4658
Accuracy requirements for an automated deep-learning-based slice prescription for cardiac MRI1GE Healthcare, Munich, Germany, 2GE Healthcare, Barcelona, Spain
Synopsis
Keywords: Acquisition Methods, Machine Learning/Artificial Intelligence, Automated plane prescription, workflow
Motivation: Automated plane prescription tools can make cardiac MRI more accessible, but their accuracy needs to be validated.
Goal(s): We aim to determine the accuracy requirements for an AI-driven automated prescription tool.
Approach: To determine the accuracy requirements for an AI-driven automated prescription tool we compare landmarks set by the tools to those set manually by operators with different levels of experience.
Results: The prototype can match the average performance of an operator group, outperforming the less experienced individuals.
Impact: To be reliable the performance of automated prescription tools needs to be established. Here an AI-driven automated prescription tool for cardiac MRI planes could match the average performance of an operator group, outperforming the less experienced individuals.
Background
A cardiac MR (cMR) exam relies on the radiographers prescribing double oblique cardiac planes while monitoring the patient’s wellbeing during a long exam with breathing manoeuvres. This requires a high level of training and expertise which limits availability of cMR. A tool for automated plane prescription could make cardiac imaging more widely accessible. Higher automatization can reduce exam time, ensure overall better image quality and a higher level of reproducibility. To achieve these goals the quality and stability of the tool’s results need to be ensured.The goal of this study was to determine the accuracy requirements for an AI-driven automated prescription tool called SaxLocNet, by comparing its performance to a cohort of operators with different levels of cMR expertise.
Methods
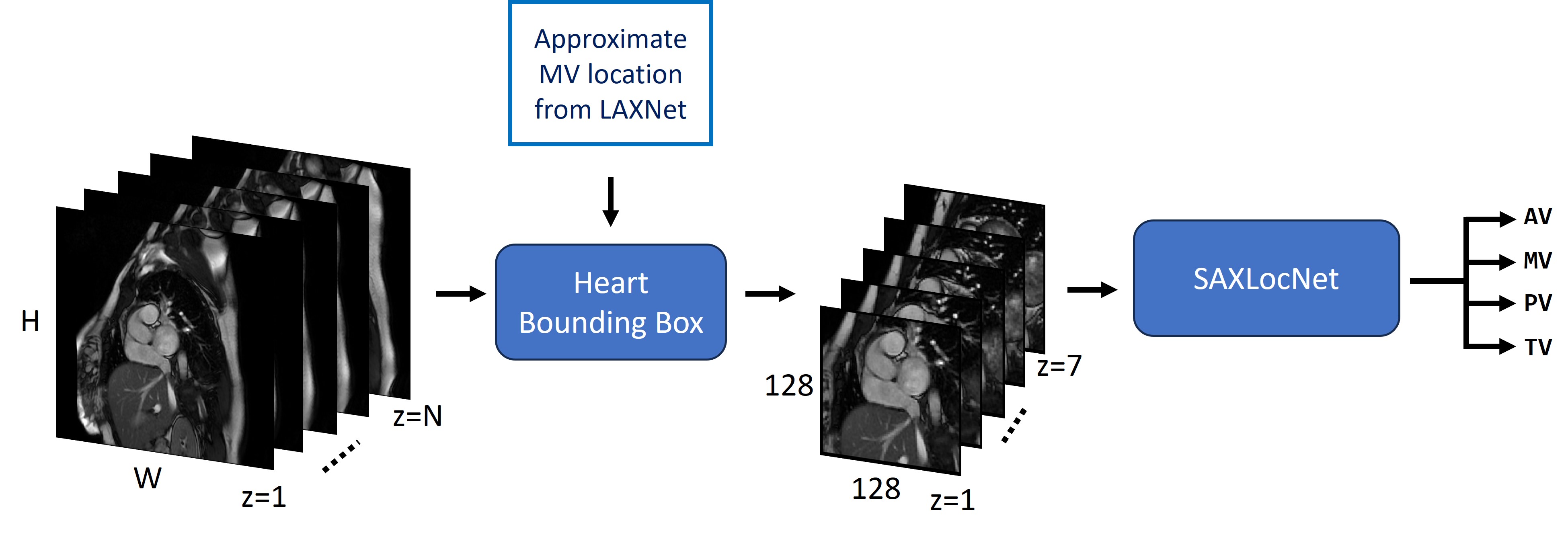
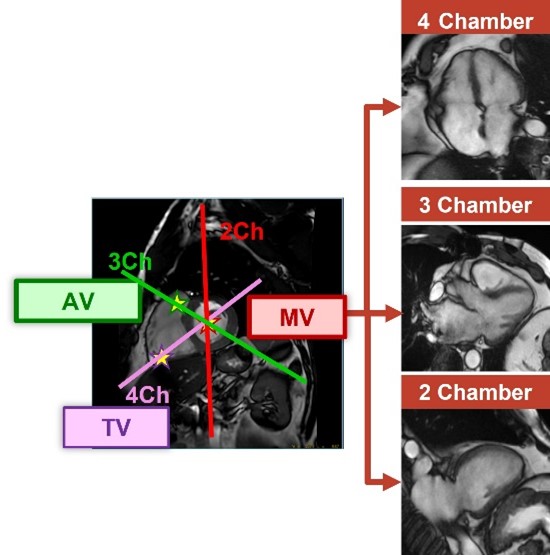
Automated localization of cardiac landmarks:A prototype convolutional neural network (CNN) was trained to prescribe 2-, 3- and 4-chamber views on bSSFP short axis stack (SAX) cine images [1, 2]. The prescription is based on the automatic localization of the aortic, mitral, pulmonary, and tricuspid valves on the SAX. A separate deep learning CNN (SAXLocNet) adapted to a multi-task UNet architecture is employed to predict locations of the four valves. This network takes an approximate mitral valve location from the previous stage of pseudo-long axis (LAX) processing to reduce the localization search space by creating a bounding box around the heart. The four valves are then localized within the reduced search space, see figure 1. The long axis views are determined based on the localized valve locations, see figure 2.
Performance evaluation:
In this study the landmarks identified by the prototype were compared to those manually defined by 12 operators with varying levels of CMR expertise [1-22 years]. Randomly selected standard cardiac morphology 2D SAX images from 9 adult patients from 1.5 and 3.0T GE HealthCare scanners (SIGNA Artist, Architect, Premier, MR450w) from three different sites were used for this comparison. The ground truth valve locations were calculated as the median of the landmarks manually set by all operators. The distances to these ground truth locations were calculated for each operator and compared to those generated by the automated prototype.
Results
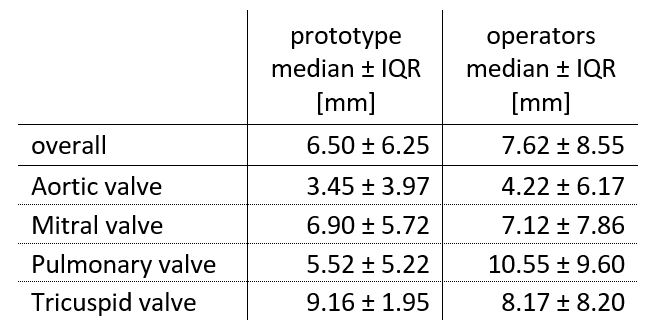
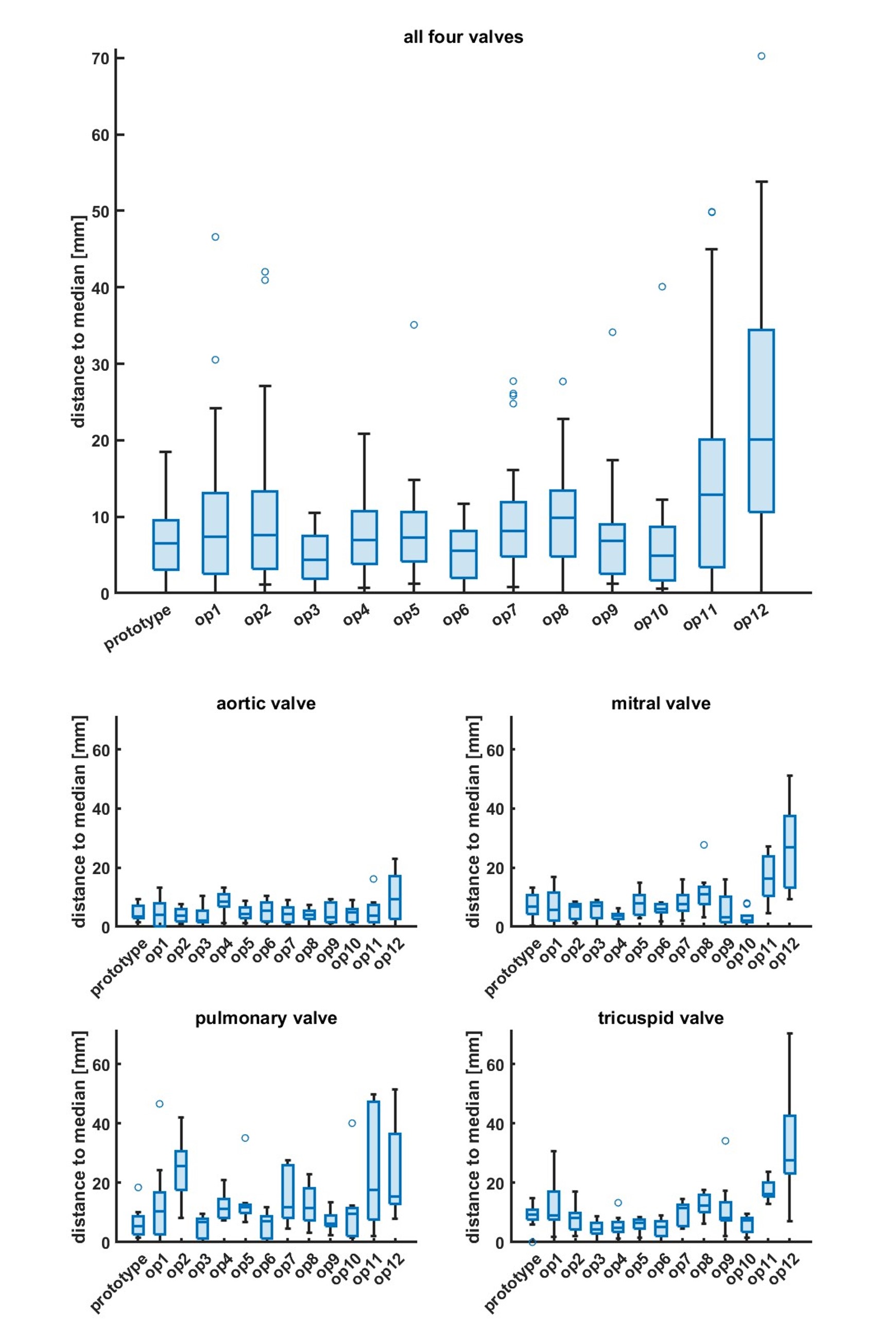
The processing was completed successfully for all available data sets. The distances to the ground truth for all four valves are shown in table 1. The range of IQR values obtained by the prototype is smaller compared to the range of the human operators indicating a more stable performance on all valves. Three out of 12 operators showed a better performance than the prototype, two of them being operators with most cMR experience (>13 years). Figure 3 shows the results over all valves by operator as well as the results by operator and valve. While the aortic and mitral valves were well recognised by both the model and the operators, the pulmonary valve was difficult for both. Nevertheless, the module presents a more stable behaviour in the latter case. It should be noted that an operator would not rely only on a SAX to localize this valve. In this study we only tried to define a realistic performance target for the model.Conclusion
The prototype can match the average performance of an operator group, outperforming the less experienced individuals. These results demonstrate that the prototype can effectively assist non-expert radiographers in performing a diagnostic exam, thereby increasing access to cMR.Acknowledgements
Big thanks to Michael Vinsky, Junjie Ma, Fara Nikbeh, Mary Thomas, Ana B Solana, Haonan Wang, Pingni Wang, Patrick Quarterman, Eman Ali and Martina Hoertemoeller for contributing to this abstract.References
1. Blansit, K. et al. “Generalizability and Robustness of an Automated Deep Learning System for Cardiac MRI Plane Prescription”, abstract #2661, ISMRM 2021
2. Blansit, Kevin, et al. "Deep learning–based prescription of cardiac MRI planes." Radiology: Artificial Intelligence 1.6 (2019): e180069.
Figures