate redundancies across the contrast dimension during reconstruction7. A learnable weighting of the regularization term in k-space was used to allow each cascade to focus on specific regions of k-space8. A bias field correction9 was applied to both the target and predicted images before loss computation. Two separate networks were trained for acceleration rates 3 and 4. Both networks consisted of a total of 15 cascades and were trained for 100 epochs using an Adam optimizer with a learning rate of 0.005.A dataset consisting of 1750 MOLLI 5(3)3 acquisitions in short axis view was used for training (1600), validation (50) and testing (100) of the networks. The data was acquired using the vendor T1 mapping sequence with an acceleration factor of 2. The corresponding GRAPPA10-interpolated k-space was regarded as “fully sampled” ground truth and retrospectively undersampled by factors 3 and 4 using an equispaced undersampling mask.
Additionally, 10 MOLLI 5(3)3 scans were acquired prospectively in healthy volunteers using the above-mentioned sequence and 2 modified versions. One uses an acceleration rate of 3 and increases the phase resolution from 66% to 90% and the spatial resolution from 1.41x2.13 mm2 to 1.32x1.46 mm2. The second increases the acceleration rate to 4, the phase resolution to 100% and the spatial resolution to 1.18x1.18 mm2.
All data was acquired on clinical 3T scanners (MAGNETOM Skyra, Vida, Lumina, Cima.X, Siemens Healthineers AG, Erlangen, Germany).
The network was integrated into an existing vendor reconstruction for T1 mapping using the FIRE11 framework. The original reconstruction uses GRAPPA followed by a motion compensation step and a parametric fit. In the modified reconstruction, GRAPPA is replaced by the respective variational network.
The variational networks were evaluated in terms of image quality in the reconstructed images. The results were compared to the ground truth images using SSIM, PSNR and NMSE. The higher resolution mapping sequences using either GRAPPA or the variational network for reconstruction were tested using the prospectively acquired data. Resulting T1 maps were evaluated visually and in terms of T1 agreement with results for the vendor sequence.
Results and Discussion
The metric scores achieved by the variational networks are displayed in Figure 1(a) and indicate overall good reconstruction performance.The Bland-Altman plots in Figure 2 show better T1 agreement for using GRAPPA compared to using the variational network for image reconstruction. Nonetheless, the resulting T1 values do not differ significantly from the values produced by the ground truth method, when using either of the evaluated reconstruction methods, cf. Figures 1(b).
Figure 3 shows the mean T1 values across the six midventricular AHA myocardial segments for all evaluated methods. No significant T1 differences between the ground truth method and the evaluated methods were reported, cf. Figure 3(f).
Figures 4 and 5 show T1 maps with increased noise when using GRAPPA to reconstruct higher resolution MOLLI acquisitions. Although using GRAPPA results in good mean T1 agreement (cf. Figure 2), the added noise may be a confounding factor when detecting small focal lesions. When using the variational network, the image quality of the resulting T1 maps is noticeably improved. Additionally, the T1 maps appear sharper when compared to the ground truth T1 maps due to the increased resolution.
Conclusion
A modified variational network was proposed, that when integrated into an existing T1 mapping sequence, allows for the acquisition of higher resolution T1 maps without increasing the scan or breath hold duration. The resulting T1 values show no significant differences compared to a clinically approved T1 mapping sequence. The resulting higher resolution T1 maps may potentially improve the detection of small focal lesions, which will be the subject of future clinical evaluation.Acknowledgements
No acknowledgement found.References
[1] P. Haaf, P. Garg, D. R. Messroghli, D. A. Broadbent, J. P. Greenwood, and S. Plein. Cardiac T1 mapping and extracellular volume (ECV) in clinical practice: a comprehensive review. J Cardiovasc Magn Reson, 18(1):89, 2016.
[2] D. R. Messroghli, A. Radjenovic, S. Kozerke, D. M. Higgins, M. U. Sivananthan, and J. P. Ridgway. Modified Look-Locker inversion recovery (MOLLI) for high-resolution T1 mapping of the heart. Magnetic Resonance in Medicine, 52(1):141–146, 2004.
[3] K. Piechnik et al. Shortened Modified Look-Locker Inversion recovery (ShMOLLI) for clinical myocardial T1-mapping at 1.5 and 3 T within a 9 heartbeat breathhold. Journal of Cardiovascular Magnetic Resonance, 12(1):69, 2010.
[4] M. Doneva et al. Compressed sensing reconstruction for magnetic resonance parameter mapping. Magnetic Resonance in Medicine, 64(4):1114–1120, 2010.
[5] Y. Jun, H. Shin et al. Deep model-based magnetic resonance parameter mapping network (DOPAMINE) for fast T1 mapping using variable flip angle method. Medical Image Analysis, 70:102017, 2021.
[6] A. Sriram, J. Zbontar, T. Murrell, A. Defazio, C. L. Zitnick, N. Yakubova, F. Knoll, and P. Johnson. End-to-end variational networks for accelerated MRI reconstruction. In Medical Image Computing and Computer Assisted Intervention – MICCAI 2020, pages 64–73, 2020.
[7] M. Vornehm, J. Wetzl, D. Giese, R. Ahmad, and F. Knoll. Spatiotemporal variationalneural network for reconstruction of highly accelerated cardiac cine MRI. European Heart Journal - Cardiovascular Imaging, 23(Supplement_2):jeac141–018, 2022
[8] M. Vornehm, J. Wetzl, D. Giese, and F. Knoll. K-t Adaptive Regularization in Variational Networks for Cardiac Cine Reconstruction. In Proceedings of the ISMRM Workshop on Data Sampling & Image Reconstruction (Sedona, AZ), 2023
[9] N. J. Tustison et al., N4ITK: Improved N3 Bias Correction. In IEEE Transactions on Medical Imaging, vol. 29, no. 6, pp. 1310-1320, 2010
[10] M. A. Griswold, P. M. Jakob, R. M. Heidemann, M. Nittka, V. Jellus, J. Wang, B. Kiefer, and A. Haase. Generalized autocalibrating partially parallel acquisitions (GRAPPA). Magnetic Resonance in Medicine, 47(6):1202–1210, 2002
[11] Chow K, Kellman P, Xue H. Prototyping Image Reconstruction and Analysis with FIRE. In Proc SCMR Virtual Scientific Sessions 2021. p. 838972
Figures
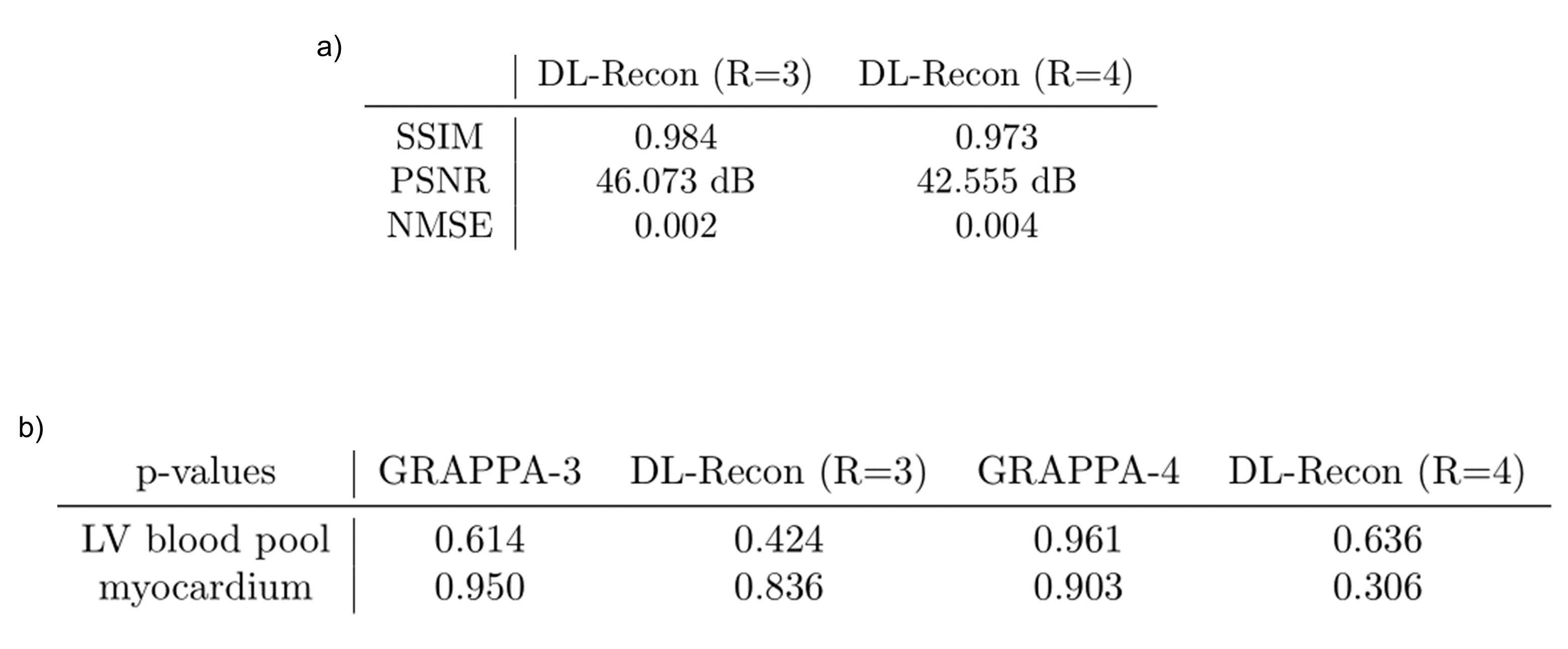
Figure 1: (a) SSIM, PSNR and NMSE scores achieved by the modified variational networks when compared to the ground truth test data in terms on reconstruction quality. Acceleration rates of 3 and 4 were used during training and testing. (b) P-values for a two-sided students t-test reflecting the significance of the T1 differences when comparing the evaluated methods to the ground truth. Values above the significance level of 0.05 indicate a non-significant difference. The comparison was conducted using the prospectively collected, higher spatial resolution MOLLI acquisitions.
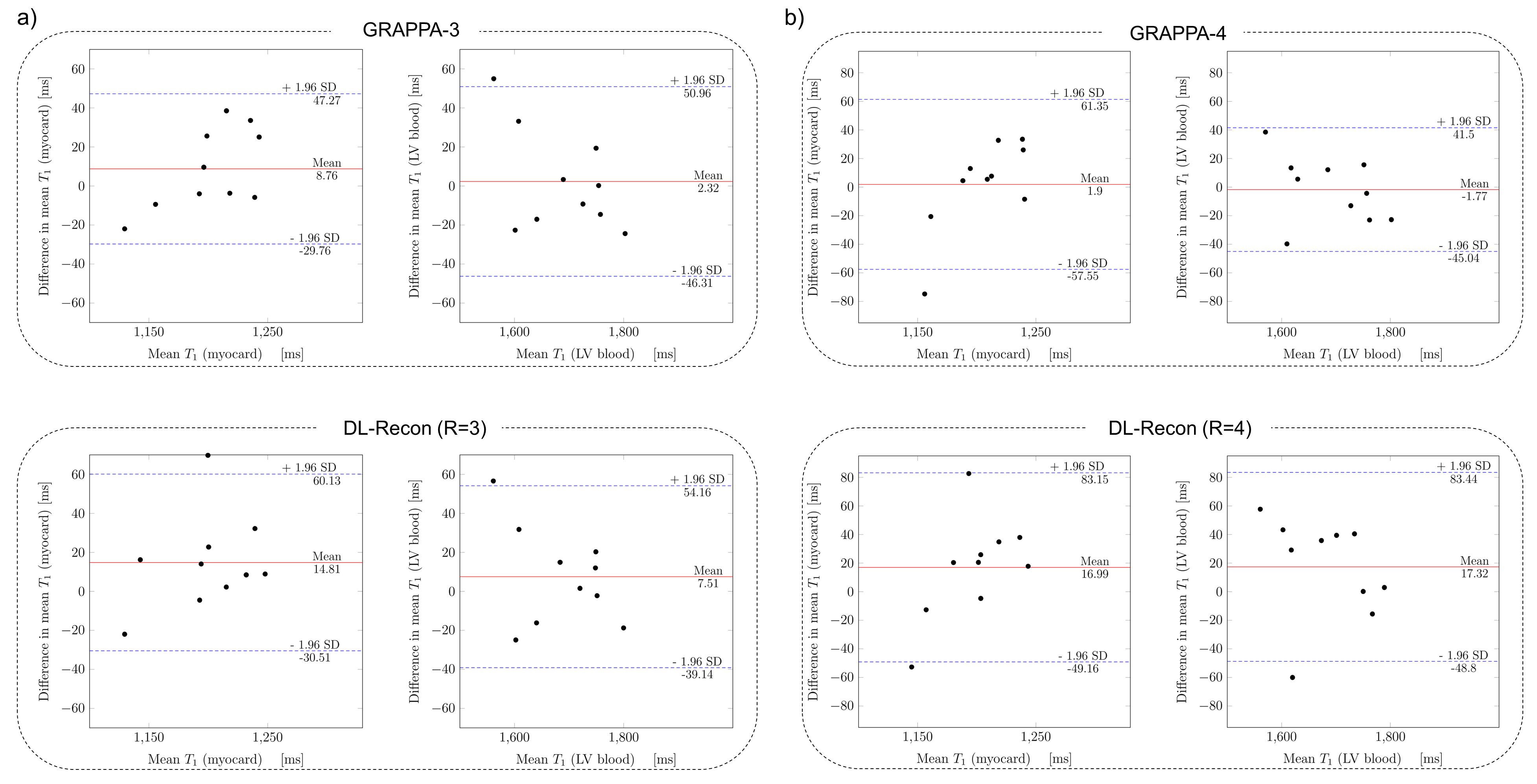
Figure 2: Bland-Altman plots showing the T1 agreement with the vendor sequence when using GRAPPA and the variational network (DL-Recon) within the modified T1 mapping sequence. Acceleration factors of 3 and 4 were used. Mean T1 values were compared in the regions of the myocardium and the left ventricular blood pool. The mean T1 difference is shown as a red line and the corresponding limits of agreement are displayed as dotted blue lines. Note that T1 differences are potentially amplified as the analyzed values correspond to independent acquisitions of the same subject.
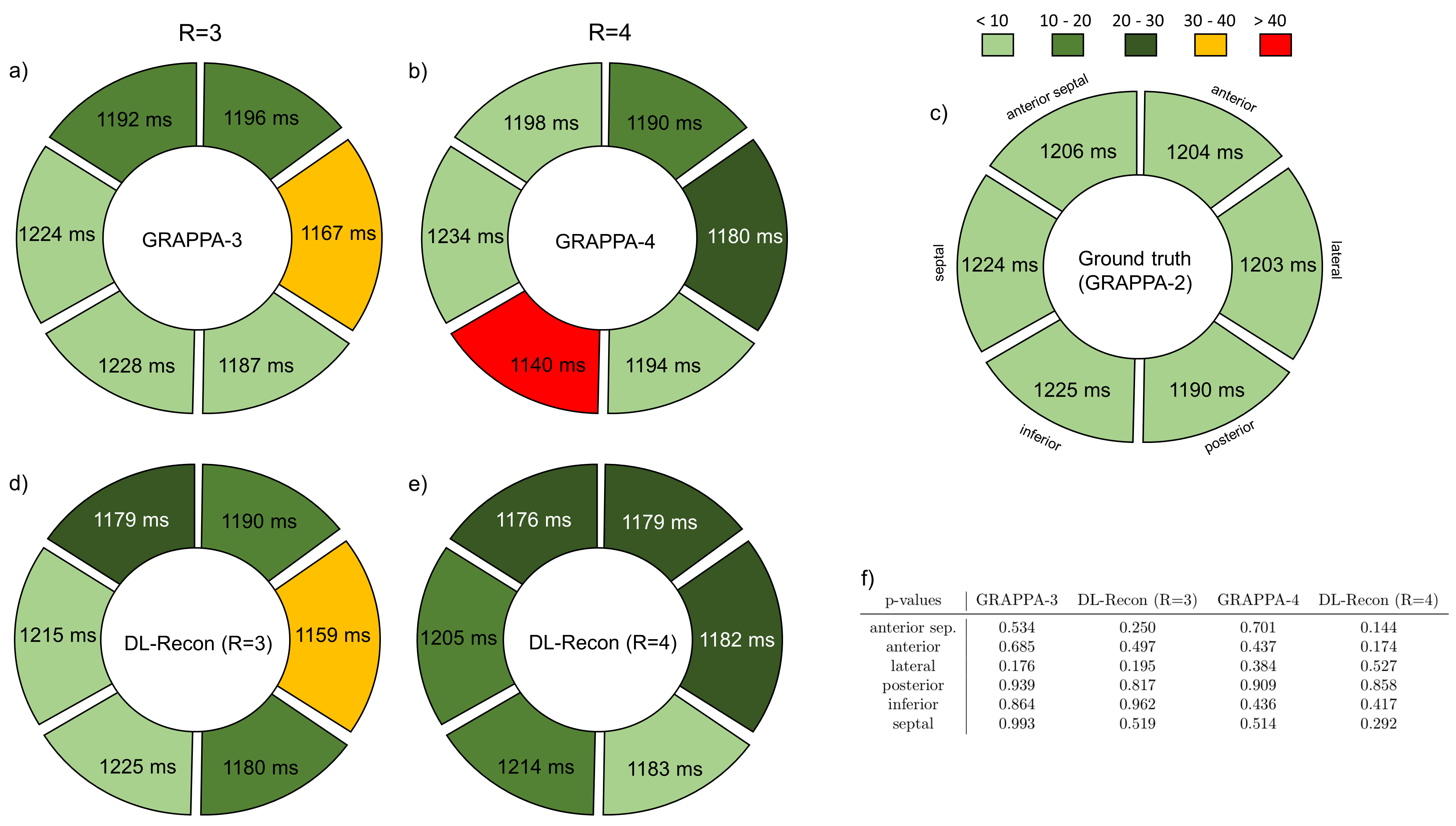
Figure 3: (a) - (e) Mean T1 values in the mid myocardial segments for the ground truth T1 maps and T1 maps computed by using GRAPPA or the variational network (DL-Recon) within the modified T1 mapping sequences for acceleration rates 3 and 4. Mean T1 differences between the ground truth and the evaluated methods are illustrated using the displayed color scheme. (f) P-values for a two-sided students t-test reflecting the significance of the T1 differences across the myocardial segments when comparing the evaluated methods to the ground truth. A significance level of 0.05 was used.
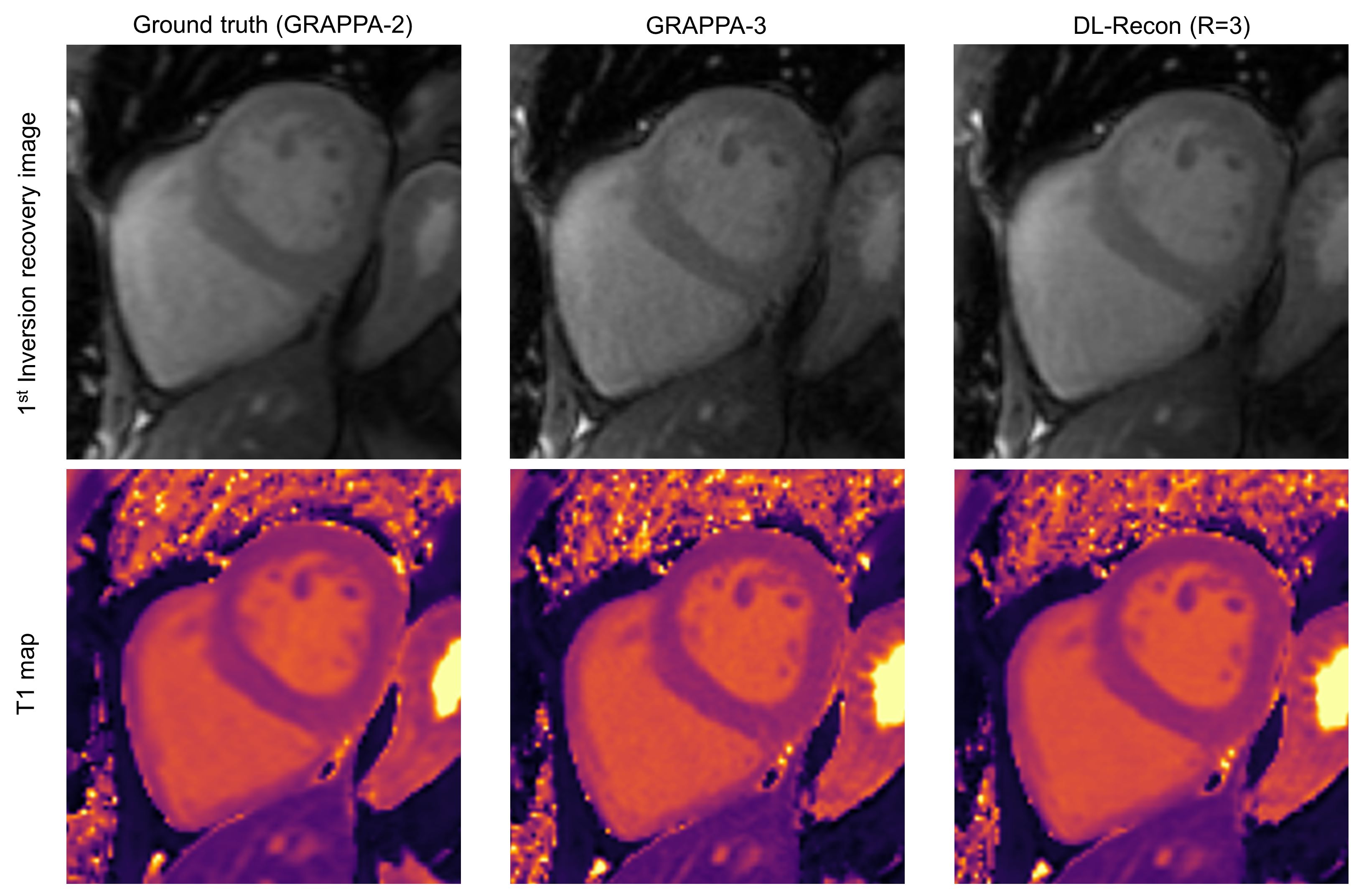
Figure 4: Example reconstructions of the first inversion recovery image from the MOLLI image set and the corresponding T1 maps. Results for the vendor sequence are shown in the left column. Results for using GRAPPA within the modified T1 mapping sequence for an acceleration factor of 3 are shown in the middle column. Results for using the variational network (DL-Recon) within the modified T1 mapping sequence for an acceleration factor of 3 are shown in the right column. The MOLLI image sets for the results shown in the middle and in the right column were acquired in higher resolution.
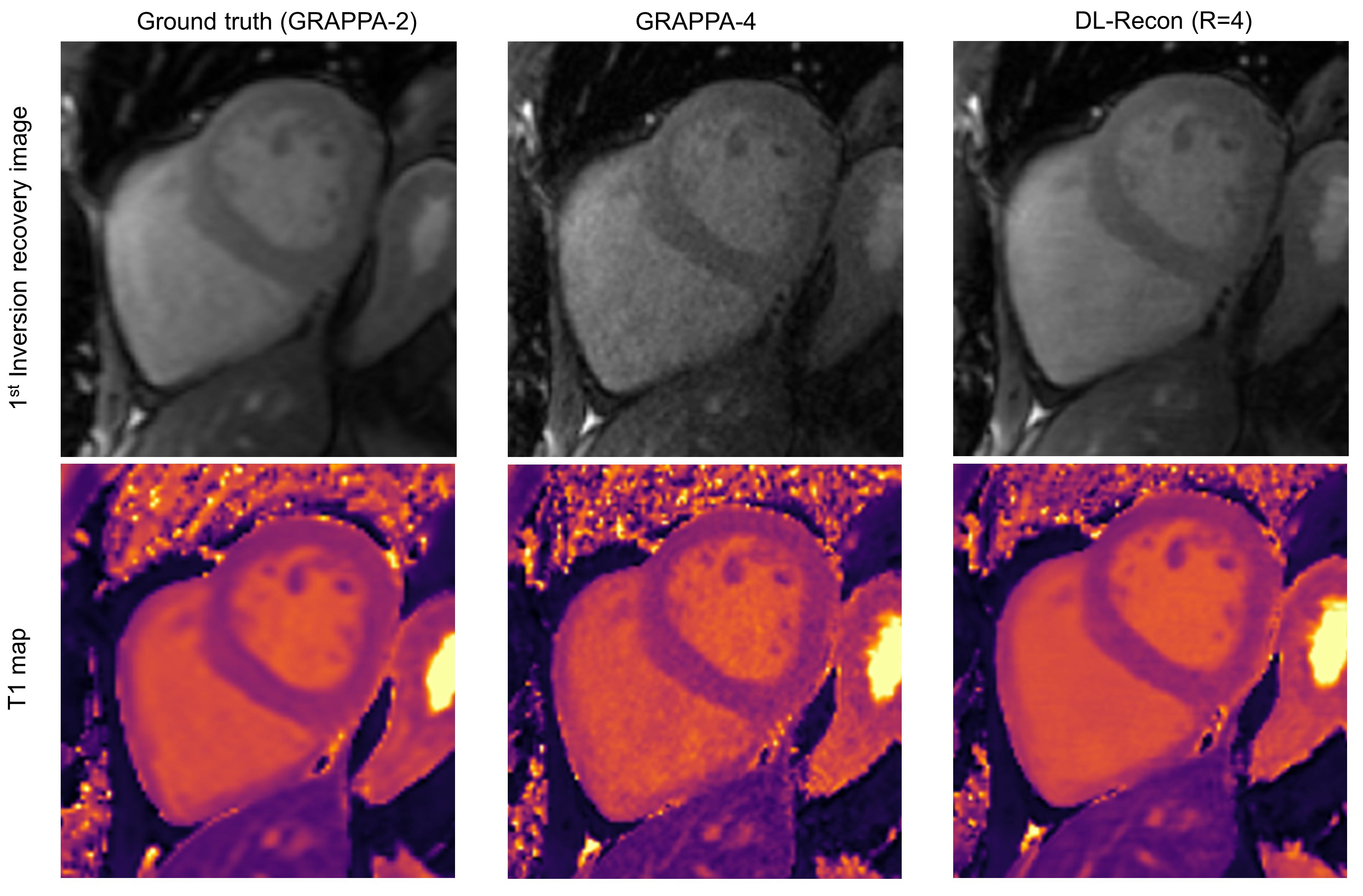
Figure 5: Example reconstructions of the first inversion recovery image from the MOLLI image set and the corresponding T1 maps. Results for the vendor sequence are shown in the left column. Results for using GRAPPA within the modified T1 mapping sequence for an acceleration factor of 4 are shown in the middle column. Results for using the variational network (DL-Recon) within the modified T1 mapping sequence for an acceleration factor of 4 are shown in the right column. The MOLLI image sets for the results shown in the middle and in the right column were acquired in higher resolution.