4650
Using Image Quality Metric to Improve Navigator-based Motion Correction Robustness1Canon Medical Research USA, Inc., Mayfield Village, OH, United States
Synopsis
Keywords: Motion Correction, Motion Correction
Motivation: Navigator-based rigid-body motion correction (MoCo) can improve IQ when the correct motion parameters are extracted from navigator data. However, navigator-based MoCo can reduce IQ when incorrect motion parameters are derived.
Goal(s): We propose combining IQ assessment with navigator-based MoCo to improve correction robustness.
Approach: The proposed solution was implemented by calculating the entropy (IQ metric) of images with/without navigator-based rigid-body MoCo, and MoCo was applied only when the image entropy decreased.
Results: During volunteer studies, the proposed solution reduced the number of slices that showed IQ reduction due to rigid-body correction, while maintaining a large majority of slices that benefited from rigid-body correction.
Impact: Navigator-based rigid-body motion correction (MoCo) robustness was improved by using an image quality metric to determine whether MoCo improved IQ.
Introduction
Patient motion is a major challenge in MRI because of long acquisition times. Autofocus1 and navigator2 based motion correction (MoCo) are two solutions for addressing motion. Autofocus1 iteratively determines the rigid-body motion parameters that provide the best image quality (IQ) according to an IQ metric. However, autofocus is computationally complex and requires long reconstruction times. Navigator-based MoCo can rapidly extract rigid-body motion parameters but can reduce IQ when incorrect parameters are derived. Incorrect parameters can result from a mismatch between the MoCo motion model and the actual motion. Hybrid3 autofocus and navigator-based MoCo has been proposed to improve efficiency of autofocus, but this solution still relies on iteratively determining motion parameters. In this study, we propose combining the IQ metric from autofocus with navigator-based MoCo to enable robust motion correction using only a single iteration.Methods
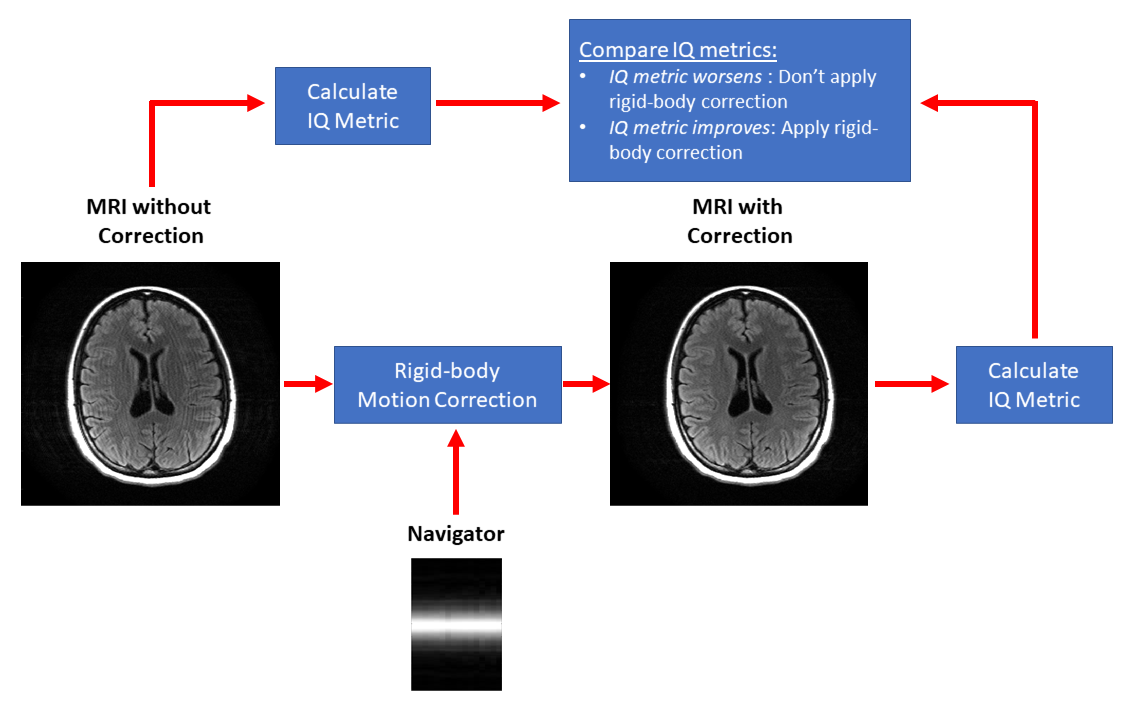
(Theory) IQ metrics can be used to determine whether navigator-based MoCo improves IQ. In a single iteration, an IQ metric can evaluate images before and after MoCo. The MoCo image will only be used if the IQ metric improves (Figure 1). (Implementation) The proposed solution was applied to each individual slice of 2D multi-slice fast-spin echo (FSE2D) imaging as follows: 1) The motion parameters are estimated from RO and PE navigator echoes acquired at the end of each FSE shot. 2) Imaging shots are corrected for translation motion by applying linear phase ramps in k-space. 3) Multi-coil images with/without MoCo are combined using coil sensitivity maps. Simple coil-combination is used for both accelerated (R=2) and non-accelerated (R=1) multi-coil imaging to reduce the proposed solution’s processing time. 4) IQ of coil-combined images before and after MoCo are evaluated with an IQ metric (entropy focus criterion1). 5) MoCo is only applied if the IQ metric improves (i.e., entropy decreases) due to MoCo. Lower entropy corresponds to lower motion artifact level1. (Volunteer studies) The brain and c-spine of 10 volunteers (5 males) were scanned under institutional IRB-approved protocol on Vantage Orian and Vantage Galan 3T clinical MR systems (Canon Medical Systems Corporation, Tochigi, Japan) with FSE2D sequences. Accelerated and non-accelerated FSE2D images with motion artifacts were acquired by asking volunteers to move sporadically during scanning. Accelerated FSE2D images were reconstructed using CG-SENSE, and non-accelerated FSE2D images were coil-combined using coil sensitivity maps. Slices acquired from all volunteers were individually processed with MoCo and visually inspected to determine the number of slices that showed IQ improvements (improved cohort) and IQ reductions (worsened cohort) due to MoCo. Entropy was calculated for with/without correction of both improved and worsened cohorts, and the proposed solution was assessed for its capacity to reduce the number of worsened cohort cases while maintaining the number of improved cohort cases.Results
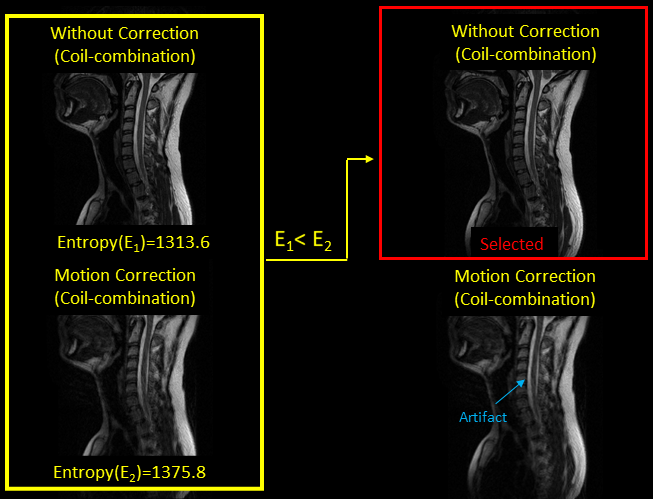
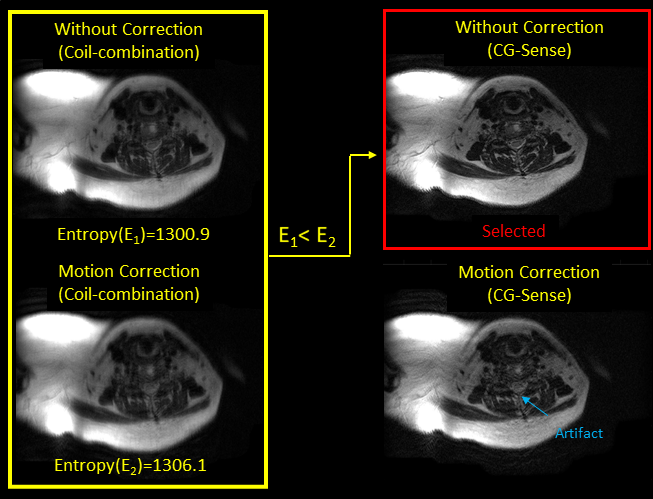
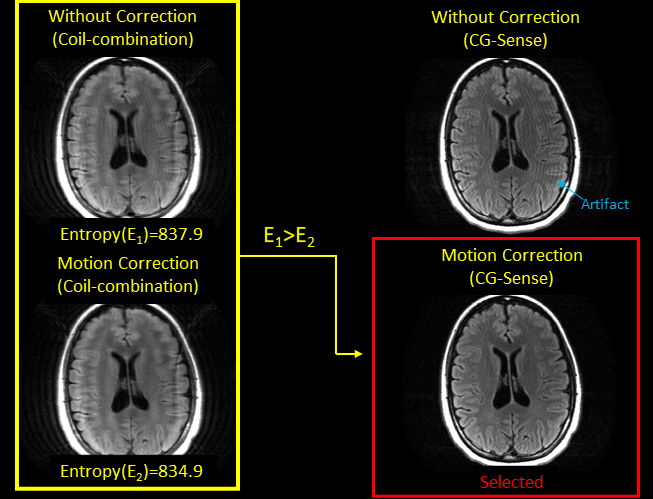
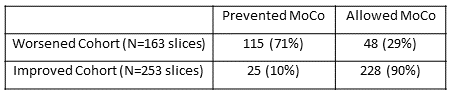
A total of 253 slices showed improved IQ due to MoCo, and a total of 163 slices showed worse IQ due to MoCo. As shown in Table 1, the proposed solution prevented the application of MoCo for 71% (115/163) of the worsened cohort cases, while allowing the application of MoCo for 90% (228/253) of the improved cohort cases. Figure 2 and 3 show examples of proposed solution preventing MoCo for the worsened cohort cases. Figure 4 shows an example of proposed solution allowing MoCo for the improved cohort cases.Discussion
During the volunteer studies, the proposed solution improved the robustness of navigator-based MoCo by reducing the number of slices that showed IQ reduction due to MoCo, while maintaining a large majority of slices that benefited from MoCo. (Limitations) (1) The proposed solution provides only a binary control over navigator-based MoCo (i.e., apply or not apply correction). The solution does not attempt to refine or improve navigator-based MoCo. (2) The solution did not prevent MoCo in all of the worsened cohort slices. (3) The solution did not allow MoCo in all of the improved cohort slices. (Future Direction) More studies are needed to investigate the proposed solution’s performance in additional anatomies. Additionally, studies with large patient cohorts are needed to evaluate the solution’s performance in a clinical setting.Conclusion
This preliminary study showed that combining IQ metric assessment with navigator-based MoCo improves motion correction robustness.Acknowledgements
No acknowledgement found.References
1. Atkinson, D., Hill, D.L., Stoyle, P.N., Summers, P.E., Clare, S., Bowtell, R. and Keevil, S.F., 1999. Automatic compensation of motion artifacts in MRI. Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine, 41(1), pp.163-170.
2. Lin, W., Huang, F., Börnert, P., Li, Y. and Reykowski, A., 2010. Motion correction using an enhanced floating navigator and GRAPPA operations. Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine, 63(2), pp.339-348.
3. McGee, K. P., Felmlee, J. P., Manduca, A., Riederer, S. J., & Ehman, R. L. (2000). Rapid autocorrection using prescan navigator echoes. Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine, 43(4), 583-588.
Figures