4656
Patient adaptive intelligent MRI scanning with consistent Image Quality1GE HealthCare, Bangalore, India, 2GE HealthCare, Waukesha, WI, United States
Synopsis
Keywords: Acquisition Methods, Signal Representations, Workflow, Reproducibility
Motivation: Adapt the MR imaging for patient specific anatomical coverage.
Goal(s): Adapt MRI protocol while maintaining contrast, SNR and scan time in patient specific MR imaging.
Approach: The Intelligent slice placement estimated the brain segmentation and key landmarks for determining imaging volume center, orientation and coverage. The MRI protocol is then adjusted to demonstrate that contrast, SNR and scan time can be maintained within limits.
Results: The MRI images with patient adaptive MR imaging have similar view and coverage of anatomy while contrast, SNR and scan time is maintained.
Impact: MRI protocol adaption (while maintaining contrast, SNR and scan time within limits) demonstrated in this abstract along with anatomical coverage for patient adaptive scanning is essential for consistent high quality MRI imaging within and across clinical sites.
INTRODUCTION
MRI require continuous update to anatomical coverage and orientation. Changes to these often leads to change in contrast, SNR and scan time which can severely impact the clinical usability (leading to reorder) and patient comfort. There are several MRI protocol parameters such as matrix size, and averages which can be adjusted to maintain the contrast, SNR and scan time within reasonable limits. The intricate relationship between these parameters and their impact on the contrast, SNR and scan time limits the patient adaptive MR imaging in the clinical practice leading to fewer number of slices and/or too large FOV.Several research and commercial techniques have been proposed to estimate anatomical coverage and imaging volume planning [1,2]. AI based intelligent slice placement (ISP) method provides consistent imaging center and orientation for multiple landmarks[1,2]. AI based anatomical coverage methods estimate number of slices to cover the anatomy of interest. However, these methods rely on the expertise of the MR technologist to ensure desired contrast is maintained with expected SNR in similar scan times. In this abstract, we demonstrate a methodology for patient adaptive iantelligent MRI (PAiMRI) scanning for 2D brain MRI which utilizes ISP for setting up the imaging center and orientation, uses information about landmark extents from ISP to setup anatomical coverage, while using MRI physics relationships to ensure that desired contrast, SNR and scan time is maintained within a user specified limit.
METHODS
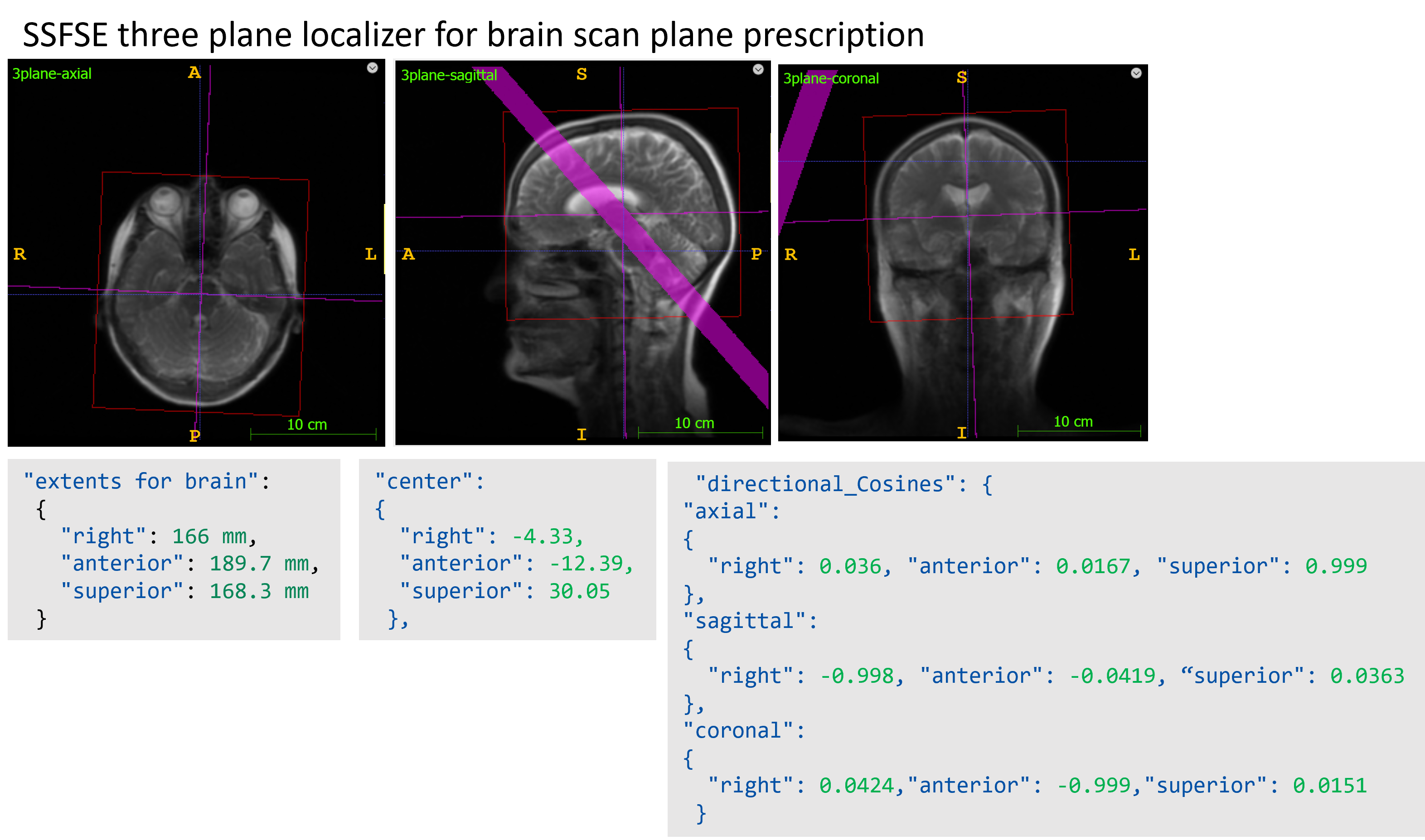
The proposed method for PAiMRI consists of two steps,- Imaging volume planning: Intelligent slice placement (ISP) [2] provide whole brain segmentation and key landmarks which are then utilized for determining the imaging plane orientation and center depending on the imaging plane and anatomy of interest such as whole brain axial Talairach AC-PC based planning. The segmentation of brain and landmarks are used to determine the FOV extents in the readout and phase encoding direction. Number of slices and slice thickness/spacing is adjusted based on the extend in the slice direction.
- MRI Protocol optimization: The changes in the anatomical coverage can induce change in contrast (increased TR in 2D T1w FSE), SNR (change in voxel size) and scan time (increase in number of acquisitions in 2D FLAIR imaging). MRI protocol dependent SNR was determined using [3],
Where, $$$\delta_r, \delta_p and \delta_s$$$ corresponds to voxel size in readout, voxel size in phase-encoding and slice thickness, respectively. $$$N_{ex}$$$ refers to all the averaging including oversampling in phase direction. $$$N_r$$$ and $$$N_p$$$ correspond to imaging matrix size in readout and phase encoding directions, respectively. $$$ R_{BW}$$$ corresponds to receiver bandwidth and $$$R_{fast}$$$ corresponds to net acceleration due to all fast imaging techniques including partial Fourier, parallel imaging and compressed sensing. The contrast in kept similar by maintaining TE, TR (for T1w) and Inversion times. Patient adaptive MRI protocol optimization involved optimizing the protocol (including but not limited to matrix size, ETL for FSE, averages and acceleration) to obtain same voxel size with similar SNR and scan times.
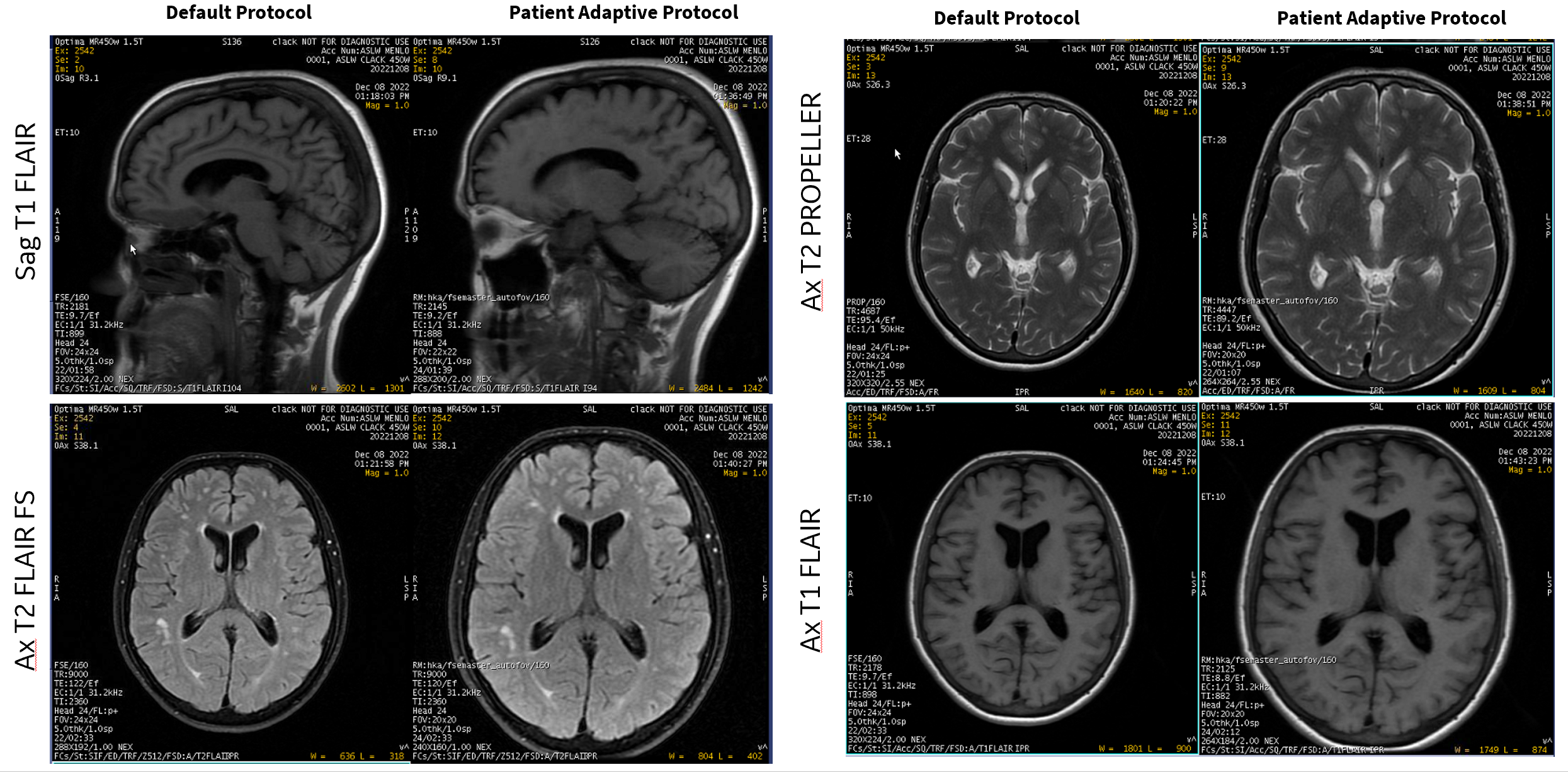
A volunteer was scanned in an IRB approved study with informed consent at a commercial 1.5T MRI scanner using the default site brain protocol having multiple 2D acquisitions (Sagittal-T1w-FSE-FLAIR, Axial-T2w-PROPELLER, Axial-T2w-FLAIR-Fat-Sat and Axial-T1w-FLAIR). These acquisition were then repeated with PAiMRI. The site MRI protocol and the PAiMRI protocol parameters are shown in Table 1.
RESULTS
Figure 1 shows the output of ISP on three-plane localizer MR images of brain for a volunteer with brain extent smaller (166-189.3mm) than baseline FOV of 240 mm suggesting changes in anatomical extent.Figure 2 demonstrates baseline and PAiMRI. MRI images with PAiMRI have full anatomical coverage with similar SNR and contrast. Table 1 shows that except for Axial T2 FLAIR, scan time has reduced for other protocols (gain of ~ 10-20% from baseline protocol). This is primarily achieved by adjusting the Matrix size to match the voxel size, while ensuring that SNR is always > 80% of the baseline protocol.
DISCUSSION AND CONCLUSION
PAiMRI is demonstrated with an automated framework to utilize the ISP for consistent scan planes and utilize it to auto-prescribe the FOV and coverage for patient anatomy size. This is coupled to a MR physics engine which ensures that adapting to patient size maintains contrast, SNR and scan time to a pre-configured tolerance limits. The feasibility of PAiMRI in this abstract warrants additional studies to show reduced dependence of MRI on technologist expertise and automated scan time reduction due to lower SNR threshold due to the use of AI based image enhancement methods [4].Acknowledgements
No acknowledgement found.References
- Alansary, Amir et.al;, Daniel. (2018). “Automatic View Planning with Multi-scale Deep Reinforcement Learning Agents”. MICCAI 2018, pp.277-285.
- Shanbhag DD et.al, “A generalized deep learning framework for multi-landmark intelligent slice placement using standard tri-planar 2D localizers”, ISMRM 2019, p.670
- Dwight G. Nishimura, “Principles of Magnetic Resonance Imaging”, 1996, 223 pages, Chapter 7.
- Lebel, Marc, “ Performance characterization of a novel deep learning-based MR image reconstruction pipeline”, arXiv:2008.06559 [eess.IV].
Figures