4651
Comparison of Motion Correction Schemes for Cardiac Diffusion Tensor Imaging Using Image Registration1Siemens Medical Solutions USA, Inc., Cleveland, OH, United States, 2Cardiovascular Innovation Research Center, Heart Vascular Thoracic Institute, Cleveland Clinic, Cleveland, OH, United States, 3Siemens Medical Solutions USA, Inc., Columbus, OH, United States, 4Siemens Healthcare, Erlangen, Germany, 5Cardiovascular Medicine, Heart Vascular Thoracic Institute, Cleveland Clinic, Cleveland, OH, United States, 6Imaging Institute, Cleveland Clinic, Cleveland, OH, United States, 7Siemens Medical Solutions USA, Inc., Los Angeles, CA, United States, 8Department of Biomedical Engineering, Case Western Reserve University & Cleveland Clinic, Cleveland, OH, United States
Synopsis
Keywords: Motion Correction, Motion Correction
Motivation: Motion correction (MOCO) is critical for free-breathing cardiac DTI, but it is challenging due to low SNR and variations in b-value contrast in acquired images.
Goal(s): To compare MOCO schemes for cardiac DTI with the ultimate goal of implementing the entire post-processing workflow inline on the scanner.
Approach: Three image registration-based MOCO schemes were compared with a previous low rank tensor (LRT) method in 7 volunteers.
Results: Compared with the LRT method, proposed MOCO methods achieved smaller standard deviations of MD and FA values, more smoothly varying helical structure in HA maps, and visually less motion of the heart in diffusion weighted images.
Impact: A robust and fast motion correction approach for free-breathing cardiac diffusion tensor imaging (DTI) improves the quality of diffusion maps, and facilitates clinical translation of cardiac DTI.
Introduction
Cardiac diffusion tensor imaging (DTI) provides a non-invasive tool to detect microstructure in the heart. Previously proposed second-order motion compensating (M2) diffusion gradients enable robust spin-echo based diffusion acquisition in the heart1. However, motion correction (MOCO) is challenging due to low SNR and variations in b-value contrast in acquired images. A low-rank tensor (LRT) model has been proposed to correct respiratory motion for cardiac DTI data by regressing out b-value contrast before image registration2. Alternatively, pair-wise image registration method has been successfully used for CMR applications such as perfusion, T1 mapping, free-breathing phase sensitive inversion recovery (PSIR), etc3-5. This study aims to apply such image registration method to cardiac DTI data acquired on a 3T MR system (MAGNETOM Cima.X, Siemens Healthineers AG, Erlangen, Germany) with Gmax of 200mT/m. Shorter TE enabled by the high gradient amplitude improves SNR of the diffusion weighted images, which alleviates the challenges of image registration.Methods
Human data acquisition:A research sequence employing M2 diffusion gradients and single-shot EPI readout was performed in 7 healthy subjects under an IRB approved protocol on a 3T MR system (MAGNETOM Cima.X, Siemens Healthineers AG, Erlangen, Germany). TE of 59ms was achieved benefiting from the maximum gradient strength of 200mT/m. Other acquisition parameters are: FOV 350mm × 131mm, Zoomit with 2D RF pulse, matrix size 128 × 48, slice thickness 8mm, 5 slices, TR 500 ms, 12 diffusion directions, 1 average for b0 (b=50 s/mm2), 8 averages for b=500 s/mm2. All images were acquired at end systole with ECG triggering under free-beathing in <5min.
Motion correction schemes:
Three MOCO schemes using pair-wise non-rigid image registration6 were compared against the previous LRT based multitasking approach. The first method (MOCO_naive) registered all individual diffusion weighted images to the first acquired b0 image. The second method (MOCO_avg) registered all 12 b0 images to the first acquired image to form a relatively high SNR reference image. Individual b=500 s/mm2 images were registered to the above reference image followed by averaging for each diffusion direction. Then averaged b=500 s/mm2 images were registered to the reference image again. On top of MOCO_avg, the third method (MOCO_avg_out) threw away 10% outliers before averaging b=500 s/mm2 images. Outliers were defined as the top 10% images (10 images in this study) with largest deformation in the heart region. All three MOCO schemes were performed in MATLAB (Mathworks, 2023a).
Data analysis:
Mean diffusivity (MD), fractional anisotropy (FA), and helix angle (HA) maps were generated using a custom built, Python-based DTI processing library. Mean and standard deviation of MD, FA, and helix angle transmurality (HAT) maps for each slice and for global were calculated by manually segmenting the left ventricle. A paired t-test was performed for comparisons between different MOCO methods and statistically significant difference was reported at p<0.05.
Results
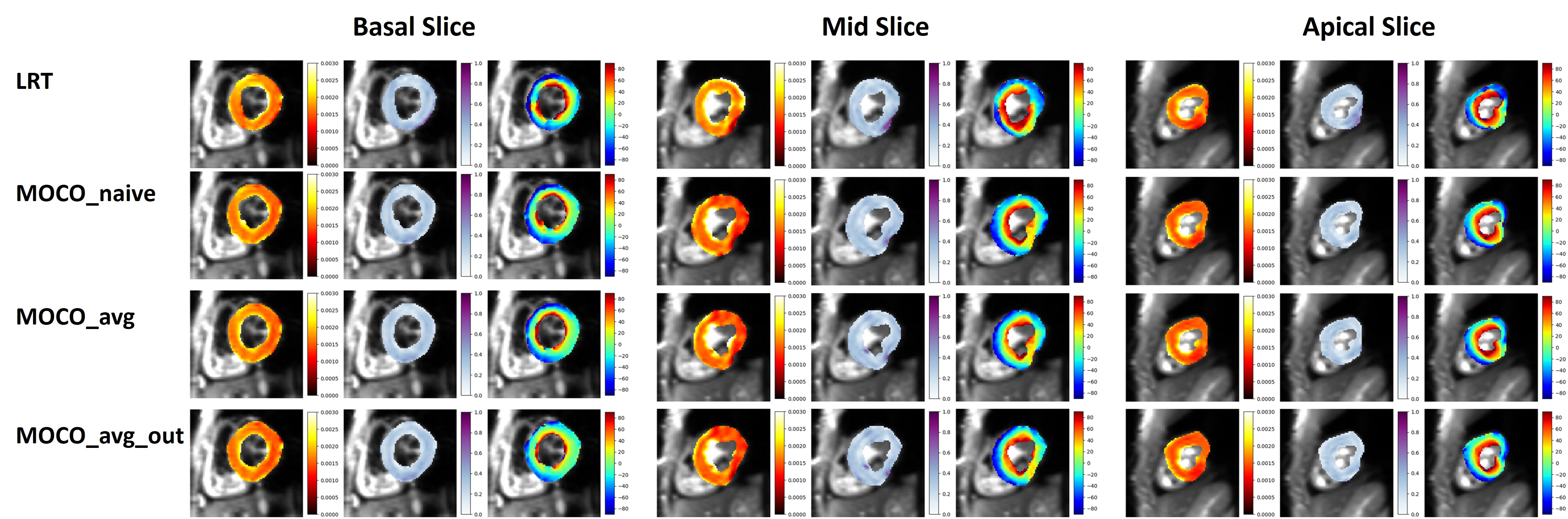
Figure 1 shows animated diffusion weighted images of 5 slices in one subject before MOCO and using different MOCO methods. The proposed three MOCO methods all yield visually more stable heart in the images. Figure 2 shows comparison of mean value of MD, FA, and HAT. Compared with the LRT method, proposed MOCO schemes yield similar MD values except in slice2 where significant difference is observed for MOCO_naive and MOCO_avg_out; similar HAT values except in slice5; and overall decreased FA values with significant difference in slice3, slice5, and global. Standard deviations of MD and FA are overall reduced in proposed methods compared with the LRT method (Figure 3). HA maps of all 5 slices and MD, FA, HA maps of the base, mid, apex slices in one subject are shown in Figure 4 and Figure 5, respectively. More smoothly varying helical structure is observed in the HA maps generated by proposed MOCO methods.Discussion & Conclusions
This study shows the feasibility of image registration-based MOCO for cardiac DTI images acquired on Cima.X without the need to regress out b-value contrast. It benefits from higher SNR and contrast stability enabled by ultra-high gradient performance of Cima.X. Its feasibility for data acquired on other systems with lower gradient performance needs further investigation. All three proposed schemes are more robust than the LRT method reflected by visually less motion of the heart in diffusion weighted images, visually smoother helical structure in HA maps, as well as smaller variation in the MD and FA values. Interestingly, MOCO_avg and MOCO_avg_out yielded similar results, possibly because MOCO_avg already achieved satisfactory motion correction and keeping all images is more beneficial to gain SNR. Therefore, MOCO_avg is considered the most effective MOCO method in this study. MOCO_avg and MOCO_avg_out need to be further evaluated in patient cohorts to determine if it is necessary to throw away outliers for patient data. The ultimate goal is to implement the MOCO scheme inline to enable fast post-processing and convenient diffusion maps visualization on the scanner.Acknowledgements
No acknowledgement found.References
1. Nguyen C, Fan Z, Xie Y, Pang J, Speier P, Bi X, et al. In vivo diffusion-tensor MRI of the human heart on a 3 tesla clinical scanner: An optimized second order (M2) motion compensated diffusion-preparation approach: Optimized in vivo M2 DT-CMR for a 3T clinical scanner. Magn Reson Med. 2016 Nov;76(5):1354–63.
2. Nguyen CT, Christodoulou AG, Coll‐Font J, Ma S, Xie Y, Reese TG, et al. Free‐breathing diffusion tensor MRI of the whole left ventricle using second‐order motion compensation and multitasking respiratory motion correction. Magn Reson Med. 2021 May;85(5):2634–48.
3. Xue H, Zuehlsdorff S, Kellman P, Arai A, Nielles-Vallespin S, Chefdhotel C, Lorenz C, Guehring J. Unsupervised inline analysis of cardiac perfusion MRI. Lecture Notes Comput Sci 2009;5763:741–749.
4. Xue H, Shah S, Greiser A, Guetter C, Littmann A, Jolly MP, Arai AE, Zuehlsdorff S, Guehring J, Kellman P. Motion correction for myocardial T1 mapping using image registration with synthetic image estimation. Magn Reson Med. 2012 Jun;67(6):1644-55. doi: 10.1002/mrm.23153. Epub 2011 Aug 29. PMID: 22135227; PMCID: PMC4158317.
5. Kellman P, Xue H, Chow K, Howard J, Chacko L, Cole G, Fontana M. Bright-blood and dark-blood phase sensitive inversion recovery late gadolinium enhancement and T1 and T2 maps in a single free-breathing scan: an all-in-one approach. J Cardiovasc Magn Reson. 2021 Nov 8;23(1):126. doi: 10.1186/s12968-021-00823-3. PMID: 34743718; PMCID: PMC8573877.
6. Guetter C, Xue H, Chefd’hotel C, Guehring J. Efficient symmetric and inverse-consistent deformable registration through interleaved optimization. In: Proc. IEEE Int. Symp. Biomed. Imag. 2011, p. 590–3.
Figures
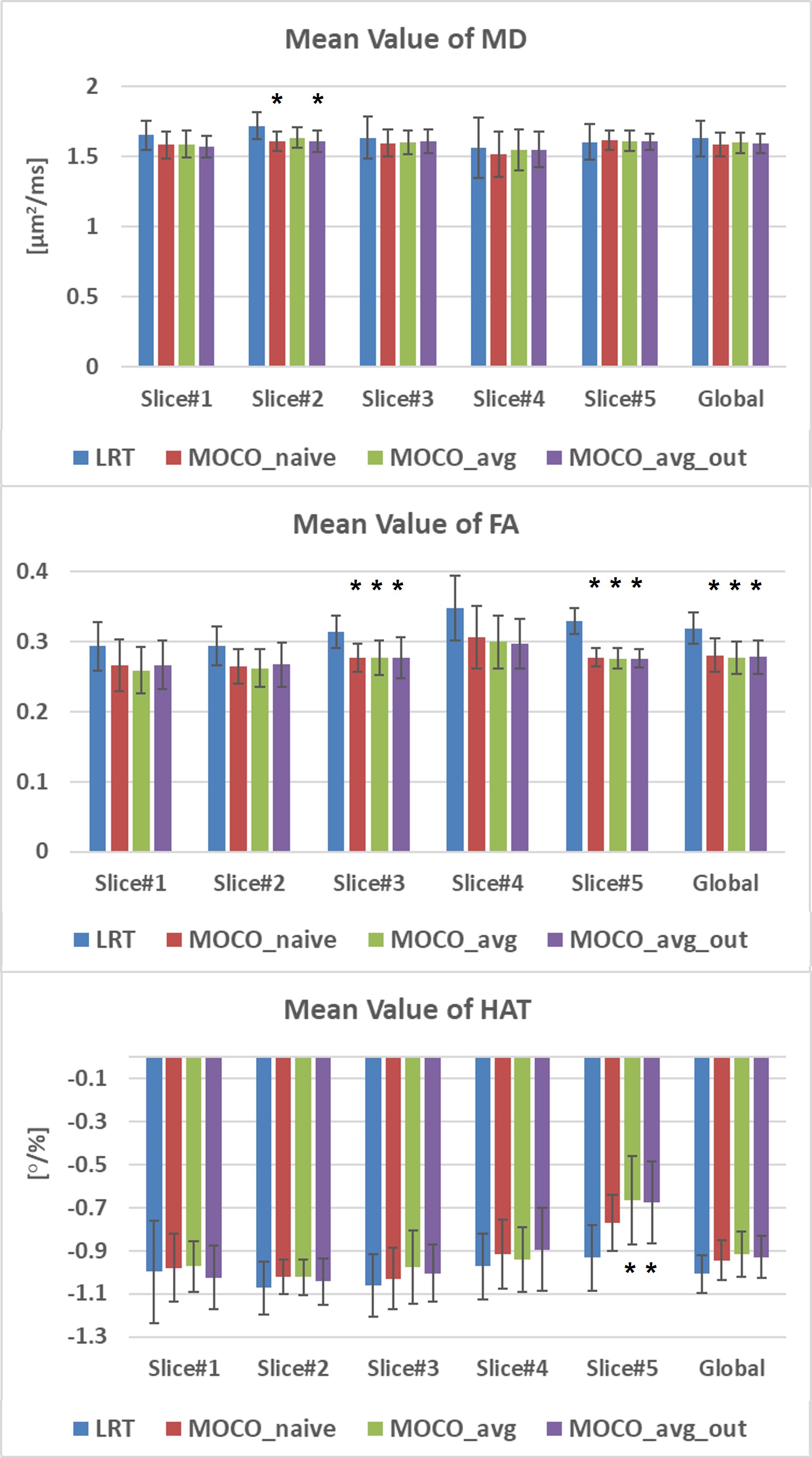
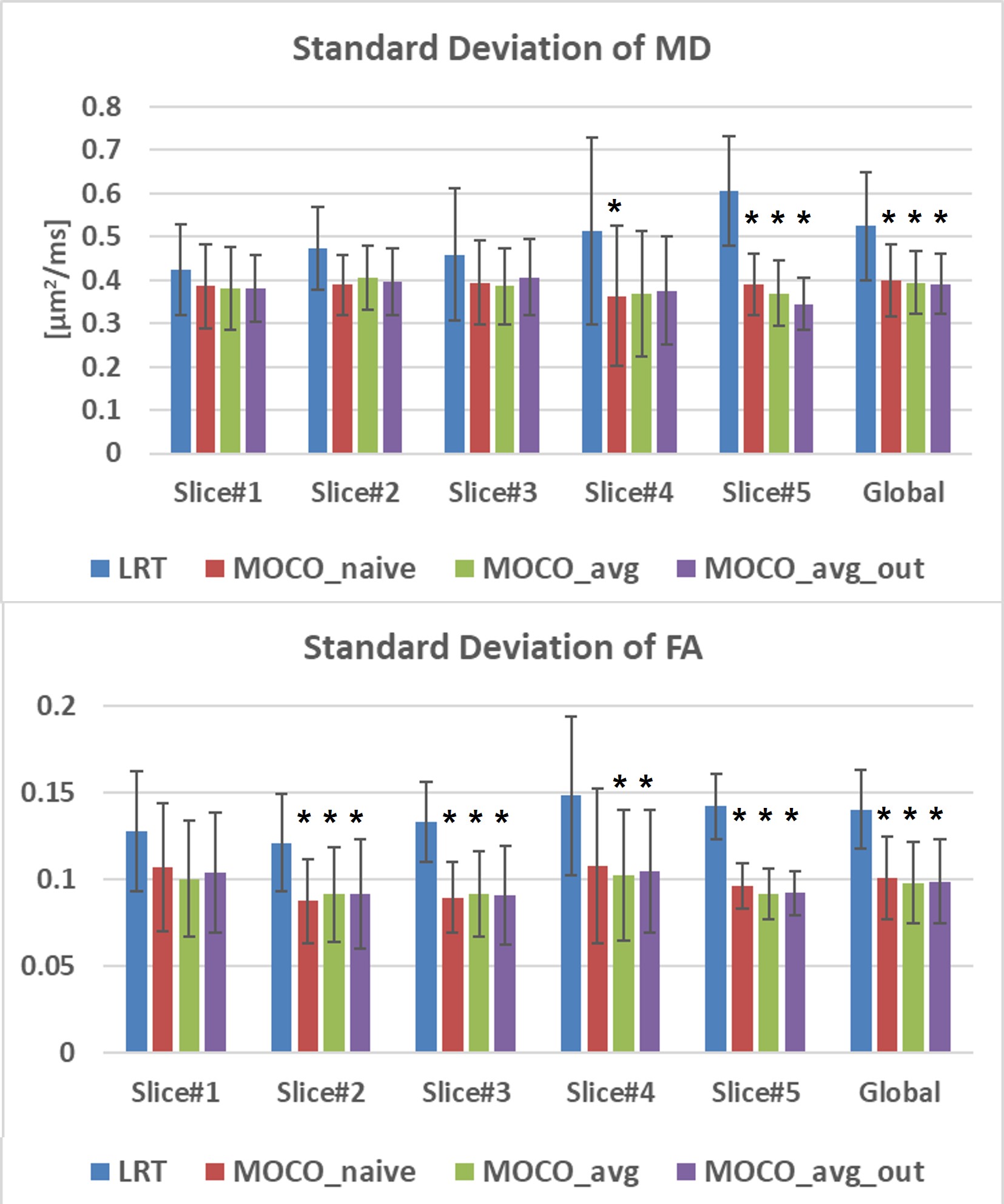
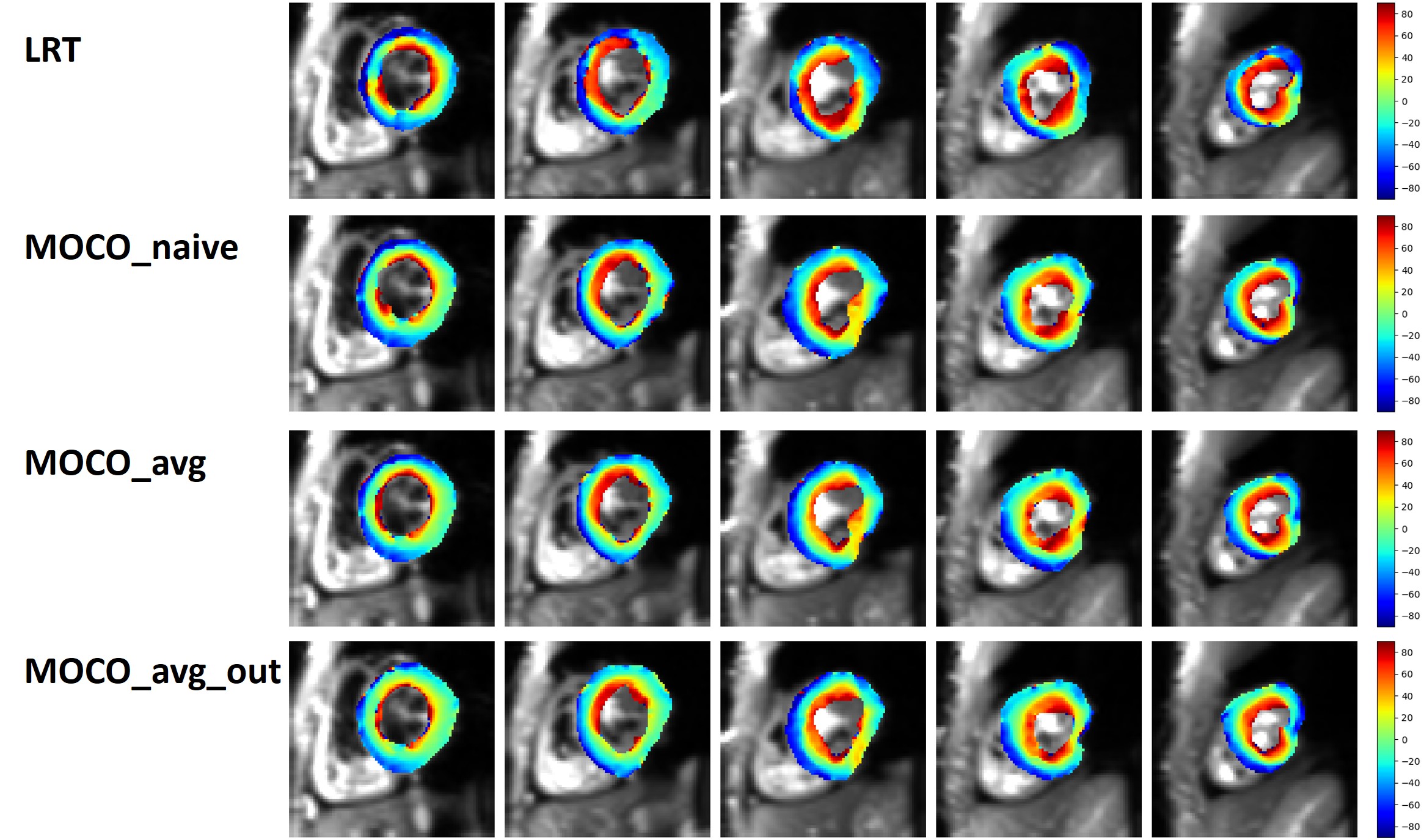
Figure 4. HA maps of all 5 slices in one subject generated by the LRT method and proposed three MOCO methods. More smoothly varying helical structure is observed in proposed MOCO methods.